SciresolSciresolhttps://jmsh.ac.in/Journal of Medical Sciences and Health10.46347/jmsh.v12.i1.25.98CASE REPORT<p>Pulmonary Nocardiosis with Cutaneous Involvement: A Diagnostic Conundrum</p>303202620261211Abstract
<p><emphasis>Nocardia</emphasis> are soil borne actinomycetes belonging to family Nocardiaceae. These are gram positive and weakly acid-fast organisms causing primary cutaneous, lymphocutaneous, and pulmonary infections in immunocompromised and immunocompetent patients and simulates respiratory pathogens like Mycobacterium tuberculosis. A 31-year-old male, presented with left sided chest pain, fever, cough with expectoration since 2 months and swelling on left side of chest since 1 month, gradually progressing in size. Chest X-ray showed minimal left sided pleural effusion. Ultrasonography and HRCT showed lesion of size 3.7x3.3cm with patchy focal subpleural area of consolidation in inferior segment of lingula with adjacent perichondral soft tissue thickening suggestive of infective etiology like Koch’s. On past history, patient was on chronic steroid therapy for Upper motor neuron-type paraparesis suggestive of long segment transverse myelitis. FNAC showed chronic inflammatory lesion with reparative changes with no AFB seen. Modified ZN stain showed meshworks of long, thin partially acid-fast filaments indicating <emphasis>Nocardia</emphasis> species. Xpert MTB was negative for <emphasis>Mycobacterium tuberculosis</emphasis>. Patient was finally diagnosed as a case of Pulmonary Nocardiosis and was treated with Inj. Septran and Inj. Amikacin for 4 weeks and treatment for 6 months. The chest abscess was resolved within 4 weeks. <emphasis>Nocardia</emphasis> are slow growing in culture and can be misdiagnosed as TB if not investigated thoroughly. In such a scenario, the direct gram stain and modified ZN stain can provide a rapid diagnosis to help initiate empirical therapy.</p>
KeywordsPulmonary Nocardiosis<I>Nocardia</I> speciesAcid- Fast StainingChest AbscessFine needle Aspiration Cytology (FNAC)Nocardiosis diagnosisAcid-Fast BacilliNocardial PneumoniaCotrimoxazole treatmentSteroid-induced infectionChadhaVasudha1 Junior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra India Associate Professor, Department of Pathology Government Medical College Nagpur, Maharashtra India Senior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra IndiaGolharVedita Bobde2 Junior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra India Associate Professor, Department of Pathology Government Medical College Nagpur, Maharashtra India Senior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra IndiaPawarPriya3 Junior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra India Associate Professor, Department of Pathology Government Medical College Nagpur, Maharashtra India Senior Resident, Department of Pathology Government Medical College Nagpur, Maharashtra IndiaIntroduction
Nocardia species are soil-borne actinomycetes belonging to the family Nocardiaceae. They are gram-positive, weakly acid-fast organisms known to cause primary cutaneous, lymphocutaneous, and pulmonary infections in both immunocompromised and immunocompetent individuals. The clinical diagnosis of pulmonary nocardiosis remains challenging, and reported cases are relatively few. It represents a rare yet increasingly recognized bacterial infection with a high potential for misdiagnosis due to its clinical overlap with other respiratory pathogens, including other actinomycetes and Mycobacterium tuberculosis[1]. As a result, it contributes substantially to morbidity and mortality, particularly among immunocompromised patients. Here, we describe a rare presentation of pulmonary nocardiosis
with extension to the overlying skin in a patient receiving prolonged steroid therapy for transverse myelitis.
Case History
A 31-year-old male computer engineer presented with a two-month history of left-sided chest pain, intermittent fever, and productive cough, accompanied by a progressively enlarging, soft, non-tender chest-wall swelling of one month’s duration. There was no antecedent trauma, and the overlying skin exhibited no abnormality. Six months prior, he had developed insidious-onset upper motor neuron–type paraparesis with early bladder–bowel involvement. MRI findings were consistent with a non-compressive intramedullary long-segment transverse myelitis, for which he received pulse methylprednisolone followed by high-dose oral Wysolone. Chest radiography demonstrated minimal left pleural effusion. Ultrasonography revealed a 3.7 × 3.3 cm hypoechoic lesion at the sixth intercostal space, suggestive of an abscess. HRCT showed subpleural lingular consolidation with adjacent perichondral soft-tissue thickening and a focal collection, raising suspicion for an infectious process. FNAC displayed chronic inflammatory changes without granulomas, necrosis, acid-fast bacilli, or fungal elements; Xpert MTB/Rif Ultra
was similarly negative. In view of persistent diagnostic ambiguity, a modified Ziehl–Neilsen stain was performed and revealed long, thin, partially acid-fast filaments consistent with Nocardia. A definitive diagnosis of pulmonary nocardiosis with associated chest-wall abscess was established. The patient received intravenous Septran and amikacin for four weeks, resulting in substantial symptomatic resolution.
