Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i2.24.235
Year: 2025, Volume: 11, Issue: 2, Pages: 154-159
Original Article
Vivek Shende1 , Nishat Khan2 , Sandhya Sawant3 , Nirjhar Chatterjee4 , Reena Set5
1 Junior Resident, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India,
2Additional Professor, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India,
3Additional Associate Professor, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India,
4Assistant Professor, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India,
5Professor & Head, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India
Address for correspondence:
Vivek Shende, Junior Resident, Department of Microbiology, Topiwala National Medical College & BYL Nair Ch. Hospital, Mumbai, Maharashtra, India.
E-mail: [email protected]
Received Date:24 July 2024, Accepted Date:22 February 2025, Published Date:16 June 2025
ntroduction: Enteric fever is a systemic disease caused by Salmonella enterica serotype Typhi and is a major cause of morbidity and mortality worldwide. Infection occurs in all age groups, and it is transmitted by ingestion of food or water contaminated with feces. Thus, this study is undertaken to determine the prevalence of widal positivity and its seasonal trend from 2015 to 2022 in a tertiary care hospital. Material & Methods: The present study is a retrospective study which was conducted in Department of Microbiology of a tertiary care hospital in Mumbai from January 2015 to December 2022. A total of 11,135 samples were analyzed during the study. Analysis was done and data was presented as numbers and percentages. Results: A total of 11,135 blood samples were analyzed during the study period, out of which 1245 samples were positive for widal test. Out of 1245 positive samples, adult and paediatric cases were 895 and 350 respectively. The overall prevalence was found to be 11.18 %; the male to female prevalence ratio was 1:1.22. Increased widal positivity was seen from June to September corresponding to the monsoon season. Conclusion: Enteric fever remains an important public health problem in developing countries. Though blood culture method has been used as gold standard method for diagnosis of enteric fever, it has certain limitations. Therefore, widal test, which is more rapid, simpler, and cheaper diagnostic method is very useful.
Keywords: Widal test, Enteric fever, Prevalence, Seasonal variation
Enteric fever, encompassing both typhoid and paratyphoid fever, is a significant systemic febrile illness caused by the bacteria Salmonella enterica serovar typhi and Salmonella enterica serovar paratyphi A, B, and C. 1
The disease burden in terms of enteric fever mortality and morbidity has been notably reduced in industrialized countries due to improvements in living conditions and the use of antibiotics. However, enteric fever remains a major public health issue in many developing nations within the WHO African, Eastern Mediterranean, South-East Asia, and Western Pacific Regions. According to 2019 data, there are approximately 9 million cases of enteric fever annually, leading to around 1,10,000 deaths each year. 2
Humans are the sole reservoir and host for enteric fever, which is transmitted through the consumption of contaminated water and food. 3
The median infective dose (ID50) for Salmonella infection ranges from 103 to 106 bacilli, with an incubation period typically around 14 days. Common clinical features of the disease include fever, bradycardia, and toxaemia. 4
A definitive diagnosis of typhoid fever involves isolating Salmonella from blood, faeces, urine, or other body fluids. 5 Prior to the initiation of the antibiotic therapy, culture isolation of Salmonella typhi can confirm diagnosis in 73% to 97% of cases, but excessive antibiotic use has reduced this rate to 40% to 60%. The culture isolation process is time-consuming and often infeasible in resource-limited regions. 1
Consequently, in such regions, diagnosis frequently relies upon looking for the clinical features and the detection of agglutinating antibodies to Salmonella typhi by using the widal test. 5
Developed by Georges Fernand Widal in 1896, the widal test is a sero-diagnostic test, that has been widely used for over a century. 6 This test detects antibodies to Salmonella typhi and Salmonella paratyphi in the patient's serum from the second week of symptoms onset. Despite its limitations, the widal test remains a valuable, accessible, cost-effective, and simple diagnostic tool for enteric fever diagnosis in resource-limited settings. 7
So, the present study was done to determine the prevalence of widal positivity and to correlate this positivity with the seasonal trends in a tertiary care hospital.
