Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2019.v05i01.008
Year: 2019, Volume: 5, Issue: 1, Pages: 42-46
Original Article
Pınar D. Yilmaz1, Cengiz Kadiyoran2
1Assistant Professor, Department of Radiology, Necmettin Erbakan University, Meram Medical Faculty, Konya, Turkey,
2Radiology Specialist, Department of Radiology, Necmettin Erbakan University, Meram Medical Faculty, Konya, Turkey
Address for correspondence:
Pınar D. Yilmaz, Department of Radiology, Necmettin Erbakan University, Meram Faculty of Medicine, Konya, Turkey. Phone: +90 5057798424. E-mail: [email protected]
Objective: We aimed to determine the relationship between microalbuminuria and atherosclerosis in patients with Type II diabetes and evaluate the parameters of extracranial internal carotid artery (ICA) duplex ultrasonographic scanning; pulsatile index (PI) and resistive index (RI) in relation to microalbuminuria, which is an indicator of microangiopathy.
Materials and Methods: The study population was 42 patients with Type II diabetes. The parameters of ICA duplex ultrasonographic scanning, intima-media thickness (IMT) of common carotid artery, and urine albumin-to-creatinine ratio were measured, and their relationships were analyzed.
Results:A total of 42 patients were included in the study. Microalbuminuria was detected in all of five cases who had plaque in ICA. Of the 35 patients who had no plaque, microalbuminuria was not detected in 23 cases (65.7%). This shows that atherosclerosis may correlate well with the progression of microangiopathy. Microalbuminuria was detected in 6 cases (85.7%) with common carotid artery wall IMT ≥1 mm, but microalbuminuria was not detected in 1 (14.3%) case. This shows a statistically significant presence of concurrent microalbuminuria in Type II diabetic patients with intima-media thickness increase. PI and RI values of ICA were not differentiated in microalbuminuria and non-microalbuminuria group. Hence, the PI and RI values are not available to use as an indicator of microangiopathy in patients with diabetes.
Conclusions:Atherosclerosis is correlated well with the progression of microangiopathy in Type II diabetic patients. Diabetic patients with microalbuminuria can be examined for carotid arteries with B mode and color Doppler sonography to detect atherosclerosis.
KEY WORDS:Atherosclerosis, duplex ultrasonography, microalbuminuria, microangiopathy, type II diabetes.
Diabetes is undoubtedly one of the most important health problems, and nowadays, one in every 11 adults has diabetes, 90% of whom are Type II diabetics.[1]
Death rates due to diabetes and its complications are more serious than death from infectious diseases. The majority of cases with diabetes are Type II diabetes. In Type II diabetes cases, many complications arise as a result of angiopathy development. Therefore, early recognition of angiopathy is of great importance in the control of the disease and its complications.
Increased intima-media thickness (IMT) in the carotid system is a good indicator of the development of atherosclerosis and is associated with cardiovascular and cerebrovascular complications. Along with microangiopathy, atherosclerotic changes are also beginning. For this reason, the IMT increase in the main carotid artery and plaque development can be used as an indicator of cardiovascular and cerebrovascular disease risk in the case of microangiopathy.[2]
Microalbuminuria has been suggested as a marker of microangiopathy underlying diabetic complications and the relationship between carotid IMT increase and microalbuminuria has been evaluated and correlations between these two parameters have been demonstrated.[3] Albuminuria is a high-risk factor in hypertensives and diabetics in the general population. The relationship between albuminuria and cardiovascular events continues even after the exclusion of risk factors. The risk level increases in direct proportion to the amount of urine albumin.[4] The albumin-creatinine ratio is used to evaluate protein content in spot urine and is an auxiliary parameter in the detection of microalbuminuria.
The aim of this study was to evaluate the association of carotid artery atherosclerosis with microalbuminuria in Type II diabetes and to determine the relationship between Doppler flow parameters, resistive index (RI) and pulsatile index (PI) values obtained from the extracranial internal carotid artery (ICA) with microangiopathy and microalbuminuria and to contribute to the control of the disease.
Ethical approval for this study (Registration No. 2011–2017) was provided by the Ethics Committee of Ankara Numune Training and Research Hospital, Turkey, on August 2011.
