Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i02.003
Year: 2015, Volume: 1, Issue: 2, Pages: 14-18
Original Article
D Namitha1, Aliya Nusrath2, A Rajeshwari3, N Asha Rani4
1Post-graduate, Department of Biochemistry, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya,Karnataka, India,
2Professor and Head, Department of Biochemistry, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India,
3Associate Professor, Department of Biochemistry, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India,
4Assistant Professor, Department of Biochemistry, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Mandya, Karnataka, India
Address for correspondence:
Aliya Nusrath, Professor and Head, Department of Biochemistry, Adichunchanagiri Institute of Medical Sciences, BG Nagara,
Mandya, Karnataka, India. Phone: +91-9448168236, E-mail: [email protected]
Background and Objectives: Diabetes, a lifelong progressive disease, with metabolic dysregulation, is associated with increased risk of cardiovascular complications. Paraoxonase (PON), an enzyme associated with high-density lipoprotein (HDL) is known to modulate the antioxidant and anti-inflammatory role of HDL and may have a protective role in the prevention of these complications. The present study was undertaken to evaluate serum PON, thiobarbituric acid reacting substances (TBARS) and serum lipid profile in Type 2 diabetes mellitus (DM).
Materials and Methods: The study group consisted of 60 cases of clinically diagnosed Type 2 DM and 60 age and sex-matched controls. Lipid profile was estimated by enzymatic methods using EM-200 auto- analyzer, TBARS by thiobarbituric acid assay and serum PON by spectrophotometric method.
Results: Type 2 DM patients showed significant increase in total cholesterol (P < 0.05), triacylglycerol (P < 0.0001), very low density lipoproteins (P < 0.0001), TBARS (P < 0.0001) levels, and significant decrease in HDL (P < 0.05) compared to controls. A significant decrease was observed in both basal (P < 0.0001) and salt stimulated PON activity in cases (P < 0.0001). Salt stimulated PON activity showed a positive correlation with HDL levels (P < 0.05) in cases, whereas basal PON activity showed negative correlation with TBARS in controls (P < 0.005).
Conclusion: Type 2 DM patients have significantly lower levels of PON activity along with dyslipidemia with a direct correlation of PON with HDL levels. This may reduce the protective role of HDL and increases the susceptibility of cardiovascular complications.
KEY WORDS:Dyslipidemia, thiobarbituric acid reacting substances, paraoxonase, Type 2 diabetes mellitus
Diabetes mellitus (DM), a chronic progressive metabolic disorder, occurring due to body’s inability to secrete or use insulin to its full potential is characterized by hyperglycemia. The sustained hyperglycemia attacks both microvessels and macro vessels in the body.[1]
Type 2 DM is a disease of metabolic dysregulation, involving derangements in glucose and lipid metabolism resulting in accumulation of altered lipid species in the circulation and in the tissues, and alteration in metabolic signaling pathways that regulate insulin secretion from the pancreatic beta- cells.[2]
Paraoxonase (PON) (EC 3.1.8.1), a human serum arylesterase is a polymorphic enzyme consisting of PON1, PON2, and PON3 that catalyzes the hydrolysis of organophosphates such as paraoxon and aromatic carboxylic acid esters of fatty acid. It is a glycoprotein containing 337 amino acid residues with a molecular weight of approximately 43kDa and a serum concentration of about 50 mg/L.[3] It is produced by the liver and is associated with high-density lipoprotein (HDL) particles and is known to modulate the antioxidant and anti-inflammatory role of HDL.[4,5]
It hydrolyzes proinflammatory oxidized lipids, which are present in oxidized low-density lipoprotein and ruins their atherogenic characteristics, and it also decreases the accumulation of lipid peroxidation products.[3,5] The enzyme plays a role in decreasing oxidative stress. PON1 is an important endogenous free radical scavenging system in the human body.[5]
