Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i3.24.203
Year: 2024, Volume: 10, Issue: 3, Pages: 327-332
Case Series
K N Rajesh1 , H R Pallavi2 , Suprabha R Hegde3 , Akshata M Goudar3
1Assosciate professor, Department of General Surgery, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India,
2Assistant professor, Department of General Surgery, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India,
3 Junior resident, Department of General Surgery, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India
Address for correspondence: Suprabha R Hegde, Junior resident, Department of General Surgery, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India.
E-mail: [email protected]
Received Date:01 July 2024, Accepted Date:06 August 2024, Published Date:28 October 2024
Intestinal malrotation is arrested normal rotation of the gut during development. Malrotation seldom presents in adults and often not timely diagnosed. These diagnostically challenging cases may lead to worser outcomes, with increase in morbidity and motility compared to paediatric age group. 1 We present six such rare diagnostically challenging cases of adult presentation of malrotation of gut. Five rare presentations of malrotation of gut during a period of three years (2020- 2023). Outcome was analysed retrospectively. Among the five patients, four were male and one was female. Youngest patient was 18 years and the oldest in the study was an 80-year-old male. All patients presented with multiple episodes of bilious vomiting and vague symptoms of pain abdomen. All five had varying degree of malrotation of gut. Patients underwent Erect Xray abdomen, and contrast-enhanced computed tomography abdomen and diagnostic laparotomy to confirm the diagnosis. All five patients underwent Ladd procedure or division of peritoneal bands with one requiring right hemicolectomy with end ileostomy. Four had favourable outcomes post procedure whereas one underwent reversal of end ileostomy procedure two months post hemicolectomy.
Keywords: Malrotation gut, Peritoneal band, Ladd’s procedure, Volvulus
A congenital defect known as malrotation arises when the intestines fail to fully rotate along the superior mesenteric artery's axis during the embryonic development. This anomaly usually presents in the first month of life and is a rare presentation in the adults 2. The majority of adult cases remain asymptomatic during life and are discovered incidentally, until they lead to acute or chronic discomfort in the abdomen. Midgut volvulus is the most common clinical manifestation in adults, frequently self-limiting and recurring but sometimes contributing to an abdominal crisis 3. The extent of circulatory compromise and its duration influence the severity.
Unlike adults who may present with unusual symptoms such pain drawing to the legs, chronic pain in the abdomen, and sporadic episodes of bilious vomiting, children with malrotation typically show clear indicators of abdominal distension, vomiting, and failure to thrive. Paediatric patients who present early with midgut volvulus, require immediate surgical intervention. 4
There are different types of midgut malrotation; a. non-rotation b. incomplete rotation c. reverse rotation d. anomalous fixation of mesentery. 5
The interventional approach is surgery, as inability to do so may result in intestinal gangrene which worsens the morbidity and mortality. Ladd's procedure is the preferable approach. 2
Yin et. al concluded from their study that due to ambiguous clinical signs, adult congenital intestinal malrotation is a rare condition that is frequently misdiagnosed. The mainstay of care for this illness continues to be surgery. Enhancing surgical results can be achieved by combining the classic Ladd6
Bhatia et al., further observed that to diagnose adult cases of intestinal malrotation, a strong index of suspicion is required. Patients who have recurring episodes of bilious vomiting and abdominal discomfort but no history of TB or evidence for an adhesive aetiology should be suspected of this illness. An ultrasonography looking for the superior mesenteric vessels' reversed relation might be highly helpful in an emergency situation. Early detection will stop this disease's fatal consequences. 7
Successful diagnosis and effective management of five such cases at our institution have been described here. These cases were followed up monthly for the first three months and thereon every third month for one year post surgery.
