Gall stone associated biliary tract disease is not an uncommon surgical condition presenting during pregnancy. Such patients may require invasive procedures due to repeated attacks of biliary colic, acute cholecystitis, choledocholithiasis, cholangitis, or gallstone pancreatitis. Acute cholecystitis continues to be the second most common non-obstetrical indication for surgery in pregnant women after acute appendicitis
The main risks of surgery during pregnancy are foetal loss, premature labour and delivery, which can result
from both, the disease process itself and the intervention. Intra-abdominal procedures for inflammation immediately adjacent to the uterus are more likely to result in uterine irritability and the risk of preterm labour or abortion. The anaesthesiologist must provide safe anaesthesia to the mother while minimizing the risks to the developing foetus
We hereby report two patients presenting with cholecystitis and cholelithiasis, in various stages of pregnancy, for two different procedures, laparoscopic cholecystectomy and ERCP.
A 33-year Gravida Two Para One patient with fifteen weeks of gestation presented with complaints of abdominal pain and high coloured urine for four days. She underwent lower segment caesarean section five years ago under spinal anaesthesia. An ultrasound abdomen revealed cholelithiasis and she was posted for laparoscopic cholecystectomy.
An obstetric consultation was obtained, and she was advised injection Progestin (progesterone) 250 mg intramuscularly prior to surgery and Hydroxyprogesterone Hexanoate (Capsule Susten SR 200 mg- oral progesterone tablets) twice a day for two weeks post operatively. The patient was counselled by a team of obstetricians, gastro-intestinal surgeons, anaesthesiologists and appropriate consents were obtained for both anaesthesia and surgery.
The patient was advised nil by mouth for 8 hours prior to surgery. A wedge was placed below the patient's right hip before induction. All standard American Society of Anaesthesiologists (ASA) monitors were connected. The patient was induced with Injection Fentanyl 2 mcg/kg and Injection Propofol 2 mg/kg i.v. Muscle relaxation was achieved with Injection Rocuronium 1.2 mg/kg. The airway was secured with size 7.0 cuffed endotracheal tube and connected to the ventilator using volume control mode of ventilation with the following settings, a tidal volume of 450 ml, respiratory rate of 14/min and an I:E ratio of 1:2. Anaesthesia was maintained with Sevoflurane, titrated to a Minimal Alveolar concentration of 1, with oxygen and air at a ratio of 50:50. Injection morphine 4 mg i.v. and acetaminophen 1 g i.v. was administered as analgesia. The surgery lasted for 1 hour and 45 minutes. She received 1000 ml of normal saline as intravenous fluids and the urine output was 200 ml. The blood loss was approximately 100 ml. Post the procedure the effect of the muscle relaxant was reversed with injection neostigmine 2.5 mg and glycopyrrolate 0.4 mg and she was extubated when she was completely awake demonstrating intact muscle tone. She was discharged on the second post-operative day with no maternal or foetal compromise. Her post-operative course was uneventful. She was found to have no more symptoms of biliary colic post-surgery.
A 33-year-old primigravida with 30 weeks gestation, presented with repeated episodes of pain abdomen and vomiting. Ultrasound abdomen showed dilated CBD with multiple calculi; however liver function tests were normal. She had three episodes of pain abdomen during the course of pregnancy, which was managed conservatively. In view of recurrent episodes of pain abdomen and vomiting she was scheduled for endoscopic retrograde cholangio-pancreaticography (ERCP).
A thorough pre-anaesthetic evaluation was done. She had no other comorbid conditions. An obstetrician opinion was sought regarding the foetal well-being. Foetal heart rate was recorded, and non-stress test (NST) was performed which was reassuring. The risks of general anaesthesia for ERCP including foetal loss, positioning related issues and risk of aspiration were discussed in detail with the patient and her husband and written informed consent was obtained.
All standard ASA monitors were connected, Routine general anaesthesia with rapid sequence induction was performed using Injection propofol titrated to effect and Injection Rocuronium 1.2 mg/kg i.v. was used as a muscle relaxant. Injection Fentanyl 2 mcg/kg i.v. was used as an analgesic. The airway was secured with size 7.0 cuffed endotracheal tube and connected to the ventilator. Anaesthesia was maintained with Sevoflurane at a MAC of 1 with oxygen and air at a ratio of 50:50. The duration of the ERCP was 45 minutes.
The ERCP was performed in the left lateral position after discussion with the Gastroenterologist. A lead shield was applied over the abdomen to minimize radiation exposure to the foetus. The procedure was uneventful. She received 500 ml of intravenous fluids (Normal Saline).
