Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i1.22.112
Year: 2023, Volume: 9, Issue: 1, Pages: 23-28
Original Article
J Sagathia Kinjal1 , I Mulla Faruq2 , Monica Gupta3
1Resident,, P.S. Medical College, Bhaikaka University, Gujarat, India,
2Professor, Department of Pathology, P.S. Medical College, Bhaikaka University, Gujarat, India, 3Professor & Head of the Department in Pathology, PSMC, Karamsad, Anand, Gujarat, India
Address for correspondence:
I Mulla Faruq, Professor, Department of Pathology, P.S. Medical College, Bhaikaka University, Gujarat, India.
E-mail: [email protected]
Received Date:03 March 2022, Accepted Date:19 December 2022, Published Date:13 January 2023
Context: Tru cut biopsy is a minimally invasive procedure because of its low morbidity and low cost and are preferred standards of care to initially access cells from tumours and other lesions for diagnostic assessment. Aims: To evaluate the usefulness of Tru cut biopsy for various tissue diagnosis and to analyse its sensitivity, specificity, positive and negative predictive values and the accuracy. Settings and Design: The present study is a prospective and retrospective observational study for patients undergoing Tru cut or excisional biopsy. Methods and Material: The present study was undertaken at the Department of Histopathology, Central Diagnostic Laboratory, Pramukhswami medical college and Shree Krishna Hospital, Karamsad, Anand for a period from April 2014 to March 2021 that included 497 samples of Tru cut biopsy. Data was retrieved from the Laboratory Information System of the hospital according to the proforma. Statistical analysis: Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Accuracy were found. Results: Of the 497 Tru cut biopsy samples, 105 excision biopsy were received. For the remaining 392 samples, descriptive analysis was done. Mean age of participants in excision biopsy group was 55.2±14.4 years with female participants (n=92, 87.6%) outnumbering males (n=13, 12.4%) and breast being the most common site of biopsy. There were 6 discordant and 99 concordant cases. Sensitivity, Specificity, Positive predictive value, Negative Predictive value and Accuracy were 96.73%, 92.30%, 98.8%, 80% and 96.1% respectively. Conclusions: Thus, for solitary or diffuse tissue lesions, needle biopsies provide precise localization and are much more likely to yield representative samples cost-effectively with a good safety profile.
Keywords: Tru cut biopsy, Excision biopsy, Concordance, Discordance, Sensitivity
Cancer is one of the leading causes of death after cardiovascular diseases 1. Cancer burden continues to grow globally, exerting tremendous physical, emotional and financial strain on individuals and healthcare system. Quality medical care begins with accurate diagnosis - a combination of good clinical eye, high-quality imaging, and appropriate pathological techniques.
The emergence of the Tru-Cut biopsy (TCB) in the recent years has helped in histological assessments ensuring information essential to guide a suitable therapeutic strategy for patients, being first preferred procedure for the diagnosis of breast lesions prior to operation 2 and has also gained popularity for intra thoracic and intra-abdominal masses 3, 4 . The present study intends to review the diagnostic usefulness of Tru cut biopsy, as it causes minimal morbidity, is less time-consuming, cost effective and provides a tissue diagnosis of malignancy before definitive treatment and obviates the need for formal excision biopsy of lesions for which there is low index of suspicion.
To evaluate the usefulness of Tru cut biopsy for various tissue diagnosis and to analyse its sensitivity, specificity, positive and negative predictive values and the accuracy.
It was a retrospective and prospective observational study carried out at the Department of Histopathology, Central Diagnostic Laboratory, Pramukhswami medical college and Shree Krishna Hospital, Karamsad, Anand for a period from April 2014 to March 2021. A total of 497 samples were studied.
Inclusion Criteria
All the Tru cut biopsy and excision biopsy data in the above mentioned time period were included.
For statistical analysis, only the tru cut biopsies with their excisional counterpart were included.