The study included 42 people diagnosed with Type II diabetes, according to the American Diabetes Association diagnostic criteria and followed up. Patients with major cerebrovascular, cardiovascular, and renal disease, patients with drug use history other than antidiabetic drug therapy, and patients with urinary infection, smokers, and pregnancies were excluded from the study. All subjects included in the study were asked to measure urine albumin/ creatinine (u-ACR) in the spot urine sample obtained in the morning. The threshold for microalbuminuria is 30 uq/mg (American Diabetes Association).[5]
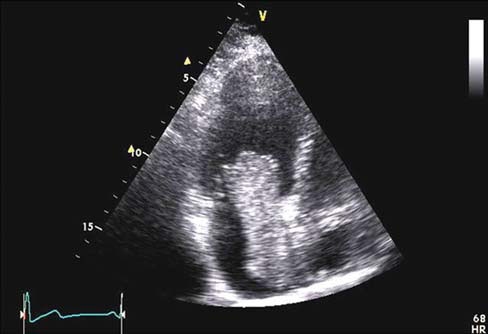
In all cases, a carotid system, Doppler ultrasonography examination was performed in a supine position, neck slightly extensor, and reversed position on the head side. Extracranial carotid system B-mode, color Doppler, and pulse Doppler examinations were evaluated on both sides using a 7 MHz linear transducer with General Electric Logic 9 US. B-mode examination revealed plaque presence on transverse and longitudinal planes.
The distance between the first echogenic line adjacent to the vessel lumen and the second echogenic line was measured as IMT from 2 cm proximal to the main bilateral main carotid artery bulb level to provide standard. Later, both carotid arteries were scanned with color Doppler US to investigate the presence of stenoal fused defect and/or color scattering. Peak systolic velocity, end diastolic velocity, and PI and RI values were obtained by conducting a spectral examination of the longitudinal bit from 1 cm distal to the bilateral ICA bifurcation level. The Doppler angle was kept between 45 and 60°.
An SPSS program for Windows was used for statistical analysis of the data. Statistical comparisons were considered significant at P < 0.05 for p value obtained as a result. Receiver operating characteristics (ROC) analysis test was used to examine the sensitivity and specificity of the Chi-square test, PI and RI for the detection of microangiopathies in comparison of the parameters of the cases.
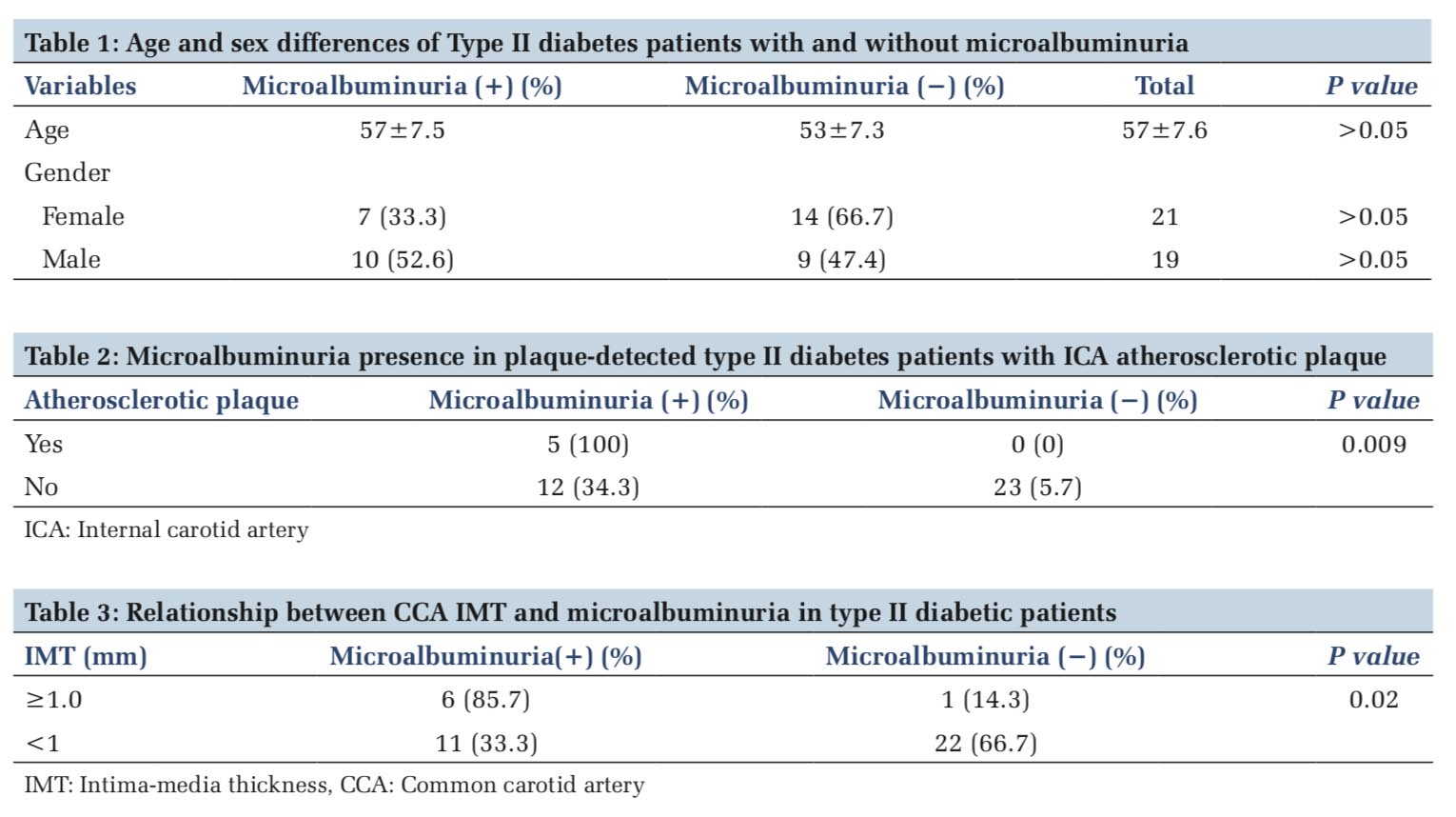
A total of 42patients followed-up with TypeII diabetes mellitus were enrolled. One of the cases was excluded from the study due to the presence of the antihypertensive drug use story, and the second was cardiovascular disease. The mean age of the patients is 57 ± 7.6. Microalbuminuria was detected in 17 patients and microalbuminuria was not detected in 23 patients. The mean age of the