Homocysteine thiolactone hydrolase, a calciumdependent protein of 45kDa is a component of HDL and is identical with serum PON.[6] Homocysteine thiolactones, a metabolite of homocysteine causes endothelial dysfunction and vascular damage. PON1 plays a vital role in cardioprotection, as it is required for detoxification of homocysteine thiolactone.[3] Study by Suvarna et al. reported that Type 2 DM patients with complications have significantly decreased HDL-C and PON1 activity, leading to decreased functioning of HDL-C in these patients.[2] Study done by Ferretti et al. reported significantly lower PON1 activity in Type 1 DM.[4] Another study by Abbott et al. reported that PON activity was lower in both Type 1 and Type 2 diabetes patients.[7] However, Beer et al. found no significant difference in PON 1 activity and concentration in the diabetic group when compared to impaired fasting glucose and control although postprandial hyperlipidemia was associated with changes in serum PON1 in diabetic subjects.[8] Reduced PON activity increases the oxidative stress in the patients. Hence, the present study was undertaken to evaluate serum PON levels and serum lipid profile in Type 2 DM. Monitoring the trends in cardiovascular complications via PON 1 is of critical importance in managing patients with Type 2 DM
Materials and Methods Clinically diagnosed 60 DM cases attending Medicine outpatient department at Adichunchanagiri Hospital and Research Centre, B G Nagar, Mandya were included in the study. Age and sex matched 60 healthy individuals were taken as a control group. Informed consent was taken and the study was approved by the ethical committee of the institution. Patients suffering from acute and chronic inflammatory conditions, other metabolic conditions like ketoacidosis, cerebrovascular accidents, preeclamptic patients, pre-existing chronic kidney disease, chronic renal failure, nephrotic syndrome, and primary hypertensives were excluded from the study. 5 ml of fasting blood sample was drawn from all subjects under the aseptic precaution and 2 ml of blood was drawn in postprandial period. Fasting samples were analyzed for routine blood parameters, fasting plasma glucose (FPG), serum lipid profile, TBARS levels, and PON levels. Postprandial sample was analyzed for postprandial plasma glucose (PPPG). Plasma Glucose was measured by glucose oxidase - peroxidase method (Trinder’s method), serum total cholesterol (TC) by CHOD-PAP method, HDL by modified polyvinyl sulfonic acid and polyethylene glycol methyl ether coupled classic precipitation method and triacylglycerol (TG) by glycerol phosphate oxidase Trinder method using standard kits from ERBA diagnostics on EM-200 auto-analyzer. Very low-density lipoprotein (VLDL) was calculated by dividing TG with five (TG/5). LDL level were calculated using Friedwald’s formula, LDL= TC - (HDL+TG/5). Serum PON was measured by spectrophotometric method using p-nitrophenyl acetate as a substrate, in which PON catalyzes the cleavage of p-nitrophenyl acetate resulting in the formation of phenol. The rate of formation of phenol is measured by monitoring the increase in the absorbance at 412 nm.[9,10] Serum TBARS, a marker of lipid peroxidation and hence oxidative stress was measured by thiobarbituric acid method.[11]
Statistical analysis Results are represented as mean ± standard deviation. Statistical analysis was done using Student’s t-test, and statistical significance was compared between the cases and the controls. Pearson correlation between the study variables was performed to establish the relationship. Probability value (P) of < 0.05 was considered as statistically significant. Statistical analysis was done using the Statistical Software: SPSS-16.
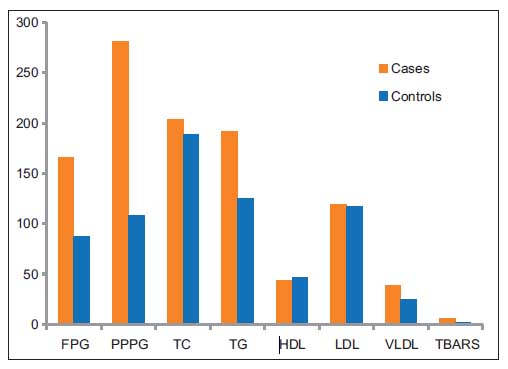
ResultsType 2 DM patients showed significant increase in FPG (P < 0.0001), PPPG (P < 0.0001), TC (P < 0.05), TG (P < 0.0001), VLDL (P < 0.0001), TBARS (P < 0.0001) levels, and significant decrease in HDL (P < 0.05) compared to controls as shown in Table 1 and Figure 1.
