Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i02.009
Year: 2016, Volume: 2, Issue: 2, Pages: 44-47
Case Report
Ashwini Bakde1, Amit Disawal2, Kishor Taori3, Aarti Aanand4, Prajwalit Gaur5, Manish Agrawal5
1Assistant Professor, Department of Radiodiagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India,
2Associate Professor, Department of Radiodiagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India,
3Professor and Head, Department of Radiodiagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India,
4Professor, Department of Radiodiagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India,
5Resident, Department of Radiodiagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India
Address for correspondence: Dr. Ashwini Bakde, Flat No. 303, Plot No. 150/A, Prajakta Orchid Apartment, Pande Layout, Khamla, Nagpur - 440 025, Maharashtra, India. Phone: +91-9822909771. E-mail: [email protected]
Lymphatic filariasis is an endemic infection seen predominantly in the tropical and subtropical regions, and approximately 120 million people are infected and 1.1 billion are at risk of infection all over the globe. It presents with lymphatic dysfunction in various forms such as elephantiasis, lymphocele, hydrocele, chyluria, and groin lymphadenovarix. The patient may complain about symptoms of fever, redness and pitting edema, etc. We report a rare presentation of filariasis in an unusual and uncommon location, presenting as an intra-abdominal mass.
KEY WORDS:Retroperitoneal cyst, filariasis, para-aortic hypodensity.
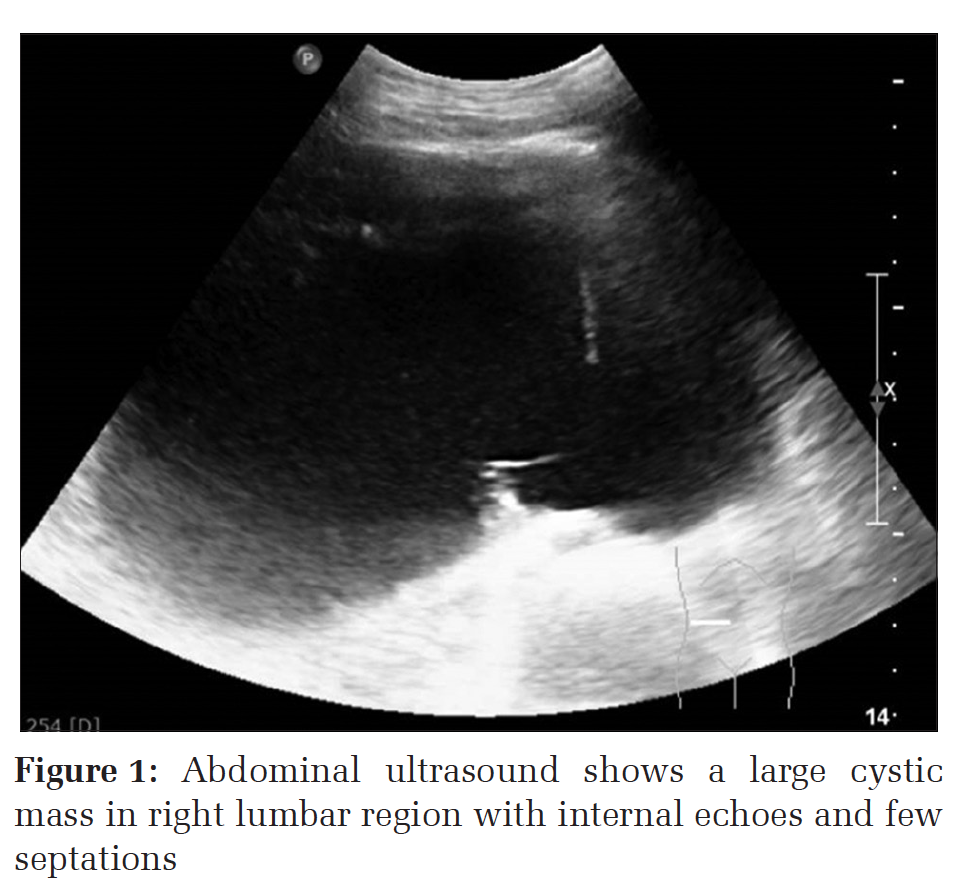