Post the procedure, she was reversed with Injection Neostigmine 2.5 mg i.v and Glycopyrrolate 0.4mg i.v. and extubated when she demonstrated intact airway reflexes and intact muscle tone. The foetal non stress test was reassuring post the procedure. She was discharged on the second post-operative day with no maternal or foetal compromise. On following up the course of pregnancy, we were informed that she had delivered a healthy male baby at 37 weeks.
The American College of Obstetricians and Gynaecologists and the American Society of Anaesthesiologists guidelines for non-obstetric surgery during pregnancy are as follows
1. Surgery on a pregnant woman should never be delayed or denied regardless of trimester because this can adversely affect the pregnant woman and her foetus.
2. Elective surgery should be postponed until after delivery.
3. Given the potential for preterm delivery with some non-obstetric procedures during pregnancy, corticosteroid administration for foetal benefit should be considered for patients with foetuses at viable pre-mature gestational ages, and patients should be monitored in the perioperative period for signs or symptoms of preterm labour.
4. Pregnant women undergoing non-obstetric surgery should be screened for the risk of venous thromboembolism and should have the appropriate perioperative prophylaxis administered.
In providing safe anaesthesia for non-obstetric surgery during pregnancy, one must consider the requirement of balancing the safety of two patients together, the mother and the foetus. This necessitates a thorough understanding of the maternal physiological and pharmacological changes occurring during pregnancy, avoiding potentially harmful drugs during foetal development, ensuring adequate uteroplacental perfusion and avoidance of or treatment of preterm labour and delivery.
Maintenance of maternal oxygenation, perfusion and homeostasis with optimal anaesthesia for the patient will assure the most favourable outcome for the foetus
Under usual circumstances, surgery is indicated only when it is absolutely necessary for the safety of either the mother, foetus, or both. The foremost common indications being acute appendicitis, cholecystitis, trauma, and surgery for maternal malignancies.
The main risks of surgery during pregnancy are foetal loss, premature labour, and delivery, which can result from both the pathological process itself and the intervention. Intra-abdominal procedures for inflammation immediately adjacent to the uterus are more likely to result in uterine irritability, and the risk of preterm labour or abortion is significantly higher
The timing of surgery plays a crucial part in determining the outcome of surgery and the safety of both the mother and developing foetus. The decision for surgery should always be by a team decision comprising of the operating surgical team, the anaesthesiologist and the obstetrician. In a largest single series concerning surgery and anaesthesia during pregnancy, 42% of surgery during pregnancy occurred during the first trimester, 35% during the second trimester, and 23% during the third
Surgery and anaesthesia can adversely affect the outcome of pregnancy depending on the gestational age. Loss of pregnancy can vary depending from an average of 5.8% to as high as 10% during the first trimester. During the period of organogenesis which lies between the third to the eighth week, teratogens may produce major organ abnormalities. Drug exposure after this period may either cause growth retardation or functional changes as against structural abnormalities. In advanced pregnancy, the focus will be related to manoeuvring the gravid uterus away from contributing to aorto-caval compression and concerns related to difficult airway seen in pregnancy
Gall stone disease, though infrequently associated with pregnancy requires therapeutic intervention at the earliest. The incidence of gallstones during pregnancy is estimated to be between 3% and 12%
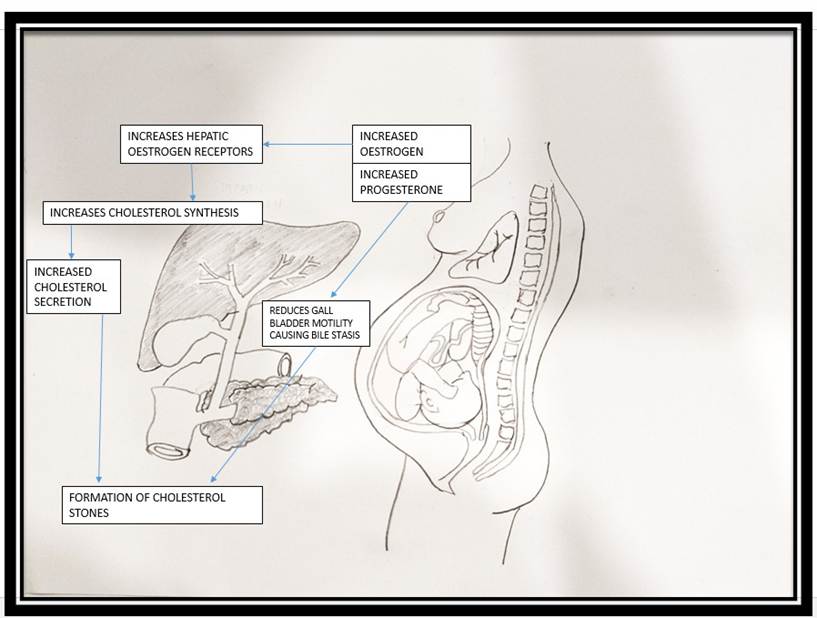
The physiological weight gain of pregnancy associated with hormonal changes predisposes a pregnant woman to biliary sludge and gall stone formation. The altered oestrogen and progesterone during pregnancy contributes to increased bile lithogenicity with delayed emptying of the gall bladder
Laparoscopic surgery once considered contraindicated during pregnancy has become the standard of care irrespective of the gestational age. Laparoscopic surgery being minimally invasive, offers added benefits as compared to open surgery such as reducing the risk of foetal loss. It also offers a better maternal safety profile with early recovery and minimum morbidity.
