SciresolSciresolhttps://jmsh.ac.in/Journal of Medical Sciences and Health10.46347/jmsh.v12.i1.25.134CASE REPORT<p>Extracranial Metastases of Glioblastoma to Parotid Gland: A rare Case Report</p>303202620261211Abstract
<p>Glioblastoma is the most aggressive intracranial tumor and diffusely infiltrates the surrounding brain tissue. Extra cranial metastasis of Glioblastoma is extremely rare. Here, we report a case of extra-cranial metastasis of left frontal lobe Glioblastoma to the ipsilateral side of parotid gland in a 47 year old male patient who presented with multiple nodular lesions of the parotid gland. Till date there have been only 13 reported cases of Glioblastoma metastases to parotid gland in literature. Initial presumptive cytological diagnosis of metastasis was made by USG guided FNAC of the parotid gland. Histopathological and Immunohistochemistry analysis aided in the confirmatory diagnosis of extracranial metastasis of Glioblastoma. We report this case to emphasize the need for rigorous follow-up, including magnetic resonance imaging of the head and neck region with a higher index of suspicion of recurrence/metastases and advancements in adjuvant treatment.</p>
KeywordsExtracranial metastasisGlioblastomaParotid glandNarayanHemavathi1 Assistant Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Associate Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Assistant Research Scientist Kidwai Memorial Institute of Oncology Bengaluru DharmalingamPriya2 Assistant Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Associate Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Assistant Research Scientist Kidwai Memorial Institute of Oncology Bengaluru AkshathaC2 Assistant Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Associate Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Assistant Research Scientist Kidwai Memorial Institute of Oncology Bengaluru AlashettySoumya1 Assistant Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Associate Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Assistant Research Scientist Kidwai Memorial Institute of Oncology Bengaluru NarayanaNavyashree Hosahalli3 Assistant Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Associate Professor, Department of Pathology Kidwai Memorial Institute of Oncology Bengaluru Assistant Research Scientist Kidwai Memorial Institute of Oncology Bengaluru Introduction
Glioblastoma (GB) is one of the most aggressive neoplasms that arise from glial elements in the central nervous system (CNS)[1]. It accounts for 14.3% of all primary CNS tumors with 49.1% o in adults and 2.2% in children. It affects men more frequently than women (1.6:1). With a peak incidence between the ages of 75 and 84, it is more prevalent in older persons over the age of 55[2]. It infiltrates into nearby brain tissue, spreads along white matter tracts, direct extension, and subarachnoid dissemination in addition to intracranial metastases to the meninges or spinal cord[3].Extracranial metastases extremely rare, occurring in only 0.2-2.7 % of all patients with glioblastoma[4]. The most common sites of extracranial metastases includes lungs and pleura (60%), lymph nodes (51%), bone (31%) and liver (22%), with rare reports to skin (6%), parotid gland (13%) and other organs[3, 4].It has a poor prognosis with 5 year survival rate of only 6.8%[2].
Case Report
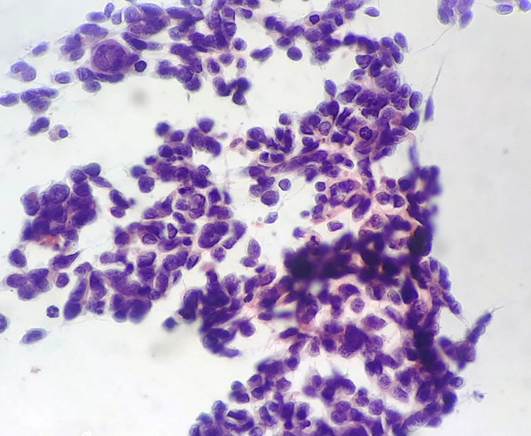
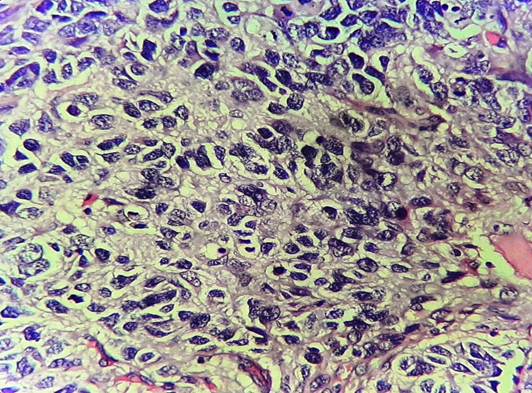
