Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i03.015
Year: 2020, Volume: 6, Issue: 3, Pages: 85-88
Case Report
N Naveen1, T S Purushotham1, H R Pallavi2, Hanumantha Basappa Vaggara2
1Assistant Professor, Department of Plastic and Reconstructive Surgery, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India,
2Post Graduate, Department of Plastic and Reconstructive Surgery, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India
Address for correspondence:
H R Pallavi, Opposite BGS Nilaya, Javranahalli, B G Nagara, Nagamangala, Mandya - 571 448, Karnataka, India. Phone: +91- 9986629321. E-mail: [email protected]
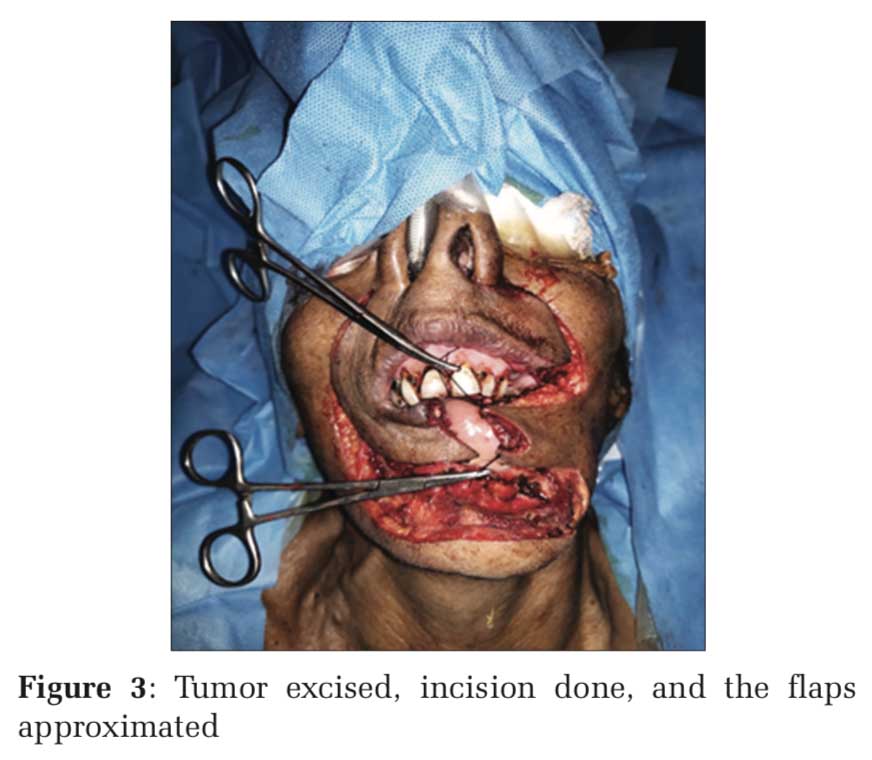
Carcinoma of the lip is a common head-and-neck region malignancy more commonly affecting the lower lip (>90%) with squamous cell variant being the most common (95%). Surgical excision of the tumor is the choice of treatment with reconstruction of the ensuing defect. Although various techniques are prescribed, the pick of surgery for reconstruction of full thickness defect in lower lip remains to contest. In this case account, a 65-year-old elderly female, who presented with near-total involvement of the lower lip to squamous cell carcinoma, underwent full thickness lip defect reconstruction combining two classical flaps: The Karapandzic Flap (KF) and Bernard Burrow Webster Flap (BBWF). KF being a single stage procedure has the advantage of being fully innervated with the preservation of sensation and motor function. The BBWF is an excellent procedure for repairing defects that affect more than one-third of the lower lip. It allows use of similar local tissue in a single sitting to cover the defect though at the cost of attaining a dynamic continuity. Thus combining both these flaps in our case advantages of both flaps has been utilized.
KEY WORDS: Karapandzic flap, Bernard Burrow Webster flap, lower lip reconstruction, squamous cell carcinoma.
IntroductionThe lips are dynamic structures and have a vital key not only in eating, drinking, speech but also play a key role in an individual’s appearance, self-esteem, facial harmony, and expression.[1] Squamous cell carcinoma (SCC) of the lip is second only to skin cancer in terms of frequency in the head and neck.[2] Wide excision of the tumor with negative margins,[3] followed by reconstruction of the subsequent tissue deficit with variable thickness flap, is the gold standard treatment.[4] Meticulous planning and careful selection of a suitable reconstruction procedure are necessary to recreate the tissue lost to be drawn from elsewhere, in treating tumors of large sizes that may have become infiltrative and destructive. Functional and aesthetic restoration of the lip structure is essential while reconstructing a new lip. Furthermore, it is necessary to preserve skin sensitivity as far as possible to provide a proprioceptive mechanism to lip movement, speech, and salivary continence.[1] However, as in any other plastic surgery procedure, it is elemental to choose the right procedure for reconstruction of the lower defect adapted to the individual depending on lip defect extension, location, and thickness with factors such as defect size, availability of healthy tissue, and involvement of the commissures.[5] Thus, it is crucial for the operating surgeon to attain a balance in aesthetic appearance with proper function of the oral sphincter. To simplify things, lip defects have been divided into – defect only (a) at the cutaneous part of the lip; (b) in the lip vermilion; and (c) full-thickness defect; varying according to the size of the defect area – (a) < 1/3rd, (b) between 1/3 and 2/3, and (c) near-total or total.[6] The latter defects of >2/3 of the lower lip may be favorably closed with Karapandzic Flap (KF) or Bernard Burrow Webster Flap (BBWF). Karapandzic was the first to describe innervated muco – musculocutaneous flaps that provided post- operative functionality.[7] Christian Bernard, in 1853, described a surgical technique using full-thickness Burrow triangles in the nasolabial sulcus to enable medial advancement of the malar flaps. In 1960, this was modified by Webster et al.[8] The Bernard Webster flap is used to reconstruct large lower lip defects recreating the commissures by means of medial cheek advancement along with the remaining lip tissue.[9] Over time, there have been many modifications of the technique with preservation of the innervated muscle fibers of orbicularis muscle by careful tissue dissection without full muscle transection at the commissure level.[10] Here, we present our experience to reconstruct a near-total lower lip defect using both KF and BBWF together. |
Case ReportThis case is of a 65-year-old lady presenting with ulceroproliferative lesion occupying almost the entire lower lip which grew rapidly over a period of 6–7 weeks. Patient had a H/O tobacco and betel nut chewing over past 40 years. Examination revealed that ulceroproliferative growth was occupying 80–85% on the mucosal side of the lower lip extending from white roll to alveolar ridge and bleed on touch [Figure 1]. No palpable regional lymphadenopathy was noted. Tissue biopsy suggested well-differentiated SCC. Metastatic workup yielded negative yielded negative. Patient had no comorbidities. |
DiscussionIn SCC of the lip, radical excision with clear microscopic margins is the treatment of choice as it is associated with satisfactory disease-free survival.[11] KF and the BBWF are 2, time tested techniques in reconstruction of the lower lip. Each of these flaps has their own advantages and disadvantages. However, by combining both, we can reap advantage of preservation of the sensibility and motility of the lower lip given by KF and also take advantage of the larger side mobilization of BBWF, especially because in our case the defect occupied about 85% of the lower lip. Use of local flaps for reconstruction in full thickness defects of facial area, especially the lip, rather than regional or free flaps, is preferred. This is because of the advantages of retaining sensation, better motility of the reconstructed area, commissure preservation and tissue matching for functionality and esthetics that the local flaps offer.
|
References |
Subscribe now for latest articles and news.