The present study was conducted in the Serology section of Microbiology department, Topiwala National Medical College and B.Y.L Nair Charitable hospital, Mumbai, Maharashtra. It is a retrospective study, and the study period was from January 2015 to December 2022.
A total of 11,135 samples were received in serology laboratory from patients presenting with acute febrile illness from outpatient, inpatient and emergency medical services of Nair hospital.
The inclusion criteria was all the samples received in the laboratory for widal testing; and the exclusion criteria was hemolysed and lipemic blood samples which were not included in the study.
The widal tube agglutination test was performed on serum samples as per manufacturer’s instruction (Typhocheck kit by Tulip Diagnostics Pvt Ltd). Positive and negative controls were also included in each batch of the test. Interpretations of the results were done as per the kit literature.
Diagnostic titres of 1:80 and above were taken as positive.
As our study is a retrospective analysis, results of the widal tests were not compared with the blood culture.
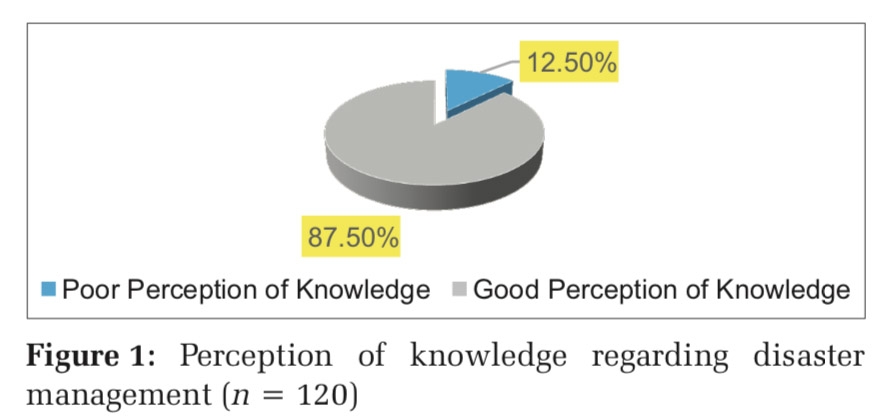
A total of 11,135 blood samples were analyzed during the study period, out of which 1245 samples had significant titer of > 1:80 for O, H, AH and BH antibodies. So, the overall prevalence was found to be 11.18 % (Figure 1).

Out of the 1245 positive samples, 292(23%) were positive for O antibodies, 795(64%) were positive for H antibodies, 109(9%) were positive for AH antibodies and 49(4%) were positive for BH antibodies (Figure 2).

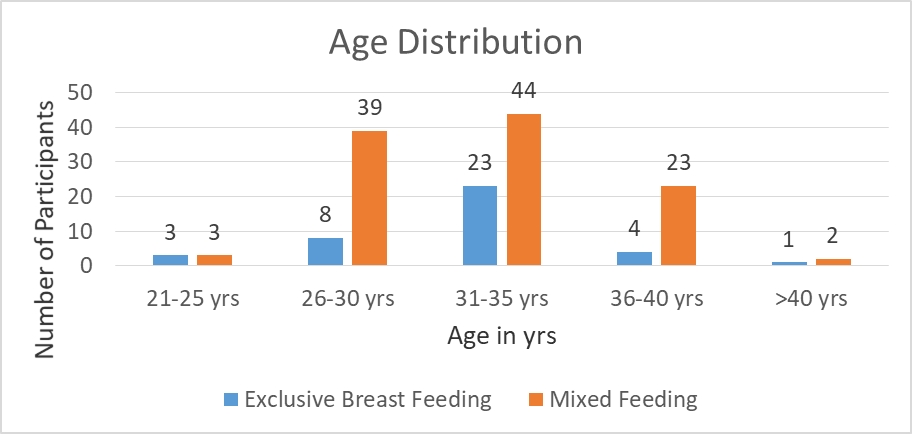
The male to female prevalence ratio was 1:1.22. Out of the1245 positive samples, 685 (55%) were female cases and 560 (45%) were male cases of enteric fever.