A 47 year old male patient, known case of Glioblastoma, NOS, and Isocitrate Dehydrogenase (IDH) wild type of the left frontal lobe, had underwent surgical resection, radiation therapy, and adjuvant chemotherapy of temozolomide (4 cycles completed). One year following surgery, the patient now observed a swelling in his left side of face. Local examination revealed a 2x1.5cm hard and tender nodule over the left parotid region and a palpable left level II cervical lymph node. Magnetic resonance imaging (MRI) of the brain revealed an ill defined cavity measuring 5.5x3.4cm in the left frontal lobe of the neuroparenchyma with a possibility of residual disease. MRI of head and neck showed multiple heterogenous nodular lesions of the left parotid gland, largest measuring 23x15mm. An enlarged left level II cervical lymph node measuring 23x14 mm was also noted. Differentials were metastasis and primary parotid neoplasm. However, FNAC correlation was done. Cytology smears were highly cellular comprising of pleomorphic tumour cells with enlarged hyperchromatic nucleus and scant cytoplasm. Few cells had spindled morphology. Vague rosetting pattern with fibrillary matrix material was evident. Atypical mitosis was noted. Metastatic High Grade Glioma (in a known case of Glioblastoma) was established by cytology [Fig. 1]. Material for cell block study was not available, so biopsy was done and sent for histopathological examination. Microscopic examination showed a malignant neoplasm composed of medium to large sized tumour cells with hyperchromatic nucleus and scant clear cytoplasm
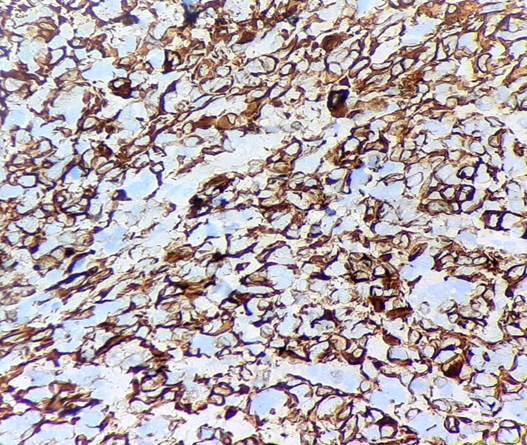
arranged in discrete nodules and focally in rosette like pattern. [Fig. 2]. It was further subjected to IHC testing. The neoplastic cells were positive for Glial fibrillary acidic protein (GFAP) and S-100, thus confirming the diagnosis of Metastatic Glioblastoma [Fig. 3]. ATRX nuclear expression was retained in the tumour cells. Nuclear p53 showed mutant positivity (>70%) and IDH-1 mutant protein is negative in tumour cells.
Fig. 1:Highly cellular cytological smear shows a neoplasm composed of large pleomorphic round tumour cells arranged in loosely cohesive clusters (pap stain, x400)
Fig. 2:Photomicrograph shows tumour cells with enlarged hyperchromatic nucleus and scant clear cytoplasm, and few bizarre mitotic figures seen (H & E, x400)
Fig. 3: Immunohistochemistry showing positivity for Glial fibrillary acidic protein [GFAP] (IHC, x 400)
Discussion
Glioblastoma is a grade IV diffuse glioma and the most common cerebral tumor in adults[2]. Despite standard debulking surgical treatment, followed by radiotherapy and chemotherapy, Glioblastoma are extremely malignant primary brain tumours with a median survival of 15 months[5].According to new research, testing for Isocitrate Dehydrogenase (IDH) mutation and 1p/19q co-deletion is now required. Based on these mutations, Glioblastoma was divided into two subtypes: IDH-wildtype (90%) and IDH-mutant (10%)[6]. Extra cranial metastases are extremely rare with incidences between 0.2 and 2.7% due to the poor prognosis resulting in a very short survival and eliminates the chances of detection of metastasis from Glioblastoma[4]. Cervio et al. proposed three potential mechanisms for the extra-neural spread of Glioblastoma, even if the precise process of extra-neural metastases has not yet been fully understood - 1) Lymphatic invasion: the drainage of cerebrospinal fluid into extraneural tissue (despite the lack of a true lymphatic system in the CNS); 2) Venous invasion: either through the leptomeningeal sinuses or the intracerebral vein; 3) Direct invasion through the dura and bone or through tumour cell migration along the ventriculoperitoneal shunts[7]. The physical disruption of the blood-brain barrier, as well as scalp metastasis near a craniotomy, leptomeningeal spread to the spine, metastases to lymph nodes, metastases to the abdomen via ventriculoperitoneal shunt, and seeding along the biopsy tract, have all been documented with regard to these pathophysiological theories. The lungs, heart, pleura, liver, and bone marrow have all been reported as sites of glioblastoma extracranial metastases[8, 9]. It is still unclear how exactly Glioblastoma spread to the parotid gland. Nguyen et al. reported subgaleal metastases on the contralateral side, which can be an indicator for possibly local vascular invasion of tumour cells, despite the fact that other authors believed tumour seeding to be a natural result to nearby tissues close to the surgical site[10]. The central nervous system venules of the dura mater, which have thin