Exclusion Criteria
Ethical approval was granted by the Institutional Ethics Committee, H M Patel Centre for Medical Care and Education, Karamsad, Anand in the 118th IEC Meeting (Ref no : 76/2020) with waiver of consent. Strict confidentiality had been maintained regarding patients’ personal details. The data was collected from the Laboratory Information System.
The data from histopathology records was analyzed for Sensitivity, Specificity, Positive Predictive value, Negative Predictive value and Accuracy. For confirmatory diagnosis of Tru cut biopsies, the diagnosis obtained in their excisional counterpart were considered gold standard. Descriptive analysis was done for the biopsy data where excisional biopsy was not received.

The present study analyzed total 497 samples of Tru cut biopsies which were divided into two groups. The first group comprised of the patients in whom Tru cut and excision biopsy, both were performed (N=105). The second study group comprised of the patients in whom only Tru cut biopsy was performed but the excision biopsy was not received (N=392). The histopathological diagnosis of both the biopsies (Tru cut and excision biopsy) were compared and were designated as either benign or malignant. Based on this comparison, Sensitivity, Specificity, PPV, NPV, Accuracy, Positive and Negative Likelihood Ratios of the Tru cut biopsy were derived.
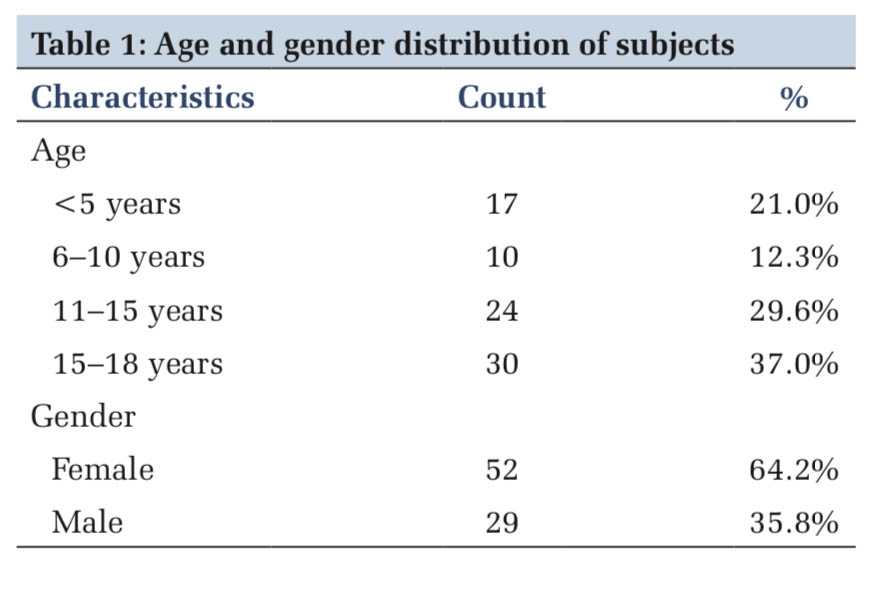
Mean age of study participants in excision biopsy group was 55.2 years with standard deviation of 14.4 years. Female participants were 87.6% (N=92) and male participants were 12.4% (N=13).
The most common site of biopsy was breast (n=90, 85.7%) followed by Axilla, Liver and Thigh (n=2, 1.9% each) and the rest constituted by Shoulder, Ovary, Prostate, Chest wall, Arm, Skin, Foot & Thyroid (n=1, 0.8% each).
Of the total 105 samples studied, six depicted discordances between Tru cut and excision biopsy findings. Out of the six discordant ones, five were malignant which were diagnosed as benign while one turned out to be benign on excision biopsy but the excision was done post chemotherapy and radiotherapy.
