Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i02.003
Year: 2020, Volume: 6, Issue: 2, Pages: 14-18
Original Article
Gurpuneet S Basra1, Ankur Joshi2, Alok Jaiswal3, Arpit Garg4
1Assistant Professor, Department of Anaesthesiology and Critical Care, Air Force Hospital, Kanpur, Uttar Pradesh India,
2Assistant Professor, Department of Anaesthesiology and Critical Care, Army Hospital Research and Referral, New Delhi, India,
3Assistant Professor, Department of Anaesthesiology and Critical Care, Armed Forces Medical College, Pune, Maharashtra, India,
4Assistant Professor, Department of Anaesthesiology and Critical Care, Command Hospital, Lucknow, Uttar Pradesh, India
Address for correspondence:
Dr. Arpit Garg, Assistant Professor, Department of Anaesthesiology and Critical Care, Command Hospital, Cantonment, Lucknow - 226 002, Uttar Pradesh, India. Phone: +91-9145431205. E-mail: [email protected]
Background: Sedation and anesthesia are required for procedures in pediatric patients for cardiac catheterization. In this study, we compare anesthetic agents in providing ideal anesthetic conditions with hemodynamic stability.
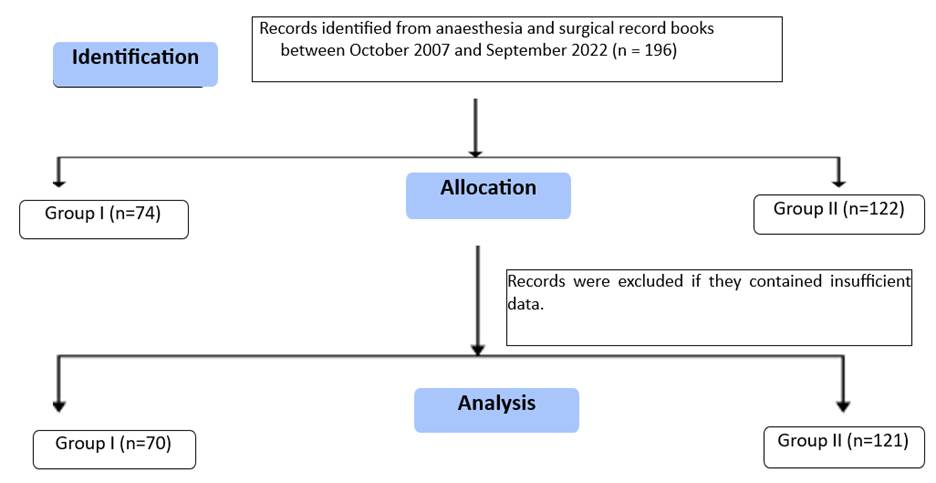
Materials and Methods: A total of 100 patients were randomized into two groups. One group was anesthetized using propofol and ketamine and other group received inhaled sevoflurane (Sevo) as sole anesthetic. Variables were recorded and outcome was compared.
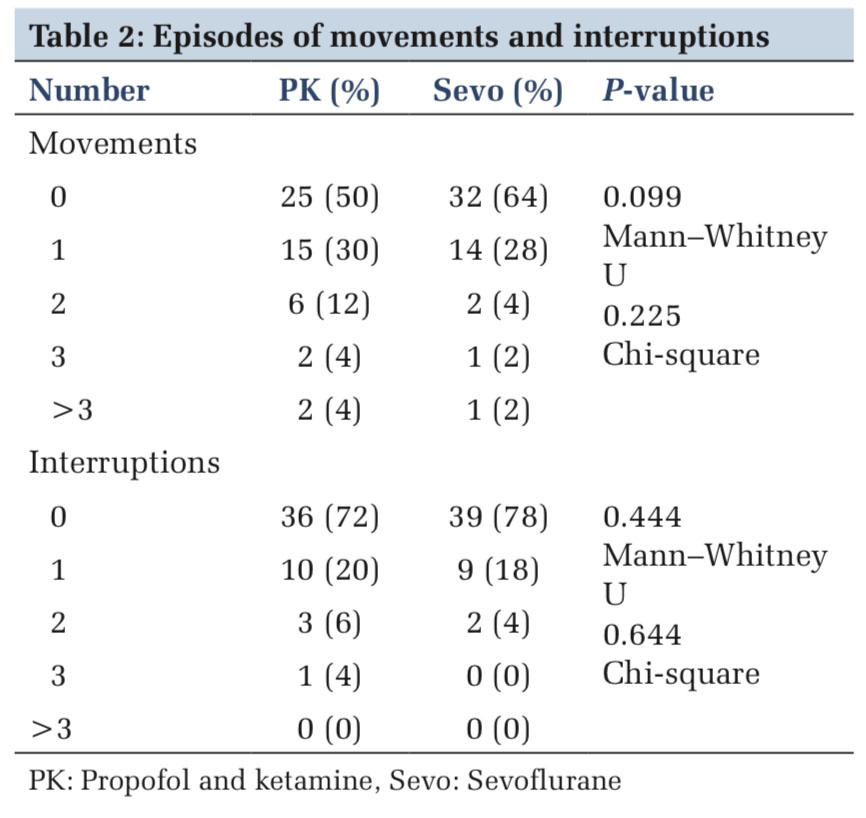
Results:Sevo provided faster onset and offset times (P < 0.01), albeit with higher incidence of emergence delirium (P < 0.01) for all other variables both the groups were comparable.
