Introduction
Stress in medical students has become a focus of concern across the globe.[1,2] Besides day-to- day stress, medical students have to endure stress related to medical education.[3] Stress is body’s reaction to demands or challenges made on it or to disturbing events in the environment.[4] Stress may be perceived as positive eustress or as negative distress. Distress occurs when a demand exceeds individual’s capability to cope.[5] When mental pressure becomes severe, it starts affecting the mood, behavior, sleeping, and eating habits of the person hence not just affecting the physical health but mental incapacitance as well.[6,7]
Conditions such as anxiety, depression, and emotional disorders have been documented vastly among medical students by many researchers worldwide[8] and have been allied to use of addictive drugs.[9] Increased evidence of dropout[10] and suicidal attempts[11] are observed among medical students. Chronic exposure to stressful conditions leads to memory loss, deterioration of academic performance, poor relationship with peers and family members, and overall dissatisfaction with life.[12]
Studies reveal that medical students mental health is similar to their non-medical peers at the start of the course[7] and worsens with advancement of the course.[1,8,13] The 1st year of the course marks the stage of transition for medical students and is observed to be highly stressful phase in most of the studies.[1,13] However, some researchers have reported higher stress as the course advances mostly in the final year students.[2]
With early stress assessment and effective training, future psychological ailments in medical students can be avoided.[14] Due to lacunae of literature in respect to such studies in an Indian urban medical college setup, the present study objectives are to estimate the stress prevalence in different study groups considering the differences of gender and residence at home or hostel and its effect on the mental health and academic accomplishment among the 1st year medical students.
Materials and Methods
After getting Institutional Ethics Committee permission, this cross-sectional study was conducted during the period of 1 year from September 2017 to August 2018 on the 1st year medical college students in India. The first MBBS students consenting to participate in study were included in the study. Students having psychiatric history or reporting any previous drug abuse, and use of antipsychotic drugs were excluded from the present study. Fifty male and 49 female students of the total batch of 99 students got enrolled in the study willingly.
To evaluate stress prevalence and its effect on mental health, validated General Health Questionnaire (GHQ-12) was used. It is an extensively used tool, consisting of six positive and six negative items to screen emotional disorders and evaluate stress levels. Four graded responses used for six positive items were more, same, less, and much less than usual and for six negative items, responses were not at all, no more, more, and much more than usual.
The study was conducted during mid-course, 1 month before terminal examination to avoid examination stress. Students assembled in lecture hall, were explained about the study objectives with assurance of confidentiality. Students were instructed to choose from given four responses to rate each item based on their experiences in the past few weeks.
Modified binary method was used for scoring GHQ- 12. Score 0 was given to the least responsive answers and score 1 was given to the most responsive answers. Thus based on the four responses, for positive items score of 0,0,1,1 and for negative items score of 0,1,1,1 was considered.[15] The CGHQ-12 scoring had minimum score of 0 and the maximum score of 12. GHQ-12 score with cutoff point at 4 had high sensitivity and specificity.[16] Therefore, participants with GHQ-12 score of 4 and more were considered to have significant stress in this study. Grading of stress was done: Mild stress with score between 4 and 6, moderate stress with score between 7 and 9, and severe stress with score between 10 and 12.
Internal assessment examination marks held around 1 month later which was used to study the impact of stress on students’ academic performance after taking consent.
Statistical analysis
With the help of GHQ-12 score, distribution of stress levels in different study groups was calculated. Data analysis was done using SPSS software version 19 by applying Chi-square test and Pearson’s correlation to obtain statistical significance of difference.