A 20 year old male, came to emergency with history of pain in the upper abdomen, since 2 days which was moderate in intensity. Pain was associated with multiple episodes (~10 episodes) of vomiting, non-projectile. Clinically, abdomen was mildly distended with tenderness in right hypochondrium, with no obvious guarding or rigidity. Hyper peristaltic bowel sounds were present. Xray showed multiple air fluid levels suggestive of intestinal obstruction and CECT abdomen and pelvis showed mid gut volvulus with intestinal malrotation. Exploratory laparotomy showed 720-degree malrotation of the mesentery, transverse colon malrotation with mesentery. Ladds bands passing over the loop of the duodenum, connecting the caecum to the lateral abdominal wall with Ileo-caecal junction pulled right sub-hepatic region (Figure 2). Peritoneal bands and ladd’s bands to the anterior lateral abdominal walls and interbowel membranous adhesions with Peritoneal bands were divided, small bowel was released from membranous adhesions, evisceration of bowel with counter clockwise detorsion of the bowel done and Ladd bands excised. Congestion of the ilial loops improved after derotation. Appendicectomy was done. Patient was followed up and no signs of obstruction was observed (Figure 1).

80-year-old male, came to emergency with complaints pain abdomen since two days, continuous type, moderate intensity and non-radiating. Pain was associated with eight to ten episodes of vomiting, non-bilious. Clinically, abdomen was distended with diffuse tenderness, with no obvious guarding or rigidity. Xray erect abdomen showed multiple air fluid levels. CECT abdomen and pelvis done showed duodenojejunal flexure is on the right side of the midline with swirling of mesentery and mesenteric vessels altered SMA, SMA relation with jejunal loops predominantly in the right quadrant of the abdomen and a few jejunal loops lateral to the ascending colon in the right paracolic gutter. Dilatation of the proximal jejuna loops s/o intestinal malrotation with midgut volvulus and subacute intestinal obstruction with Minimal ascites. Exploratory laparotomy showed 360-degree malrotation of the gut, malrotation of the mesentery, transverse colon malrotation with mesentery. Multiple bands noted interbowel and anterior abdominal wall. Multiple bands noted interbowel and anterior abdominal wall. Multiple bands noted interbowel and anterior abdominal wall. Peritoneal bands were divided with a combination of hand dissection and fine scissors. Small bowel released from membranous adhesions, (Figure 2) malpositioned DJ flexure released and Ladd bands excised. Counter clockwise detorsion of the bowel done. No bowel congestion noted post derotation of the small bowel. Appendectomy done. Patient was followed up and no signs of obstruction was observed.
42-year-old male patient came with complaints of pain abdomen, moderate in intensity, associated with multiple episodes of bilious vomiting 10 -12 episodes, and clinically, abdomen was distended with diffuse tenderness, with no obvious guarding or rigidity. Xray erect abdomen showed multiple air fluid levels. CECT abdomen and pelvis showed twisting of the proximal jejunum (just distal to the duodenojejunal junction) and ileal loops and mesentery with altered SMA &SMV relationship and swirling of the mesenteric vessels (whirlpool sign) – s/o mesenteric volvulus. Clumping of proximal jejunal loops noted in the right side of the abdomen -probably represents transmesentric hernia. Few of the small bowel loops are located in the right paracolic gutter, lateral to the ascending colon and displacing the ascending colon medially and caecum anteriorly – likely peri caecal internal hernia. Exploratory laparotomy there was twisting of the mesentery of small bowel loop, ascending colon displaced medially and caecum anteriorly, visualised at epigastrium. Gangrene of the bowel loops from distal part of ileum involving up to the ascending colon. Derotation of the colon and Right hemicolectomy with temporary end ileostomy was done after reducing the transmesenteric hernia. Ileostomy reversal was done two months after the hemicolectomy. Patient was followed up and no signs of obstruction was observed (Figure 2).

80-year-old male, came to emergency with complaints pain abdomen in the last three days, continuous type, severe intensity, and non-radiating. Pain was associated with three-day history of constipation, abdominal distension for 3 days. Patient also complained of multiple episodes of vomiting for one day which was non projectile and bilious. Clinically, abdomen was distended with in right hypochondrial tenderness, with no obvious guarding or rigidity. Xray erect abdomen showed multiple air fluid levels. CECT abdomen showed small bowel loops predominantly over the right quadrant of the abdomen, twisting of the mesentery with twirling of mesenteric vessels at its root with congestion of the ileum distal to the twisting, f/s/o malrotation of gut with mid gut volvulus with Mild ascites. During Exploratory laparotomy malrotation of gut, with ileal loop rotated 270 degrees along the superior mesenteric axis with peritoneal adhesions to the anterior abdominal wall as well intercolonic membranous adhesions lateral abdominal wall (ladd’s bands). Small bowel released from membranous adhesions, evisceration of bowel with counter clockwise detorsion of 270 degrees of the bowel done and Ladd bands and peritoneal adhesions excised. Congestion of the ileal loops improved after derotation. Appendicectomy was done. Patient was followed up and no signs of obstruction was observed.