Concordance rate : (99/105) × 100 = 94.28%
Discordance rate : (6/105) × 100 = 5.71%
|
Tru cut biopsy |
Excision biopsy |
Total |
|
|
Malignant |
89 |
01 |
90 |
|
Benign |
03 |
12 |
15 |
|
Total |
92 |
13 |
105 |
(*True positive = 89, True negative = 12, False positive = 01, False negative = 03)
Sensitivity, Specificity, Positive predictive value, Negative Predictive value and Accuracy were 96.73%, 92.30%, 98.8%, 80% and 96.1% respectively. However, as NPV and PPV depend on prevalence of a disease in the population, positive and negative likelihood ratios were derived to eliminate the population parameter.
Likelihood Ratio + : 0.967/ (1-0.923) = 13.81
Likelihood Ratio - : (1-0.967)/0.923 = 0.03
|
Tru cut biopsy |
Excision biopsy |
Total |
|
|
Malignant |
80 |
01 |
81 |
|
Benign |
03 |
06 |
09 |
|
Total |
83 |
07 |
90 |
As majority of the Tru cut biopsies were from breast (90/105), and their excision biopsy had also been received, Sensitivity, Specificity, PPV and NPV were calculated separately for breast specimens. (Tru cut biopsy from breast and their counterpart Modified radical mastectomy and lumpectomy). Sensitivity, Specificity, Positive predictive value, Negative Predictive value and Accuracy for breast biopsies were 96.3%, 85.71%, 98.7%, 66.6% and 95.5% respectively.
Likelihood Ratio + : 0.963/ (1-0.857) = 6.73
Likelihood Ratio - : (1-0.963)/0.857 = 0.04
The Fine Needle Aspiration Biopsy from breast was done in 22 participants out of the 497 participants studied which diagnosed 14 lesions to be malignant, four lesion as atypia - probably benign, one as benign lesion and three as suspicious of malignancy. The smears were inadequate in one case.
A descriptive analysis was performed for the participants whose tru cut biopsy was only received, but excision biopsy wasn’t. The data was analyzed based on the demographic details, biopsy site distribution and histopathological diagnosis. There were 200 males (51%) and 192 female (49%) participants in ‘Only Tru cut biopsy group’.
Formerly, histologic evaluation was limited to samples obtained by surgical excision. Today there are additional options of ultrasound-guided fine needle aspiration, Tru cut biopsies, or visually-guided samples obtained via laparoscopy or endoscopy. Cytology is appropriate when there is a suspicion of a disease in which the tissue architecture is not important, and in which the lesion is more-or-less diffuse within the tissue and the critical diagnostic information is likely to be gained from examination of individual cell morphology or the detection of infectious agents, without regard for tissue architecture. Tissue core biopsies retrieve only tiny histologic samples and are appropriate when the anticipated histologic changes are widespread within the tissue with need for at least some appreciation of architectural arrangement of the diseased tissue.
Presently, the most frequent minimally invasive biopsy technique is fine-needle aspiration biopsy (FNAB). In current study, the FNABs done from breast diagnosed 14 lesions to be malignant, four lesions as atypia probably benign, one as benign lesion and three as suspicious of malignancy. The smears were inadequate in one case. These findings are comparable to the study done by Saha et al5 in which there were 29 malignant, 14 benign, two as atypia probably benign and five were diagnosed as suspicious of malignancy on FNAB.
The main limitations FNAB, however, are the small sample size which may not allow immunohistochemistry staining, which could play a crucial role in the differential diagnosis 6, and often no appreciation of tissue architecture, resulting in a high rate of inadequate samples for histological assessment. As cytological smears cannot reliably predict invasion, benign and borderline lesions cannot always be reliably distinguished from their malignant counterparts 7 . Because needle biopsies are minimally invasive, they are widely used, despite known limitations of clinical inadequacy ranging from 9% to 34% for breast and thyroid lesions 8, 9, 10 to the 50% range for molecular assessment of endobronchial and deep abdominal lesions 11
Patients who underwent the procedure either had a clinically palpable mass or their radiology report seemed to be suspicious in the present study of 497 samples. Majority of specimens in the excision biopsy group comprised of breast (N=90). There were 9 (10%) benign and 81 (90%) malignant cases identified by Tru cut biopsy. Excision biopsy diagnosed 7 (7.7%) benign and 83 (92.2%) malignant cases. Various histological findings obtained were Atypical ductal hyperplasia (N=4), Fibroadenoma (N=2), Phyllodes tumour (N=1), Fibrocystic disease (N=1) and Infiltrating duct carcinoma, not otherwise specified type (N=82). There were three false negative cases and one false positive case, which is explicable for the fact that the mastectomy specimen was received after the patient had undergone chemotherapy and radiotherapy, hence no residual tumour was found.