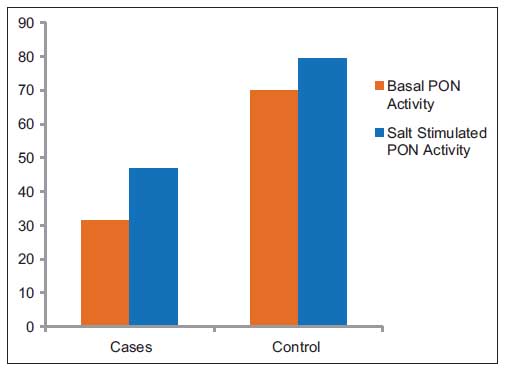
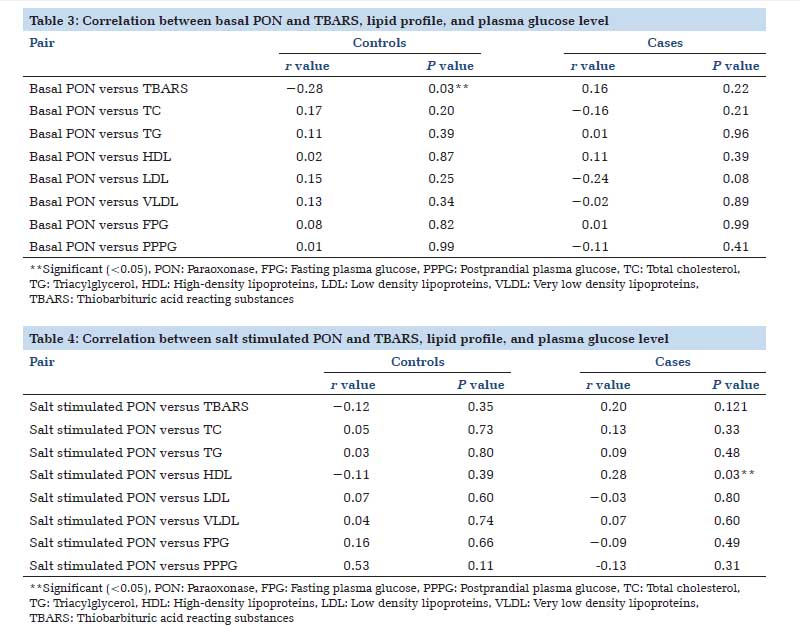
Significant decrease was observed in both basals (P < 0.0001) and salt stimulated (P < 0.0001) PON activity in cases compared to controls as shown in Table 2 and Figure 2. The salt stimulated PON activity showed a positive correlation with HDL levels (P < 0.05) in cases as shown in Table 4, whereas basal PON activity showed negative correlation with TBARS in controls (P < 0.005) as shown in Table 3. Basal PON showed a negative correlation for PPPG as shown in Table 3 and salt stimulated PON shows a negative correlation for both FPG and PPPG as shown in Table 4, but these correlations are not statistically significant. |
||||
   |
||||
|
||||
DiscussionDM is a global pandemic affecting almost all the systems in our body due to insulin deficiency or impaired insulin utilization. Hyperglycemia generates free radicals, increasing oxidative stress, which is proven to be one of the mechanisms for the development of complications in DM.[12] The high plasma levels of lipid peroxidation products in diabetic patients are attributed to higher susceptibility of lipoproteins for oxidation. In the present study, the diabetic patient showed significantly higher levels of oxidative marker TBARS (P < 0.0001). PON is an enzyme located in a subfraction of HDL containing ApoA1 and clusterin Apo J and it is anchored to HDL by its hydrophobic N-terminal end and also bound to ApoA1.[7] It contributes to most of the anti-atherogenic activity of the HDL molecule. This enzyme has both PON and arylesterase activity and by virtue of its hydrolytic action, prevents accumulation of lipid peroxides in LDL, and gives protection against lipoprotein oxidation.[13] Kota et al., have reviewed many studies reporting low PON activity in DM contributing to greater risk of atherosclerosis and cardiovascular disease.[13] However, some of these studies reported no difference in PON activity between diabetics and non-diabetics. In the present study, there was a significant decrease in both basal PON (P < 0.0001) and salt stimulated PON activity (P < 0.0001), this is in accordance with many other studies.[7,12,14] A study by Gowda et al. [15] showed a significant decrease in PON activity in Type 2 DM patients with nephropathy but not in Type 2 DM patients without any complications. They concluded that normal PON levels were protecting these diabetic patients from diabetic complications. Other studies also have found a significant decrease in PON activity in Type 2 diabetic patients with microvascular complications when compared to patients with no complications.[7,16] The cause of lower PON activity in DM is not clear, it may be due to loss of interaction between the protein and HDL molecule resulting from increased glycation and glycoxidation of PON as well as presence of circulatory inhibitors.