40-year-old female patient presented to casualty with pain abdomen abdominal distension in the past three days. Patient also complained of multiple episodes of vomiting since day which was non projectile and bilious. Clinically, abdomen was distended with in diffuse tenderness, with no obvious guarding or rigidity. Xray erect abdomen showed multiple air fluid levels. CECT abdomen showed small bowel loops predominantly over the right quadrant of the abdomen, twisting of the mesentery with twirling of mesenteric vessels at its root with congestion of the ileum distal to the twisting, f/s/o malrotation of gut with mid gut volvulus with Mild ascites. Exploratory laparotomy showed Malrotation of gut with congenital ileal bands causing 180-degree volvulus of intestine with mild congestion. Small bowel released from membranous adhesions, evisceration of bowel with counter clockwise detorsion of the bowel done and Ladd bands excised along with ileal band excised. Peritoneal bands were divided with electrocautery fine scissor. Congestion of the ileal loops improved after counter clockwise derotation. Appendicectomy was done. Patient was followed up and no signs of obstruction was observed (Figure 3).

|
Case |
Age (Years) / Sex |
Operative Findings |
Operative Procedure |
Outcome |
|
A |
20/M |
720 Degree malrotation of the mesentry with congestion of the ileal loops |
Counter clockwise derotation with ladd procedure |
Improved |
|
B |
80/M |
360 Degree malrotation of transverse colon with mesentry with multiple peritoneal bands |
Counter clockwise derotation and adhesiolysis with ladd procedure |
Improved |
|
C |
42/M |
Twisting of the mesentry of small bowel loop and ascending colon and gangrene of the distal ileum upto ascending colon |
Derotation of colon and right hemicolectomy with temporary end ileostomy, reduction of trans mesentric hernia |
Ileostomy reversal done two months post right hemicolectomy Improved |
|
D |
80/M |
270 Degree malrotation of ileum with mesentry with peritoneal bands |
Counter clockwise derotation and adhesiolysis with ladd procedure |
Improved |
|
E |
40/F |
180 Degree volvulus of ileum with mild congestion, peritoneal bands |
Manual with counter clockwise derotation and adhesiolysis with ladd procedure |
Improved |
The intestinal development has been classified into three phases. Stage I occurs between the 5th and 10th weeks of pregnancy. It consists of the midgut being extruded into the extraembryonic cavity, rotating 90 degrees counterclockwise, and returning to the foetal abdomen. Stage II begins in the 11th week and involves a further counterclockwise rotation within the abdominal cavity, completing a 270° rotation. The duodenum rotates caudally to the artery, and its C-loop follows it. The transverse and ascending colon show the rotation of the cecum cephalad to the artery. Fusion and anchoring of the mesentery occur during Stage III. The duodenum becomes retroperitoneally fixed in its third section, and becomes intraperitoneal at the Treitz ligament, and the cecum becomes fixed by lateral peritoneal bands to the lateral abdominal wall. 8
Intestinal malrotation is defined as any variation from the midgut's typical 270° counterclockwise rotation (stage II). When it fails to rotate, the entire small bowel stays on the right side of the abdomen, the colon is on the left, and absence of Treitz ligament, resulting in malrotation or incomplete rotation of the intestines and the intestine's subsequent positioning with abnormal adhesions. 9 Volvulus can arise owing to clockwise twisting of the intestine around the superior mesenteric artery axis, which can lead to ischemia and necrosis of the small bowel, when these abnormal adhesions combine with a shorter mesentery. Ladd's bands are dense peritoneal bands from the caecum to the lateral abdominal wall and across the duodenum are also associated with malrotation, which can induce duodenal obstruction. 10