Endoscopic retrograde cholangiopancreatography (ERCP) has become the most common treatment modality for symptomatic choledocholithiasis. Mitchell S Cappell et al.
The second trimester happens to be the most ideal period for therapeutic intervention during pregnancy. Interventions after the 12th week offer the best period for intervention as it is well past the phase of organogenesis and the incidence of spontaneous abortions are also minimal. Similarly, although ERCP can be safely performed during all trimesters of pregnancy, the second trimester happens to be the most suited with a very low rate of foetal loss. As the pregnancy advances into the third trimester, the positioning of the patient becomes a concern. This is due to the effect of aortocaval compression. Direct injury to the large gravid uterus may occur during the procedure and access to the gall bladder fossa may be obstructed. The ERCP is better accomplished either in the left lateral position or supine position.
Maternal haemodynamic changes due to raised intra-abdominal pressure from the pneumoperitoneum could decrease utero-placental perfusion leading to foetal hypoxia.
Iatrogenic mechanical insult to the gravid uterus and foetus, including preterm delivery, foetal loss, abortion, uterine rupture and direct or indirect foetal injuries.
Maternal and Foetal Acidosis from absorption of carbon-dioxide used to insufflate the abdomen during the laparoscopy.
Initial abdominal access can be safely accomplished with an open technique, Veress needle, or optical trocar technique. A modification of the initial trocar placement may be necessary depending on the size of the gravid uterus.
Intra-abdominal pressure is to be maintained between 8 - 12 mm of Hg and should not exceed 15 mm of Hg to avoid reduction in uterine blood flow. The insufflation pressures should be adjusted to maintain stable patient haemodynamics.
EtCO
Intraoperative and postoperative pneumatic compression devices and early postoperative ambulation are recommended to avoid deep venous thrombosis in the gravid patient. Pharmacologic thromboprophylaxis should be added for procedures lasting more than 1 hr.
Foetal Heart Rate should be monitored in all patients with a gestational age greater than 22 to 24 weeks and documented immediately prior to and at the end of the procedure.
There is no evidence to support the routine use of tocolytic drug to inhibit uterine activity and preterm labour, but should be considered perioperatively when signs of preterm labour are noted, in consultation with the obstetrician. The only effective measure that reduces the risk of premature uterine contraction, is by minimizing the manipulation of the uterus. Similarly, there is no role of prophylactic corticosteroids.
Our first patient was a second-gravida who presented with acute cholecystitis with cholelithiasis during the 15th week of gestation. In view of her acute symptoms, the gastrointestinal surgeon and obstetrician decided to proceed with laparoscopic cholecystectomy, adhering to standard guidelines. Our second patient presented with recurrent episodes of acute cholecystitis with choledocholithiasis and did not respond to conservative management. She underwent a successful ERCP, went on to complete term gestation and delivered a healthy male baby at 37 weeks gestation.
Anaesthesia for non-obstetric surgery during pregnancy presents its own challenges. Ensuring maternal and foetal wellbeing during the perioperative period necessitates a thorough understanding of the maternal physiological changes and the unique and varied requirement of different surgical procedures which they may be scheduled for.
Biliary disease during pregnancy although rare, happens to be one of the common conditions for which therapeutic intervention may be needed during pregnancy. Safe anaesthesia and perioperative care can be provided taking into consideration these following issues
(i) Optimize and maintain normal maternal physiological function;
(ii) Optimize and maintain utero-placental blood flow and oxygen delivery;
(iii) Avoid undesired drug effects on the foetus;
(iv) Avoid unwarranted uterine stimulation;
(v) Avoid awareness during general anaesthesia.
Adhering to the above principles will ensure a favourable outcome to the mother, the foetus and the healthcare personnel involved in the care of the case.