patient group with microalbuminuria was 57 ± 7.5, the mean age of the group without microalbuminuria was 53 ± 7.3, and there was no statistical difference in the distribution of patients by age. 7 (41.2%) of the patients with microalbuminuria were female and 10 (58.8%) were male; 14 (60.9%) of the patients without microalbuminuria were female and 9 (39.1%) were male. There is no significant gender difference in the distribution of patients to the groups (Table 1).
Plaques in the carotid artery were detected in five of the patients included in the study and microalbuminuria was detected in all of these 5 patients (100%). In 23 (65.7%) patients, whose plaque was not detected, it was understood that there was no microalbuminuria. Microalbuminuria was detected in 12 (34.3%) patients without plaque in the carotid system. These findings that microvascular disease was also developed in patients with Type II diabetes mellitus as a carotid system (P < 0.05).
The data obtained are summarized in Table 2. In the study, microalbuminuria was detected in 6 (85.7%) of cases with carotid artery wall IMT ≥1 mm and 1 (14.3%) indole microalbuminuria was not detected. These findings, the presence of concurrent microalbuminuria was statistically significant (P < 0.05) in patients with Type II diabetes who had an IMT increase (Table 3).
PI and RI values obtained from the right ICAs of the cases were not differentiated according to the ROC analysis in patients with and without microalbuminuria, so the cutoff value according to sensitivity and specificity could not be determined. This statistic shows that the PI and RI values obtained from ICA cannot be used as a parameter in showing the presence of microangiopathy in type II diabetic cases.
In diabetic patients, the frequency of acute metabolic complications has gradually decreased with appropriate treatment modalities. Early diagnosis and treatment of chronic degenerative complications with the prolongation of the life span of patients have become more important in the control of the disease. Retinopathy, nephropathy and neuropathy are microvascular complications of diabetes, development of atherosclerosis and related cerebrovascular events, myocardial infarction, peripheral vascular diseases are known as macrovascular complications. In our study, we examined the utility of color Doppler US, especially B-mode imaging as an imaging modality that would be useful for early diagnosis of macrovascular complications and for the control of disease.