[7] The decrease in PON activity may decrease the antiatherogenic effect of HDL leading to accelerated atherosclerosis and CAD in diabetic patients, who have additional proatherogenic dyslipidemias. Type 2 DM is associated with dyslipidemias. Due to deficiency and/insulin resistance, there is ineffective lipoprotein lipase activity, increased lipolysis, and increased hepatic VLDL secretion resulting in hyperlipidemias. The present study group showed significant increase in TG (P < 0.0001), VLDL (P < 0.0001), TC (P < 0.05), and decrease in HDL (P < 0.05). Singh et al. [17] found a significant negative correlation between PON activity and TC, LDL-C. However Abbott et al. [7] reported no association between PON and most of the lipids in DM, but found correlation between PON and HDL and Apo A in controls. In the present study, a positive correlation is found between HDL and salt stimulated PON activity in diabetics (P < 0.05), indicating decreased HDL level further decreases PON activity. This is in accordance with a study by Suvarna et al.[2] A negative correlation was found in controls between basal PON and TBARS activity (P < 0.05) showing increasing in oxidative stress with low PON activity. However, there was no correlation in diabetics; this could be due to low sample size. Blood glucose level also showed negative correlation with PON activity particularly PPPG (PPPG vs. basal PON [P > 0.05], FPG vs. salt stimulated PON [P > 0.05] and PPPG vs. salt stimulated PON [P > 0.05]), which was not significant. Hyperglycemia has an effect on PON and ApoA1 function due to a non-enzymatic glycation. There is evidence that PON activity is affected by meals, but this modulation was attributed to fat content.[18] However, in vitro experiments of incubating glucose with HDL and PON showed decrement in HDL PON activity by 50%.[4] Glycoxidation and lipoxidation may cause a conformational change in both HDL and enzyme PON resulting in decreased PON activity.[18] Both micro and macrovascular complications of diabetes mellitus are majorly due to LDL peroxidation. HDL along with PON activity reduces the formation of oxidized LDL. Hence, lower HDL levels and reduced PON activity will increase the risk for development of complications in DM. To conclude, the present study showed a significant lower PON activity in Type 2 DM and a positive correlation with HDL. Causes for the development of diabetic complications are multifactorial and increased oxidative stress precipitated by reduced PON activity adds to the pathogenesis of diabetic complications. The limitation of the present study is low sample size and there in no grouping of diabetics based on the presence or absence of complications. Furthermore, effects of duration of disease and treatment effects on study parameters are not evaluated. A larger sample sized prospective study should be undertaken to demonstrate the progress of complications of DM with low PON activity. |
Subscribe now for latest articles and news.