The gender wise distribution of significant titers of different antibodies of widal test was also determined and it was found that H antibody of Salmonella typhi was more prevalent in both males (64%) and females (63%).
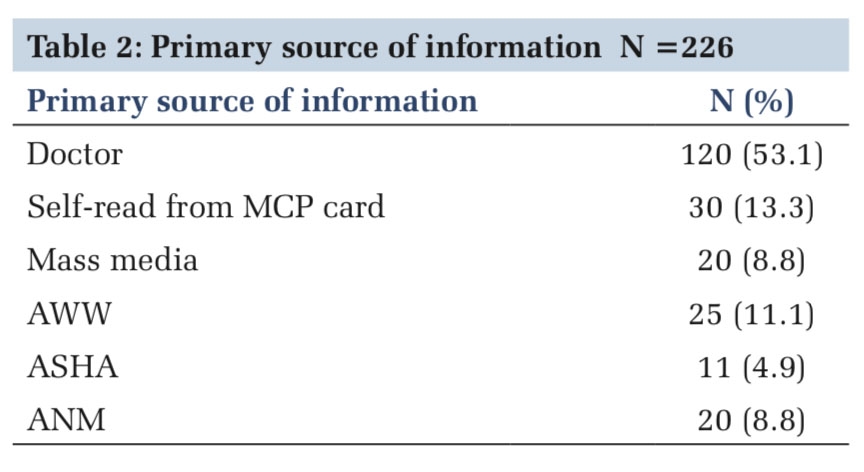
Among widal test positive cases, Adult and paediatric cases were 895 (72%) and 350 (28%) respectively (Figure 3).

Accordingly, age wise distribution of significant titers of different antibodies of widal test was determined and the findings were that the H antibody of Salmonella typhi was more prevalent in both adult (63%) and paediatric population (66%).
Seasonal variation was also seen in the positivity of the widal test. Maximum numbers of positive cases were seen in the months from June to September, which corresponds to the rainy season here in Mumbai (Figure 4).

Lastly, year wise prevalence of widal test positivity was also determined. It was 10.71% in 2015, 10.89% in 2016, 11.64% in 2017, 13.29 % in 2018, 10.54% in 2019, 9.58% in 2020, 11.09% in 2021 and 11.06 % in 2022. Significantly, the widal positivity was seen during June to September over the study period of eight years.
Typhoid fever is a significant health concern in developing countries. 4 Diagnosis of typhoid fever typically relies on isolating Salmonella typhi bacteria from blood, stool, urine, bone marrow, and others body fluids. The situation is exacerbated by the emergence of multi-drug resistant strains of Salmonella typhi, which complicates the treatment and increases the disease burden. 8
Any delay in diagnosing typhoid fever increases the risk of adverse outcomes. 9 Our study focused on the utility of the widal test, which has been extensively used for the serodiagnosis of typhoid fever in developing countries like India.
A fourfold rise in antibody titer in paired sera is often considered diagnostic of typhoid fever. 10 However, obtaining paired sera can be challenging, and specific chemotherapy often has to be initiated based on the results of a single widal test. Shyamala R et al and Kulkarni ML et al, revealed that a single widal test, in association with relevant clinical findings, can still be used as a useful diagnostic tool for typhoid fever. 10, 7
In the present study the prevalence of seropositivity was 11.18% which correlates with Sharma A et al 11, Shyamala R et al 7 and Iyer V et al 12 who reported 12.1%, 8.57% and 12.5% of seroprevalence respectively. Whereas other studies such as Bharadwaj BVG et al 13 reported 27.3 % and Isa MA et al 14 reported 20.6% as the seroprevalence.