Conclusion: Both the groups provided essentially stable and safe anesthetic option for cardiac catheterization for pediatric patients. Sevo provided for faster induction and recovery as compared to IV anesthetics used in the study, but the recovery was complicated in the Sevo group by emergence delirium more frequently. This study failed to record any statistically significant hemodynamic variation between the two groups.
KEY WORDS:Cardiac catheterization, congenital heart disease, ketamine, laryngeal mask airway, pediatric, propofol, sevoflurane..
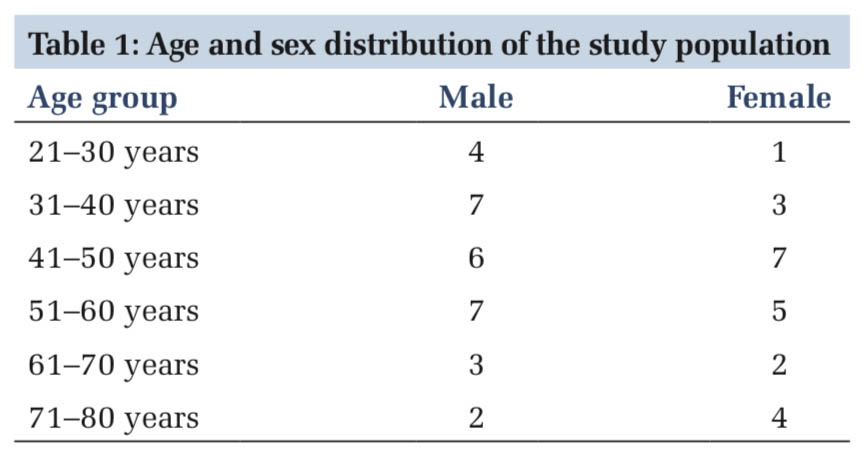
IntroductionSedation techniques for pediatric cardiac catheterizations were described in anesthesia literature as early as 1950s. Agents which caught early attention being pethidine, promethazine, and chlorpromazine, usually administered intramuscular.[1] With advances in field of echocardiography, the scope and practice of pediatric cardiac catheterization shifted from diagnosis of anatomical defects to that of classifying physiological severity and interventional procedures, currently, a wide variety of these procedures are carried out in cardiac catheterization laboratory (CCL).[2] Materials and MethodsStudy population selected were pediatric patients between the ages of 2 and 8 years who presented for procedure in CCL. A prospective, open labeled, and randomized comparative study was planned. Patients who did not provide consent, ASA grade more than III, known drug allergies to any of the drugs used in study, and patients who require drugs other than those in the study were excluded from the study. Sample size calculation was done for continuous variable (time, PAED scores, etc.), alpha error was set at 0.05 and power at 80%, the numbers required in each group were 46 and 47, it was decided to recruit 100 patients with 50 in each group, randomized using sealed envelopes. RESULTSDuring the study period, a total of 50 patients in each group were provided anesthesia for cardiac catheterization using LMA. No significant difference, between the two groups, was observed when demographic data was compared (Table 1). DiscussionGeneral anesthesia for pediatric patients undergoing cardiac catheterization had been described in 1965, before which patients were kept lightly sedated usually using a mixture of drugs given through intramuscular route.[5] Episodes of respiratory depression were recorded, also noted were increase in pulmonary vascular resistance, decrease in systemic vascular resistance thus increase in any right to left shunt.[1,6] It was acknowledged that general anesthesia would interfere with hemodynamics, so would controlled ventilation along with the partial pressures of blood gases, in effect this would lead to interference in results of the procedure for which the patient has presented.[5] Both ketamine and propofol have been used as sole agent, and each has its unique hemodynamic and anesthetic properties.[7-13] In this study, we have used subanesthetic doses of both to provide anesthesia with the aim to utilize the beneficial properties of both and reduce the incidence of undesirable effects of both the drugs.
|
ConclusionFrom our study, we can conclude that laryngeal mask anesthesia using the anesthetic agents used in this study can provide desirable anesthetic conditions in a safe manner. Sevo provides for efficient anesthesia management in a safe manner, special consideration for emergence will be required though. However, our particular study provides very limited information with regard to the ability of these agents to maintain stable or near baseline hemodynamics. What we gained mainly by the data and experience is that anesthesia using LMA and anesthetics at these doses can be safely administered for almost all varieties of congenital cardiac pathology patients presenting to CCL. Every definitive work of research requires some pilot program, this study can be considered as pilot for subsequent better designed, probably a cross-over study recording invasive pressures in real time, to provide for definitive and stronger evidence on hemodynamics, which were the secondary outcomes of this study. |
Subscribe now for latest articles and news.