walls and insufficient support, may also allow for metastatic spread, according to Willis' theory[11]. Till date, our case can be considered as the 14th case of parotid gland metastases of Glioblastoma. The interval between the Glioblastoma's diagnosis and its spread to the parotid gland was 9.2 months on average, which is nearly equal to the interval between extracranial metastases to other organs[4]. Cervical Lymphnodal metastases from CNS tumors is infrequent. Ates et al. and Mujtaba et al., had immunohistochemically proven cases of Glioblastoma metastases to nodal sites. Cervical lymph nodes were noted as the area of concomitant metastasis which supports pathophysiological theory[12, 13]. Our patient had ipisilateral cervical lymph node enlargement at the time of extraneural metastatic manifestation which led us to believe that the lymphatic system may be the primary route of extraneural metastasis. Thus, the only diagnostic tool for exact typing of the tumour is Histopathological examination supported by Immunohistochemistry. More documented reports will improve our understanding and raise our index of suspicion of extra cranial metastases of Glioblatoma. After the onset of metastatic disease, survival remains dismal. Palliative radiation therapy is the best available option for patients with disseminated metastatic disease.
Conclusions
Close imaging follow-up is extremely important due to the intracranial Glioblastoma's propensity for recurrence and its malignant character. Correlation with Ultrasound-guided FNA with Histopathological and Immunohistochemistry analysis provides a confirmatory diagnosis of extra cranial metastases of Glioblastoma to the parotid gland. The practice of autopsies in oncologic patients should be encouraged, and its studies may allow for the determination of more accurate data in pathogenesis and behavior in neoplastic/complex metastatic disease mechanisms.
References
Zhen L, Yufeng C, Zhenyu S, Lei X
Multiple extracranial metastases from secondary glioblastoma multiforme: a case report and review of the literatureJournal of Neuro-Oncology2010973https://doi.org/10.1007/s11060-009-0044-9
Quinn T Ostrom, Gino Cioffi, Kristin Waite, Carol Kruchko, Jill S Barnholtz-Sloan
CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018Neuro-Oncology202123Supplement_3https://doi.org/10.1093/neuonc/noab200
Romero-Rojas AE, Diaz-Perez JA, Amaro D, Lozano-Castillo A, Chinchilla-Olaya SI
Glioblastoma Metastasis to Parotid Gland and Neck Lymph Nodes: Fine-Needle Aspiration Cytology with Histopathologic CorrelationHead and Neck Pathology201374https://doi.org/10.1007/s12105-013-0448-x
Baskurt O, Kurtulus Y, Yavuz AY, Avci I
Extracranial metastasis of recurrent glioblastoma to the parotid gland: a case report and review of the literatureEgyptian Journal of Neurosurgery2022371https://doi.org/10.1186/s41984-022-00163-z
Alexander BM, Cloughesy TF
Adult GlioblastomaJournal of Clinical Oncology20173521https://doi.org/10.1200/jco.2017.73.0119
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, <I>et al</I>
The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summaryActa Neuropathologica20161316https://doi.org/10.1007/s00401-016-1545-1
Cervio A, Piedimonte F, Salaberry J, Alcorta SC, Salvat J, Diez B, <I>et al</I>
Bone Metastases from Secondary Glioblastoma Multiforme: A Case ReportJournal of Neuro-Oncology2001522https://doi.org/10.1023/a:1010629618859
Yokoyama H, Ono H, Mori K, Kishikawa M, Kihara M
Extracranial metastasis of glioblastoma with sarcomatous componentSurgical Neurology1985246https://doi.org/10.1016/0090-3019(85)90122-3
Nguyen B, Samara J, Lee A, Fadia M, Ngu C, Pranavan G
A case of subgaleal metastasis from glioblastoma multiformeInternal Medicine Journal2018486https://doi.org/10.1111/imj.13818The Spread of Tumours in the Human BodyPostgraduate Medical Journal195329329https://doi.org/10.1136/pgmj.29.329.160
Ates LE, Bayindir C, Bilgic B, Karasu A
Glioblastoma with lymph node metastasesNeuropathology2003232https://doi.org/10.1046/j.1440-1789.2003.00490.x