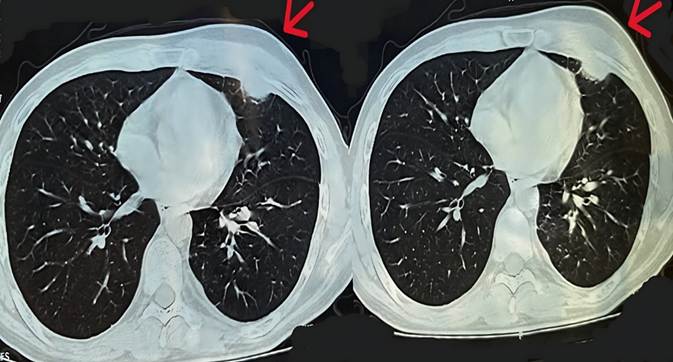
Fig. 1: Clinical picture of 31 year old male presenting with anterior chest wall swellingFig. 2: HRCT chest suggestive of subpleural consolidation with infective etiology. Arrows show cutaneous soft tissue involvement with underlying subpleural foci of consolidationDiscussion
Nocardia species are aerobic, gram positive, weakly acid‑fast, catalase‑positive organisms showing fine right‑angled branching filaments. They are saprophytic bacteria which live in carbon‑rich sources like soil, decomposing organic matter and aquatic environment. N. otitidiscaviarum is capable of causing pulmonary infections involving pleura in a debilitated host[2]. There are more than ninety Nocardia species that have been known to cause disease in humans[3].
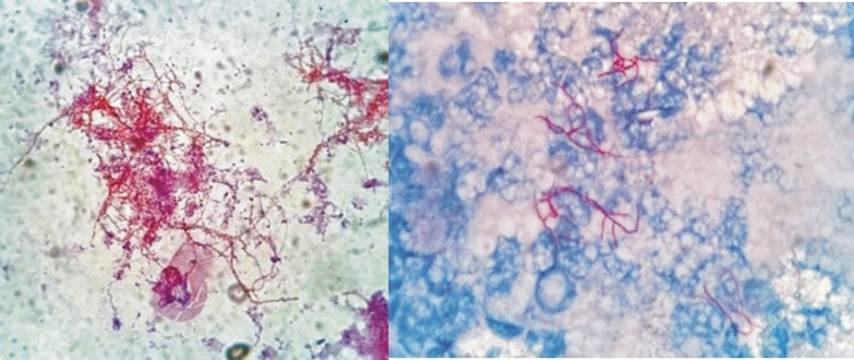
Fig. 3: Image on the left: Oil immersion field (100x): Gram staining showing gram-positive, thin, filamentous bacilli. Image on the right: Oil immersion field (100x): Modified Ziehl- Neilsen stain applied using 1% Sulfuric acid showing thin, filamentous acid- fast organisms suggestive of Nocardial Infection
Certain risk factors like old age, malignancies, diabetes mellitus, chronic pulmonary diseases, alcoholism, medical immunosuppression, high dose steroids, organ transplants etc. play an important role in promoting the causation of nocardiosis. The most common site of infection is the lung because the major route of exposure being inhalation, followed by skin and soft tissue, brain, joints or bones.
Pulmonary nocardiosis may present as an acute, subacute or chronic disease, with exacerbations and sometimes remissions. Symptoms like fever, cough, breathlessness, hemoptysis, and weight loss are often diagnosed as tuberculosis or community‑acquired pneumonia. It may also mimic fungal pneumonia. Clinical manifestations include Endobronchial inflammatory masses, pneumonia, lung abscess, pleural effusion, empyema, and cavitary disease with contiguous extension to underlying deep structures[4]. In our case, the patient was on high dose steroids for transverse myelitis which made him more prone for this infection.