Results
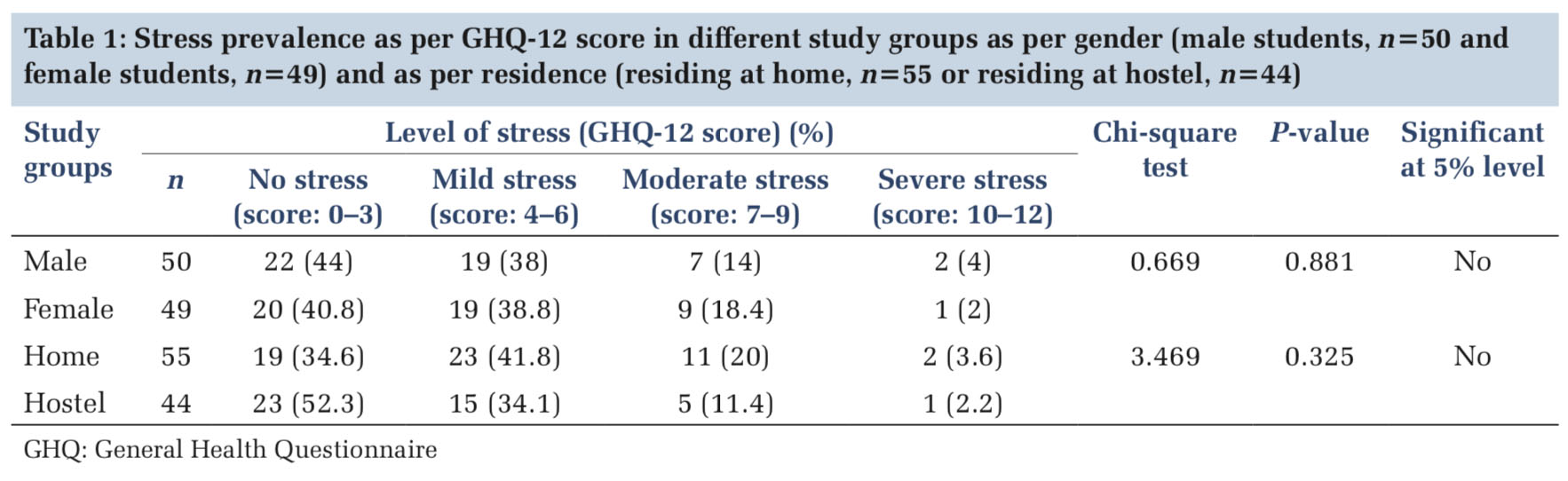
Table 1 depicts higher stress prevalence among the 1st year medical students. Out of total 99 students, 57 students mean GHQ-12 score was 4 and above signifying higher prevalence of psychological distress and its negative effect on mental health of the students.
Considering gender differences, the mean GHQ-12 score was observed to be high in male students (6.12 ± 1.41) compared to female students (4.29 ± 2.12). However, on comparing stress prevalence, there was no statistically significant difference in stress prevalence between male (58%) and female (57.1%) students.
Considering differences on the basis of residence at home or hostel, mean GHQ-12 score was observed to be higher for home group students (4.76 ± 0.71) compared to hostel group (3.66 ± 2.12) of students. However, stress prevalence was higher in the home group students (65.5%) compared to hostel group (47.7%) students but not statistically significant.