In majority of the studies such as, Kiran CMV et al 1, Shyamala R et al 7 and Lall H et al 15 have taken the titre of 1:80 and above as positive. Only two studies have taken a different cut off levels; Nilekar SL 16 et al has taken 1:120 as cut off level and Sharma A et al 11 has taken 1:100 cut off for O antibodies and 1:200 cut off for H antibodies. However, this difference in the diagnostic criteria does not influence the prevalence rates.
In our study maximum positive cases were from females (55%) followed by males (45%) which correlates with Bharadwaj BVG et al 13, Kiran CMV et al 1 and Lall H et al 15. Female preponderance seen in our study probably because, the condition such as malnutrition or anemia; which is more prevalent among women in some areas, can weaken their immune defenses, making them prone to chronic infections with sustained antibody responses. Whereas the study by Sharma A et al 11 showed a slight male preponderance in widal test positivity.
In our study, 72% of the positive cases were adults possibly because the adult population has more and easy access to the healthcare facilities.
In the present study, similar to most of the tropical diseases of infectious origin, a seasonal pattern in the distribution of seropositivity was noted. Accordingly, maximum number of enteric fever cases were seen during the months from June to September which corresponds to the rainy season here in Mumbai. This finding can be correlated with that of Damle AS et al 17, Mangal HN et al 18, Nilekar SL et al 16 and Lall H et al 15; all of these studies reported similar observation. This peak in widal positivity is seen during the rainy season in our study. Accordingly, extensive public health measures can be employed such as the supply of safe and clean drinking water by the local municipal corporation, frequent, regular and strict inspection of the food items sold by the street-side food vendors, improvement in hygiene and sanitation practices in over-crowded areas and health education and awareness of the people regarding hand hygiene and consumption of properly cooked food.
In our study, percentage positivity of TO and TH antibody was 23% and 64% respectively. This is in agreement of Akanksha Sharma et al. 11, and it seen because the O agglutinins appear early and disappear early whereas the H agglutinins appear late and disappear late in the course of infection. Also, the positivity of AH and BH antibody was 9% and 4% respectively. Similar findings were noted in two studies, namely Sharma A et al. 11 and Lall H et al. 15
It has been reported that Salmonella paratyphi A constitutes about 1.3% to 15% of enteric fever cases in the study by Basu S et al. 19 Damle AS et al. 17 reported this percentage to be 2% in his study. Our findings (8.75%) are in agreement with these studies. Salmonella paratyphi B infection is rare in India as reported by John J et al 20 and in accordance, our study showed 3.93% of paratyphoid B infection.
In the present study comparison of widal test results with blood culture and clot culture is not done. Also, the widal test results were based on the rise in antibody titre of a single serum sample, instead of interpretation of the widal test positivity based on the rise in titres in paired serum sample.
There were certain confounding factors affecting the results such as anamnestic response, individuals with prior immunization with typhoid vaccines, carrier state, individuals receiving empirical antibiotic therapy prior to the widal testing and if the widal test is done in early stage (1st week of illness) or if the test is done in late stages of the disease.
In conclusion, the widal test is an easy, inexpensive, and relatively non-invasive diagnostic tool, which can be valuable in situations where blood culture cannot be obtained or is not feasible.
Understanding the local seroprevalence rates of widal positivity helps clinicians weigh the widal test results against clinical symptoms and other diagnostic methods and subsequently aid them in the diagnosis of enteric fever. Also, tracking the widal test prevalence, helps public health officials monitor trends in enteric fever, detect outbreaks early, and implement control measures like vaccination programs or sanitation improvements.
The diagnosis of enteric fever from an early, single specimen is therapeutically valuable because early diagnosis is crucial in typhoid fever. Delay in the treatment can lead to fatal complications such as perforation or hemorrhage of the small bowel.
Thus, the widal test can be of diagnostic value in the early stage of the disease and can help in reducing morbidity and mortality.
Funding: Nil
Conflict of interest: Nil
Author contribution: All the authors contributed equall to the manuscript
Subscribe now for latest articles and news.