Epidemiologic studies have shown that the increase in the thickness of the increased carotid artery intima media correlates with the risks of myocardial infarction and stroke.[6,7]
Carotid IMT, one of the subclinical markers of arterial disease, is considered an independent indicator of cardiovascular mortality in patients with coronary heart disease, stroke, and end-stage renal disease. İt is used as a precursor of cardiovascular disease in autoimmune diseases without cardiovascular risk factors.[8] It is unclear how mechanisms associated with microalbuminuria increase cardiovascular risk, but traditional risk factors, inflammatory markers, and endothelial dysfunction are the main reasons for increased cardiovascular risk in individuals with microalbuminuria.[9]
Yokoyama et al. reported that patients with microalbuminuria had thicker carotid IMT than normoalbuminuric patients.[10] When our patient population was evaluated, the presence of microalbuminuria was remarkable in the patient population in which IMT was measured as a thickness increase. There are many studies on the risk factors of atherosclerosis in carotid arteries. It has been shown that carotid atherosclerosis is more prominent in patients with diabetes who have coronary artery disease and who have hypertension in the study performed by Adaikappan et al.[11] and Melidonis et al.[12]
In our study, we evaluated the relationship between microangiopathy and carotid artery atherosclerosis in diabetic patients; we aimed to evaluate the imaging modalities of early atherosclerosis in patients with major cardiovascular, cerebrovascular, and renal disease. Therefore, we excluded two patients with a history of cardiovascular disease and hypertension. Microalbuminuria has been suggested as a marker of microangiopathy. Several threshold values for u-ACR in microalbuminuria have been reported.[13] In our study, we used a 30 μg/mg threshold for microalbuminuria as determined by the American Diabetes Association.[5] Microalbuminuria can be used as a marker for cardiovascular risk in diabetic patients.[14] As a matter of fact, the relationship between carotid IMT increase and microalbuminuria was evaluated and the correlation between these two parameters was shown.
The increase in IMT observed in the carotid system is indicative of the development of atherosclerosis and has been shown to be associated with cardiovascular and cerebrovascular complications.[2] Atherosclerotic changes with microvascular disease are also beginning in diabetic patients.[3] Therefore, an increase in IMT in the main carotid artery can be used as an indicator of cardiovascular and cerebrovascular disease risk in a group of patients with microangiopathy.[2]
In our study, microalbuminuria indicating the presence of microangiopathy was detected in all five patients with atherosclerotic plaque in the ICA, indicating that microangiopathy was also evident when macrovascular complications started in diabetic cases. In addition, our study evaluated the relationship between IMT increase and microalbuminuria, a marker of atherosclerosis development, to detect the development of atherosclerosis earlier in diabetic patients and to reveal cardiovascular, cerebrovascular disease risk. The presence of microalbuminuria was found to be greater than those of < 1 mm. These findings have shown that IMT measurement from the common carotid artery can be used to determine the risk of major cardiovascular and cerebrovascular disease in patients with microalbuminuria.
The results obtained during the studies revealed the relationship between microangiopathic complications of diabetes and poor metabolic control. The association of microvascular complications with age and gender is not clear. In our study, there was no difference in age and sex distribution in the case group with and without microalbuminuria.
PI and RI are spectral Doppler velocimetry rates used to determine vascular resistance. In his study, Fukuhara investigated the relationship between microalbuminuria, a marker of microangiopathy in patients with Type II diabetes, and PI value obtained from cervical ICA, suggesting that microangiopathic changes in cerebral vascular structures increase the PI values obtained from intracerebral vascular pressure, and thus, cervical ICA revealed that microalbuminuria could be detected with the highest specificity and sensitivity at PI values of 1.15 and above. With this result, he suggested that PI value could be used as a parameter in microangiopathy.[15]
In our study, the cutoff value according to sensitivity and specificity could not be determined because the PI and RI values obtained from the cervical ICA in Type II diabetic patients were not differentiated according to ROC analysis in microalbuminuria and non-microalbuminuria. This statistic shows that the PI and RI values obtained from ICA cannot be used as a parameter in showing the presence of microangiopathy in type II diabetic cases.
In diabetes, atherosclerosis and related complications start earlier and become more common. About 65–75% of adult diabetics die from diseases related to the heart and major vascular disease. In conclusion, albuminuria is an independent indicator of vascular risk factors, micro- and macro-vascular disease in Type 2 diabetic patients and can be used as a marker of early cerebrovascular/cardiovascular disease.
Carotid IMT is also an independent predictor of atherosclerosis. Nowadays, carotid atherosclerosis can be determined accurately at the earliest stage with using B-mode sonography and the grade can be determined by Doppler examination. In our study, we observed that microvascular complications and carotid artery atherosclerosis were parallel to each other in cases followed by type II diabetes. Therefore, B-mode and color Doppler sonography is a non-invasive method that can be recommended for diagnosis of carotid artery atherosclerosis early and prevention of complications that are followed by type II diabetes diagnosis and microalbuminuria. We also found that the PI and RI values obtained from ICA in the presence of microangiopathy in patients with Type II diabetes could not be used as a parameter in our study.
Subscribe now for latest articles and news.