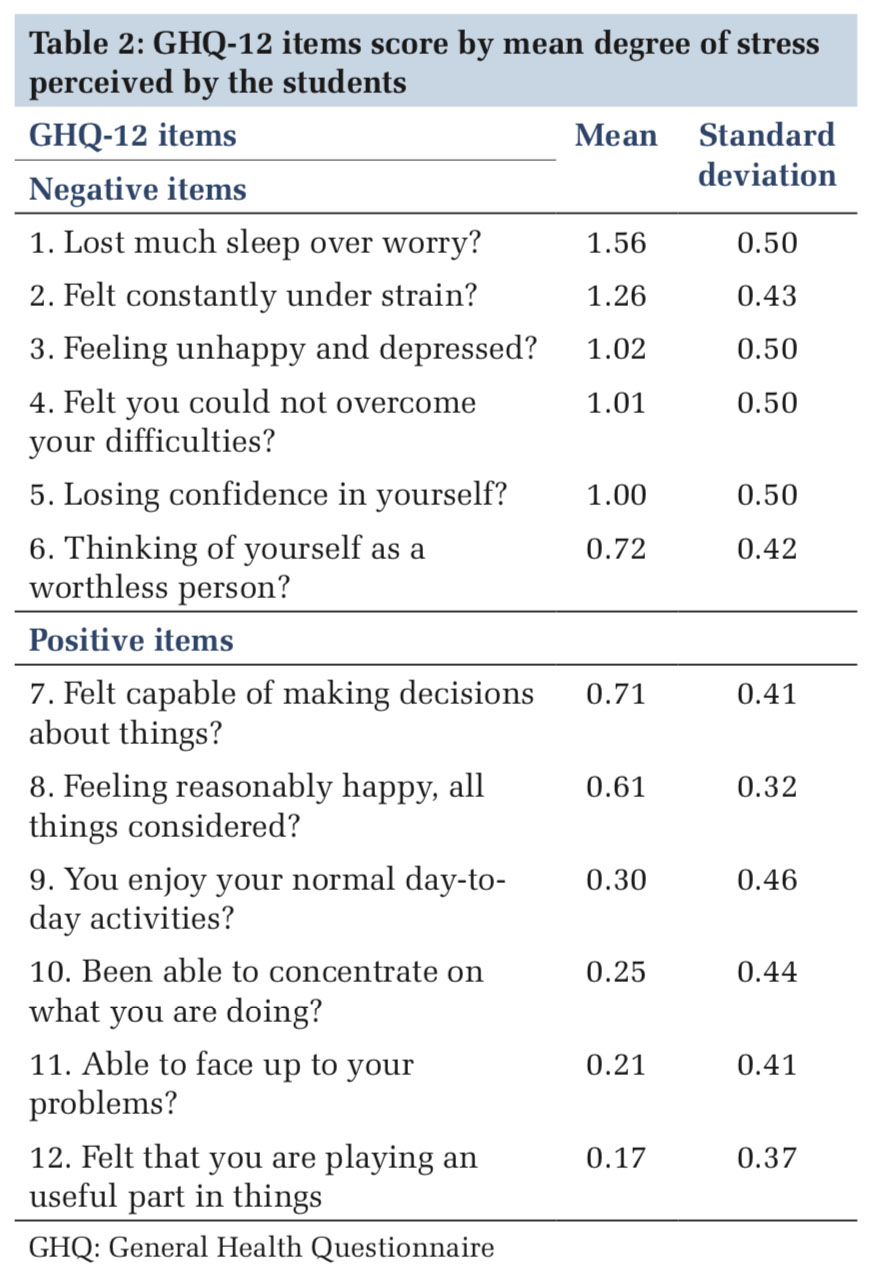
Among all the 12 items assessed by GHQ-12, as shown in Table 2, higher mean score was observed for mainly two negative items – sleep loss over worry and feeling of constant strain indicating high prevalence of psychological distress among the 1st year medical students.
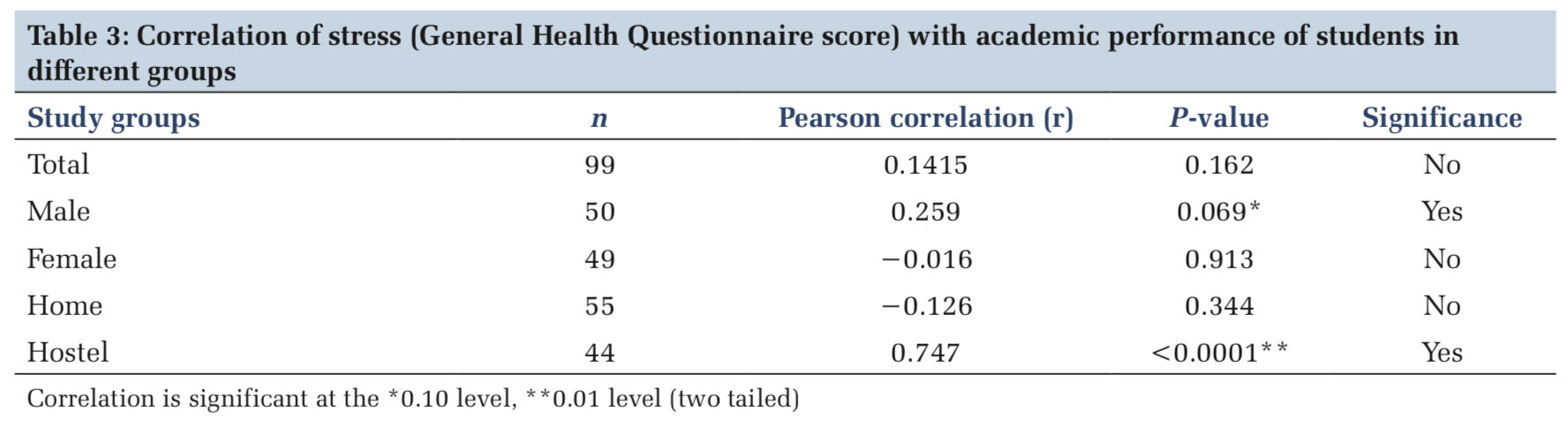
As shown in Table3, mild degree of positive correlation of stress with academic performance was observed for total group but not significant statistically.
