SciresolSciresolhttps://jmsh.ac.in/Journal of Medical Sciences and Health10.46347/jmsh.v12.i2.25.277CASE REPORT<p>Spiegler-Fendt Sarcoid: A Case Report</p>303202620261221Abstract
<p>A 79-year-old male presented with pruritic erythematous papules and plaques on chest and upper back of 2 weeks duration, along with history of bilateral enlarged cervical lymph nodes for 1 month. Skin biopsy showed dense interstitial lymphohistiocytic infiltration and occasional plasma cell infiltration consistent with Spiegler-Fendt Sarcoid (Lymphocytoma Cutis), while lymph node biopsy confirmed concurrent Angioimmunoblastic T-cell Lymphoma (AITL). The patient showed excellent response to methotrexate and narrowband UVB therapy for cutaneous lesions alongside chemotherapy for AITL. This rare case highlights the diagnostic challenges in distinguishing benign pseudolymphoma from malignant lymphoma and emphasizes the importance of comprehensive evaluation in atypical presentations. The concurrent occurrence of these conditions in an elderly male expands the known demographic spectrum of Spiegler-Fendt Sarcoid.</p>
KeywordsSpiegler-Fendt SarcoidLymphocytoma CutisCutaneous PseudolymphomaAngioimmunoblastic T-cell LymphomaChikaraddiBhavani1 Post Graduate, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Professor & HOD, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Senior Resident, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka IndiaSanjanaA S2 Post Graduate, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Professor & HOD, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Senior Resident, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka IndiaDheemantM3 Post Graduate, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Professor & HOD, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Senior Resident, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka IndiaRathodPushpavathi1 Post Graduate, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Professor & HOD, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka India Senior Resident, Department of Dermatology, Venereology & Leprosy BGS Global Institute of Medical Sciences Bengaluru, Karnataka IndiaIntroduction
Cutaneous lymphoid infiltrates include a wide range of dermatological conditions, from benign inflammatory reactions to malignant lymphoproliferative disorders [1]. One of the benign types is lymphocytoma cutis, also referred to as Spiegler-Fendt sarcoid or cutaneous pseudolymphoma [2]. It is a chronic inflammatory condition marked by localized, dense lymphocytic infiltrates in the dermis. It usually presents as solitary or grouped erythematous papules, plaques or nodules, commonly affecting the face, trunk or upper limbs. Both clinically and on histopathology, lymphocytoma cutis can closely resemble cutaneous lymphomas, particularly cutaneous B-cell lymphoma, making it difficult to differentiate without immunohistochemical analysis and clinical correlation [3].
Angioimmunoblastic T-cell lymphoma (AITL) is an aggressive and a rare form of peripheral T-cell lymp- homa. It arises from follicular helper T-cells and commonly presents with generalized lymphadenopathy,
hepatosplenomegaly, fever, weight loss, night sweats, along with polyclonal hypergammaglobulinemia and immune dysfunction. AITL accounts for about 15–20% of peripheral T-cell lymphomas and 1–2% of all non-Hodgkin lymphomas [4]. Skin involvement is seen in up to half of the patients, and may appear before, during or after the onset of systemic symptoms. These skin lesions are often non-specific macules, papules, plaques or nodules and can resemble benign skin conditions, which may delay diagnosis [5, 6].
Markers such as CD3, CD20, CD30, CD10, BCL6, Ki-67 and MUM1 help identify the cell types and their proliferation patterns, which are important for distinguishing between benign and malignant processes [7]. Advanced imaging, especially PET-CT helps identify metabolically active lymph nodes, splenic enlargement or other organ involvement, and guides the selection of biopsy sites [8]. Once a diagnosis of AITL is confirmed, treatment typically involves multi-agent chemotherapy such as CHOP or CHOEP regimens. However, the prognosis remains guarded due to its aggressive nature and frequent relapses.
Case Report
A 79-year-old male presented with a 2-week history of red, raised, itchy lesions on his upper back and chest [Fig. 1]. The lesions started as small pea-sized spots and gradually increased to coin-sized raised lesions. This was his first complaint and presentation, leading to the initial clinical workup. He also reported swelling on both sides of his neck for one month.
His medical history included ulcerative colitis (diagnosed in 2024) and hypertension (managed for four years). His vitals were stable, and there was no significant family history of similar conditions.
Fig. 1: Multiple, well defined erythematous papules and plaques seen over upper back and chest
Cutaneous examination showed multiple well-defined erythematous papules and plaques on the chest and upper back, along with a solitary erythematous nodule on the upper back. The clinical differential diagnoses included lymphomatoid papulosis, sarcoidosis, lymphocytoma cutis, and mycosis fungoides.
Routine urine, liver, and kidney function tests were normal. Blood tests revealed mild normocytic normochromic anemia. Serum cystatin C was within the normal range (0.79 mg/L). Abdominal and pelvis ultrasound detected a left non-obstructive renal calculus. CRP was elevated (17.4 mg/L), indicating inflammation.