Adults have a 0.2% chance of having intestinal malrotation. 11 The abnormality is frequently discovered by chance during a laparotomy. 12 CECT abdomen and pelvis is the investigation of choice to diagnose such cases with vague abdominal symptoms. The imaging shows the small bowel on the right and the colon on the left. Angiography reveals an abnormality in the SMA/SMV axis; whirl sign-SMA moving around SMV. Small intestine to the right, cecum to the left. Physical examination and abdominal imaging, followed by diagnostic laparoscopy/laparotomy and Ladd's operation/ division of peritoneal bands are the therapy of choice in adults. 13
These developmental anomalies are often detected during exploratory laparotomy and, if discovered by chance, should be operated on to reduce the danger of future intestinal ischemia due to volvulus. 14
Genetic alteration in the gene BCL6's disruption the signalling route that is essential for intestinal rotation, thus resulting in the caecum being positioned abnormally, and fibrotic band formation from the caecum to the retroperitoneum crossing over the duodenum, acting as a potential point for obstruction. A volvulus and consequent midgut ischaemia can occur when the displaced midgut rotates around a pedicle formed by its short mesentery. 5
In our set up, the general principle used in this operative procedure was division of the peritoneal bands/ladd’s bands after untwisting of bowel and mesentery, bowel was followed up from duodeno jejunal junction to ileocecal junction, followed by appendectomy was performed. We observed that division of peritoneal bands and ladd’s band procedure with timely intervention provided good outcome.
This surgery aims to prevent acute volvulus by positioning the small intestine in a non-rotating posture and extending the base of the mesentery. Appendectomy may be necessary to diagnose future appendicitis in locations other than the typical lower right quadrant. 8
Case series and reports by Haqqani M et al. Butterworth et al. reached to a similar conclusion that the Ladd`s procedure is still the gold standard treatment for intestinal malrotation and a high clinical suspicion, prompt diagnosis and intervention are critical to a favourable outcome in symptomatic adult presentations. 15, 16
Malrotation of the gut in adults, though a rare clinical entity, presents with a broad spectrum of symptoms that often overlap with other abdominal conditions, making diagnosis challenging. This case series underscores the importance of maintaining a high index of suspicion, particularly in patients presenting with recurrent abdominal pain, unexplained gastrointestinal symptoms, or acute abdomen without a clear cause. Timely imaging, primarily with contrast-enhanced CT, remains crucial for diagnosis. Early surgical intervention, whether laparoscopic or open, can significantly alleviate symptoms and prevent complications such as volvulus or bowel ischemia. Recognizing the diverse presentations and incorporating a multidisciplinary approach can improve patient outcomes, reduce morbidity, and avoid unnecessary delays in treatment.
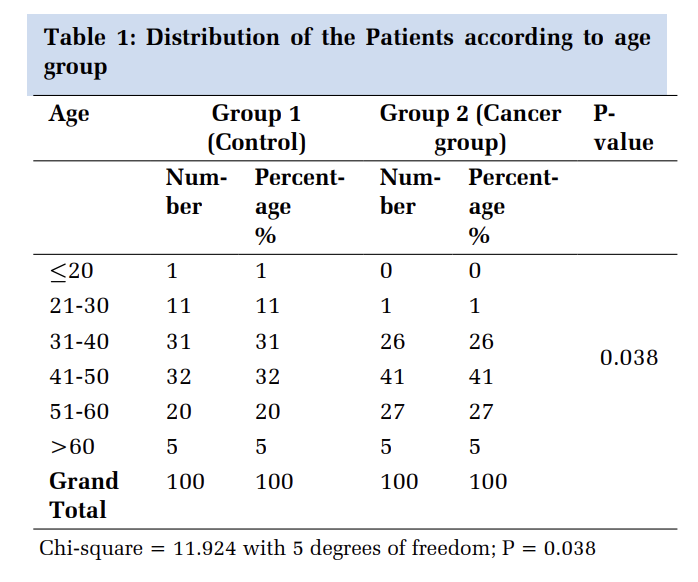
Subscribe now for latest articles and news.