There was also positive correlation observed for male group significant statistically at 0.10 level and for hostel group with high statistical significance at 0.01 level. For both female and home residence group of students, negative correlation was observed though not significant statistically.
Discussion
The present study shows that 57 students out of 99 had mean GHQ-12 score above cutoff point 4 indicating significant psychological distress. This finding is consistent with studies in other countries which show the 1st year students as highly susceptible for stress[1,2,13] compared to subsequent years students with minimized level of stress.[17] It is observed that with advancement of the course, students develop copying skills to manage stress better compared to students in the early phase of training.[18]
Most of the studies show academic factors among all the stressors to mainly contribute to stress in medical students.[1,2,13] As academic examinations are found to be the major stressors, emphasis on reduction of academic stress factors and having assessment friendly to psychological health of the students is necessary.[19]
Considering gender differences, there was no significant difference of stress prevalence. Significant difference between male and female students has been observed by other researchers.[2,13] However, no difference between male and female students is also documented by others.[20,21]
In the present study, stress levels were more in students residing at home than students residing at hostel. Higher susceptibility to develop psychological stress and anxiety by medical students living with families was also reported by other study.[22] However, this finding is in contrary to other study which reported higher amount of depression and anxiety in medical students living in dormitory compared to students living with families.[23]
One of the studies reveals that students staying at hostel learn to live independently without any parental guidance and support. Hostel life tends to make students more punctual, social, realistic, and disciplined. Students learn to solve their own problems, thus making them sharper and more confident.[24]
Among all the 12 items assessed by GHQ-12, higher mean score was for two negative items – loss of sleep over worry and feeling of constant strain indicating high prevalence of psychological distress symptoms among the 1st year medical students. The study in Malaysia has also reported similar finding of sleep loss linked to stress.[25]
There was mild degree of positive correlation observed between stress and academic performance of the students but not statistically significant. Another study with similar finding states that moderate stress is desirable for attaining good academic performance by the students.[26] However, other studies report negative correlation between stress and academic achievement.[27,28]
Mean GHQ-12 score and academic performance were higher in male group and home group compared to female and hostel group of students, respectively. Positive correlation was observed for male group (P < 0.10) and for hostel group of students with high statistical significance (P < 0.01). Negative correlation was observed for female and hostel group of students though not statistically significant. One of the researchers states that stress is essential for the process of learning.[29] Another study claims that students with high resources are able to manage stress due to academic factors better.[30] Thus, some amount of stress is necessary and helps to develop healthy competition essence among students. However, undue severe stress is likely to have an undesirable health effect on the students.[31]
High prevalence of psychological distress in students in spite of regular academic counseling and mentoring sessions done by teachers in the current setup put emphasis on screening of students for negative events in early phase of medical school life. Implementation of new competency-based curriculum and inclusion of foundation course, stress and time management, and communication skills training for future undergraduate medical students are need for the hour.[32]
|