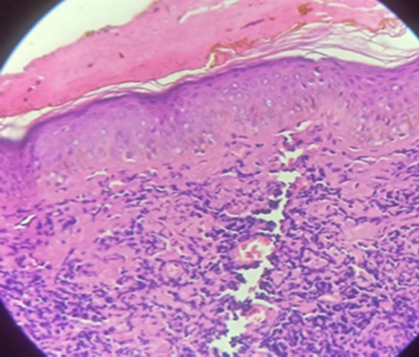
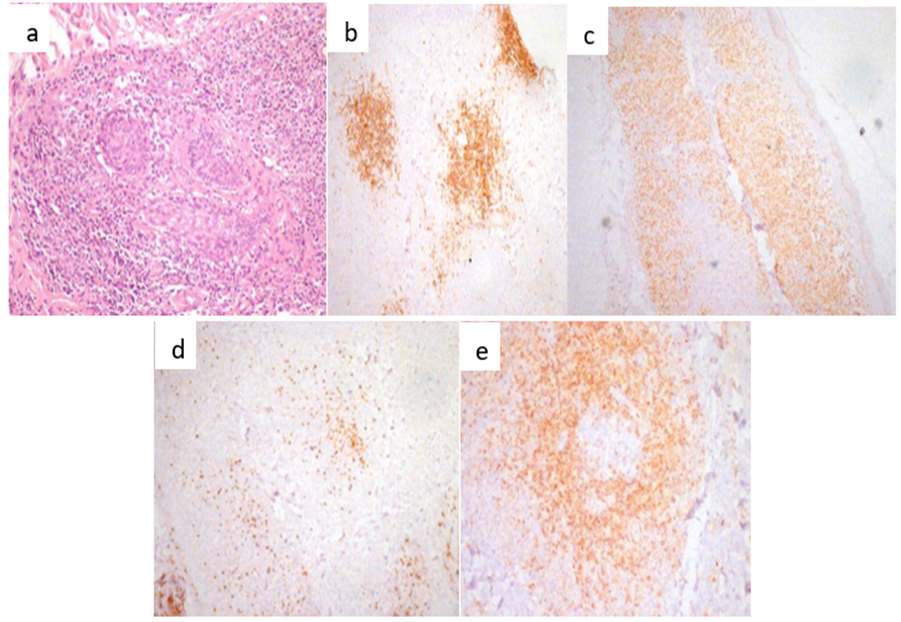
A skin biopsy showed spongiosis and dense interstitial lymphohistiocytic infiltration with occasional plasma cell infiltration [Fig. 2]. Immunohistochemistry revealed a mixed T-cell and B-cell infiltrate, positive for CD20, CD30, CD56, MUM1, Ki-67, BCL6 and BCL2 but negative for CD10 [Fig. 3].
A right cervical lymph node biopsy prompted by his second complaint of neck swelling confirmed angioimmunoblastic T-cell lymphoma (AITL) with CD3, BCL2, and CD30 positivity and a Ki-67 proliferation index of 56-58%.The PET-CT scan showed mild FDG uptake in a mildly bulky left palatine tonsil. Multiple FDG-avid lymph nodes were present on both sides of the diaphragm, and there was diffuse increased FDG uptake in the spleen, suggesting systemic involvement. The 2D ECHO findings revealed no regional wall motion abnormalities, with a left ventricular ejection fraction (LVEF) of 56%, indicating normal left ventricular systolic function. There was no evidence suggestive of pulmonary arterial hypertension (PAH).
Fig. 2: H &E 10x section of skin biopsy showing spongiosis, dense interstitial lymphohistiocytic with occasional plasma cells infiltration
Fig. 3: Immunohistochemistry revealed: a) Periadnexal lymphoid infiltrate of an admixture of T and B cells; b) CD20 expressed in follicles; c) MUM1 expressed in plasma cells; d) Ki-67 expressed in the retained and distorted germinal centres; e) BCL2 expressed in T cells
Based on clinical examination, histopathology, and immunohistochemistry findings, the diagnosis was established as Spiegler-Fendt sarcoid (lymphocytoma cutis). The patient was treated with oral methotrexate 7.5 mg weekly along with oral folic acid for 2 months. Topical high-potency corticosteroids and topical antibiotics were prescribed for 1 month, along with narrow-band UVB phototherapy administered three times per week. The patient responded well to this treatment regimen.
Fig. 4: Pre- & Post- treatment pictures of upper back
Subsequently, based on clinical examination, right cervical lymph node biopsy, and PET-CT findings following his second presentation, the diagnosis was established as Angioimmunoblastic T-cell lymphoma (AITL), Stage 3. The patient was initiated on IV chemotherapy. Cycle 1 of chemotherapy with the CVP regimen was administered, followed by post-chemotherapy IV hydration. Cycle 2 of chemotherapy with the CHOP regimen was administered as per protocol. The patient tolerated the treatment well and was discharged in a stable condition with appropriate advice.