Our institution being a chief tertiary care hospital in the Charotar region with a dedicated centre for oncology, has high inflow of patients with suspicious malignancy and high level of referral rate from the periphery region as well, thus explaining high rate of malignancy.
Discordant cases [Atypical ductal hyperplasia(ADH) which turned out to be invasive carcinoma on excision] can be elucidated by certain limitations of Tru cut biopsy as the merits of technique do not overcome the risk of underestimation of malignancy. In hyperplasia (with or without atypia) and papillary lesions, it is crucial to do open biopsy to exclude carcinoma. Present study showed three cases of atypical ductal hyperplasia in Tru cut biopsy which had invasive carcinoma after excision biopsy explained by the inherent ambiguity of ADH. Histologically, ADH has some cytological similarity to Ductal carcinoma in situ (DCIS) but, is usually present in a single duct and with size <2 mm 16. When the lesion is heterogeneous, that is, combined with ADH, DCIS, or even invasive cancer, sampling of biopsy can determine which feature is seen. Underestimation of malignancy can occur if ADH instead of DCIS or invasive cancer is retrieved from the specimen17, 18 making the role of radiologist or surgeon taking the biopsy very significant.
Needle gauges also influence the amount and volume of tissue retrieved which can be the probable reason for diagnostic inconclusiveness or non-representativeness. An eight-gauge vacuum-assisted needle results in a 39% increase in tissue harvesting compared to an 11-gauge needle biopsy 19.
Of 105 samples, there were two Tru cut biopsy from lymph nodes. One of them provided an inconclusive diagnosis which on excision, was diagnosed as Non Hodgkin’s lymphoma. This is comparable to a study conducted by Kilicarslan et al 20. As the sensitivity of CNB is lower than its specificity, it is recommended that the surgical excision of lymph nodes with a clinically strong suspicion of neoplasm be done, because of the presence of false negative cases. Hence, it can be said that Tru cut biopsies are better for diagnosing metastasis to lymph node but for disease like Lymphoma, where whole node architecture needs to be studied, excision biopsy are inadvertently required.
There are some limitations to Tru-Cut biopsy that may result in a diagnostic inaccuracy. In order to accomplish them, multidisciplinary teamwork is essential with strict cooperation among radiologist, surgeon and pathologist. It is highly recommended that all Tru-Cut biopsies be given to radiologists, which may be useful for both the patient and the success ratio. The skills of operating surgeon also play an important role in the final judgement (monitoring or surgery alone) for diagnostic and treatment planning and subsequent steps because of the error in sampling the tissue and can be reduced by taking multiple cores of tissue from the lesion. Image-guided biopsies, Automated biopsy needle and Vacuum Assisted Biopsy are the newer techniques. However, role of Tru cut biopsy becomes miniscule where diagnosis necessarily requires mitotic count, percentage of necrosis and lymphovascular invasion.
Limitation of the present study was that the number of excision biopsy obtained for the respective tru cut biopsy were less as patients were lost in follow up. Data (prospective as well as retrospective) for biopsies done under radiological guidance could not be retrieved.
Nil.
None
We acknowledge the relentless support provided by the Head of the Department, technical staff of histopathology, beloved colleagues Dr Khevna, Dr Yogesh , Dr. Jigisha, Dr. Esha, Dr. Vashistha, Dr. Vandana and the Hospital Information Systems.
Subscribe now for latest articles and news.