As neither the CT or chest radiography is pathognomonic of pulmonary nocardiosis, the definitive diagnosis of Nocardiosis requires smear and culture of appropriate samples, like sputum and pus[5]. In this case, the laboratory should always be notified about its suspicion for proper diagnosis and recovery. Sequence analysis of the 16S rRNA gene has become the "gold standard" for speciation of Nocardia in recent times[6]. Fine needle aspiration cytology material is the crucial investigation in identifying the infection at sites that are easily amenable for aspiration. Gram staining of the FNAC material aids in presumptive diagnosis of Nocardia[7, 8].
The burden of pulmonary nocardiosis seems to be highly underestimated. The disease should always be considered in the differential diagnosis of pneumonia, not only in the immunocompromised, but also in the immunocompetent, especially when they are not responding to the standard therapy. In tuberculosis endemic countries like India, nocardiosis should always be excluded among patients not responding to anti‑tubercular treatment.
Early recognition and appropriate individualized treatment is the key to a successful outcome in these cases. Cotrimoxazole is still the drug of choice in the treatment of nocardial infection followed by Amikacin, imipenem, ceftriaxone, minocycline, levofloxacin, linezolid, and amoxicillin‑clavulanic acid in combinations[9]. Duration of the treatment depends on severity of the disease, usually lasting for usually 6–12 months[10].
Conclusion
Pulmonary nocardiosis should be considered in steroid-treated, immunocompetent patients with pneumonia. Because Nocardia grow slowly, they may be mistaken for tuberculosis. While speciation needs biochemical and molecular tests, modified acid-fast and Gram stains on cytology aspirates offer rapid clues for early empirical therapy.
References
Baburao A, Prasad S, Prakash S, Narayanswamy H
Pulmonary nocardiosis: Report of two cases from a tertiary care hospitalIndian Journal of Pathology and Microbiology2019621https://doi.org/10.4103/ijpm.ijpm_793_17
Deepa R, Banu ST, Jayalakshmi G, Parveen JD
Pleuropulmonary nocardiosis due to <I>Nocardia otitidiscaviarum</I> in a debilitated hostIndian Journal of Pathology and Microbiology2016592https://doi.org/10.4103/0377-4929.182011
Özen Y, Dokuzoguz B, Mumcuoglu I, Çelikbas AK, Karahan ZC, Özbay BO
Disseminated <I>Nocardia farcinica</I> infection presenting as a paravertebral abscess in a patient with systemic lupus erythematosusIndian Journal of Pathology and Microbiology2019622https://doi.org/10.4103/ijpm.ijpm_178_17
Aggarwal D, Garg K, Chander J, Saini V, Janmeja AK
Pulmonary nocardiosis revisited: A case seriesLung India2015322https://doi.org/10.4103/0970-2113.152638
Ravi D, Bhat V, Balakrishnan C
Pulmonary nocardiosis: a case report of a rare diagnostic infection complicating <I>Pemphigus vulgaris</I>CHEST20231644https://doi.org/10.1016/j.chest.2023.07.840
Pelaez AI, Garcia Suarez Mdel M, Manteca A, Melon O, Aranaz C, Cimadevilla R, <I>et al</I>
A fatal case of <I>Nocardia otitidiscaviarum</I> pulmonary infection and brain abscess: Taxonomic characterization by molecular techniquesAnnals of Clinical Microbiology and Antimicrobials200981https://doi.org/10.1186/1476-0711-8-11
Chawla K, Mukhopadhyay C, Payyanur P, Bairy I
Pulmonary nocardiosis from a tertiary care hospital in Southern IndiaTropical Doctor2009393https://doi.org/10.1258/td.2008.080229
Ramamoorthi K, Pruthvi BC, Rao NR, Belle J, Chawla K
Pulmonary nocardiosis due to <I>Nocardia otitidiscaviarum</I> host- A rare case reportAsian Pacific Journal of Tropical Medicine201145https://doi.org/10.1016/s1995-7645(11)60116-8
Park SD, Kim HJ, Jang IH, Uh Y, Kim J, Yoon KJ, <I>et al</I>
First Report of <I>Nocardia farcinica</I> Bursitis in a Patient with Diabetes MellitusAnnals of Laboratory Medicine2014343https://doi.org/10.3343/alm.2014.34.3.252