Discussion
The patient's initial presentation as Spiegler-Fendt sarcoid was particularly unusual given this condition's well-documented female predominance (3:1 female-to-male ratio in most series) and typical occurrence in younger patients (median age 45 years), that progressed to systemic AITL. This unusual presentation shares similarities with Oliveira et al.'s report of cutaneous lymphoid hyperplasia in its initial manifestation of erythematous plaques with mixed infiltrates, yet critically diverges in its malignant transformation, highlighting both the diagnostic complexity and the importance of molecular studies and systemic staging in persistent cutaneous lymphoid proliferations [9]. Bergman et al.'s case emphasizes the role of follicular helper T-cell markers (CD10, BCL6, PD-1) and CD30 expression in distinguishing benign from malignant processes [10].
The case by Gupta et al. on AITL showed rapid progression despite similar TFH phenotype, illustrating the broad spectrum of disease behavior and strongly suggests that early systemic therapy may significantly improve outcomes in non-regressing cases [11]. While typical AITL presentation involves systemic symptoms (70-80% of cases), generalized lymphadenopathy (90%), and constitutional symptoms features absent in our patient's initial presentation but emerging during progression, our case demonstrated better response to CHOP chemotherapy potentially reflecting the therapeutic advantage of early detection through cutaneous manifestations before immune dysregulation developed.
These collective observations highlight the necessity of considering AITL in persistent cutaneous lymphoid infiltrates even when initial features suggest benignity.
Conclusion
This case of Spiegler-Fendt sarcoid in an elderly male with concurrent AITL expands the known demographic spectrum of this condition. The diagnostic challenge of distinguishing benign pseudolymphoma from malignant lymphoma highlights the importance of comprehensive histopathological and immunohistochemical evaluation. The patient's excellent response to combined dermatologic and oncologic therapies highlights the value of multidisciplinary management in such complex cases. This report emphasizes the need for malignancy surveillance in atypical presentations of cutaneous pseudolymphoma.
References
Charli-Joseph YV, Gatica-Torres M, Pincus LB
Approach to Cutaneous Lymphoid Infiltrates: When to Consider Lymphoma?Indian Journal of Dermatology2016614https://doi.org/10.4103/0019-5154.185698
van Vloten WA, Willemze R
The many faces of lymphocytoma cutisJournal of the European Academy of Dermatology and Venereology2003171https://doi.org/10.1046/j.1468-3083.2003.00482.x
Sehgal VN, Sehgal D, Lal JB, Sharma S
Spiegler–Fendt sarcoid/lymphocytoma cutis: A focus on nomenclature and diagnosisIndian Journal of Paediatric Dermatology2018192https://doi.org/10.4103/ijpd.ijpd_36_17
Rüdiger T, Weisenburger DD, Anderson JR, Armitage JO, Diebold J, MacLennan KA, <I>et al</I>
Non-Hodgkin's Lymphoma Classification Project. Peripheral T-cell lymphoma (excluding anaplastic large-cell lymphoma): results from the Non-Hodgkin's Lymphoma Classification ProjectAnnals of Oncology2002131https://doi.org/10.1093/annonc/mdf033
Xie Y, Jaffe ES
How I Diagnose Angioimmunoblastic T-Cell LymphomaAmerican Journal of Clinical Pathology20211561https://doi.org/10.1093/ajcp/aqab090
Iannitto E, Ferreri AJ, Minardi V, Tripodo C, Kreipe HH
Angioimmunoblastic T-cell lymphomaCritical Reviews in Oncology/Hematology2008683https://doi.org/10.1016/j.critrevonc.2008.06.012
Boyd SD, Natkunam Y, Allen JR, Warnke RA
Selective Immunophenotyping for Diagnosis of B-cell NeoplasmsApplied Immunohistochemistry & Molecular Morphology2013212https://doi.org/10.1097/pai.0b013e31825d550a
Kostakoglu L
PET-CT Imaging of LymphomaClinical PET-CT in Radiology2011https://doi.org/10.1007/978-0-387-48902-5_22
Oliveira EV, Badiale GB, Moraes MM
Lymphocytoma cutis - case reportAnais Brasileiros de Dermatologia2013886 suppl 1https://doi.org/10.1590/abd1806-4841.20132320
Bergman R, Khamaysi Z, Sahar D, Ben-Arieh Y
Cutaneous Lymphoid Hyperplasia Presenting as a Solitary Facial NoduleArchives of Dermatology200614212https://doi.org/10.1001/archderm.142.12.1561
Gupta D, Jaine NS, Bairwa SK, Thirunavukkarasu B, Vishwajeet V, Purohit AHL
Case of angioimmunoblastic T-cell lymphoma presenting as peripheral and bone marrow plasmacytosis: A diagnostic conundrumIndian Journal of Pathology and Microbiology2024672https://doi.org/10.4103/ijpm.ijpm_277_22