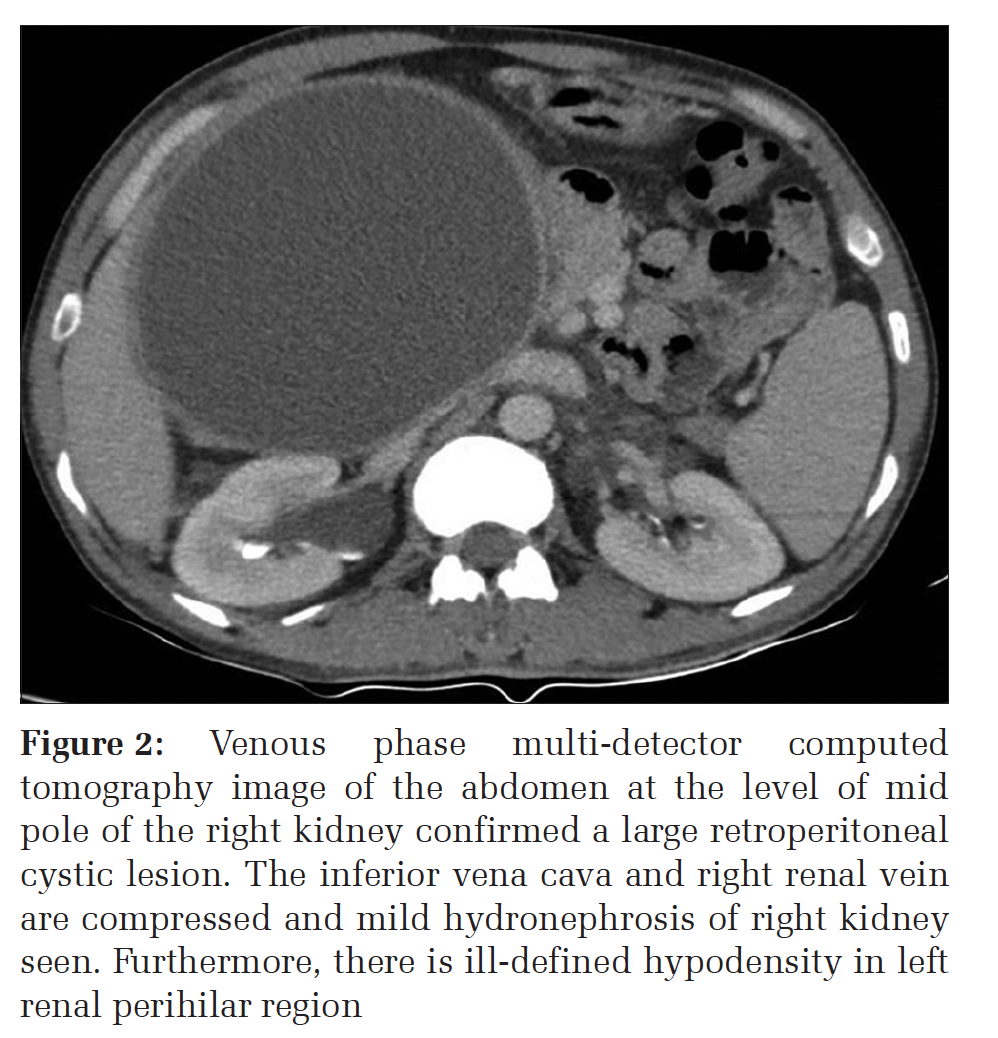
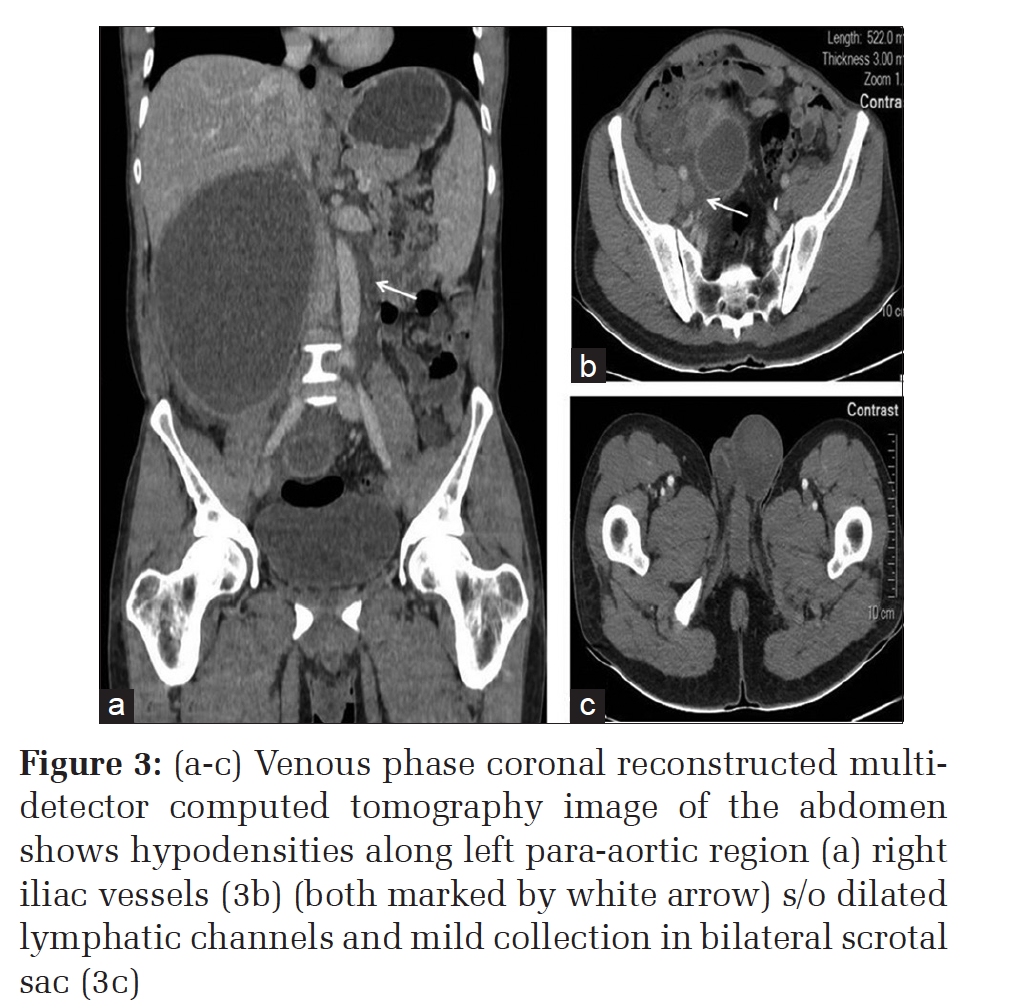
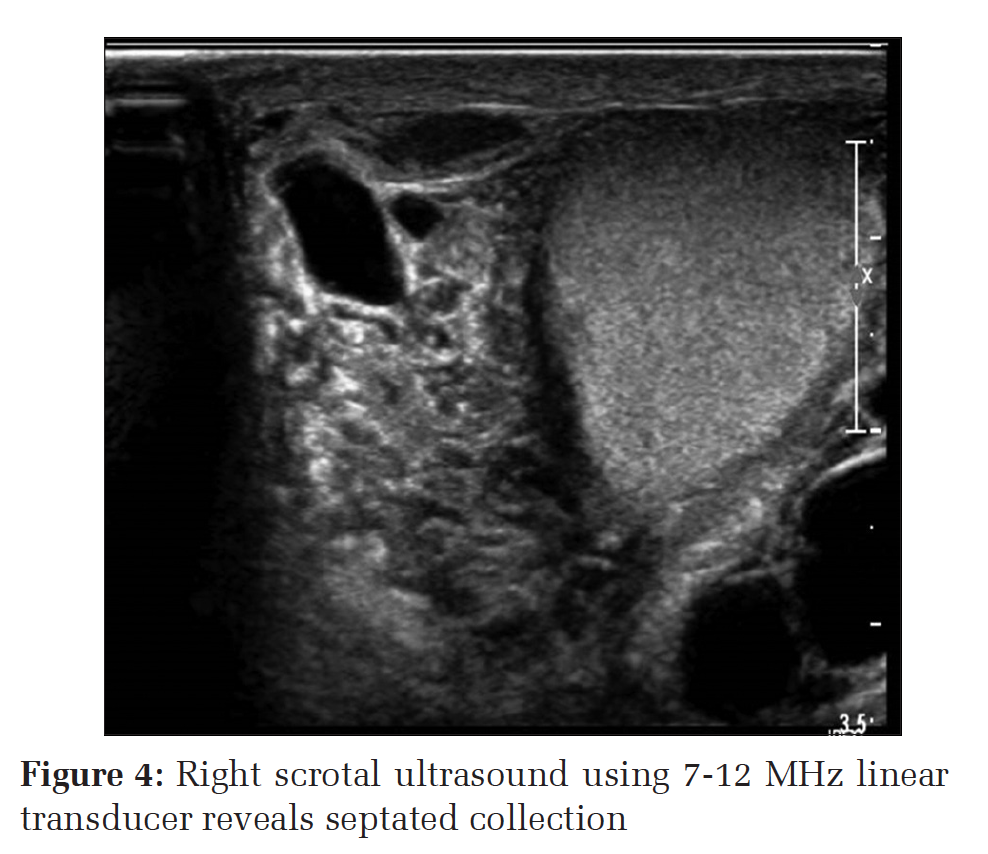
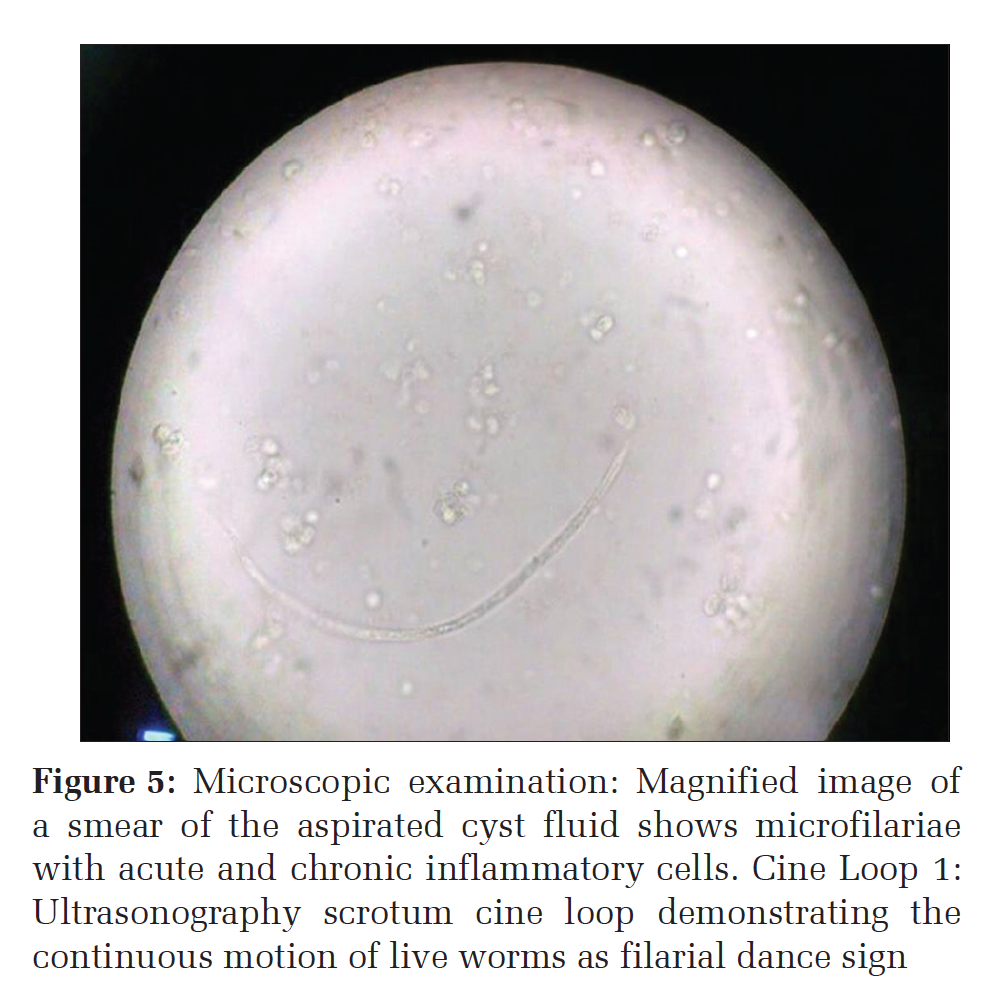
IntroductionLymphatic filariasis is a parasitic infection commonly known as elephantiasis. Filariasis presents as hydrocele, genital/scrotal swelling, adenolymphangitis (ADL), swelling of limbs, and genitalia. The causative agent resides in lymphatic channels and causes its obstructions leading to lymphedema.[1] In India, males commonly present with hydrocele and females with lymphedema.[2] Filariasis presenting as the primary retroperitoneal cyst is very rare even in endemic areas like India. Wuchereria bancrofti is the common causative agent of filarial infections in India.[3] Here, we present a rare case of filariasis presenting as a primary retroperitoneal cyst. The imaging findings are discussed in the case report, which leads us to the diagnosis with further confirmation on microscopy by the presence of microfilariae within the cyst. Only a few such cases have been reported in the literature.[3,4] Case ReportA 38-year-old male patient, from the urban area of Maharashtra state (India), was referred for radiological evaluation of a gradually enlarging mass in the abdomen extending from the right hypochondriac to the pelvic region for last 2 months. He also had an occasional low-grade fever. He was chronic alcoholic since last 10 years with intermittent episodes of acute pain in the abdomen. The patient belonged to low socioeconomic status. On clinical evaluation, surgeons suspected a diagnosis of chronic pancreatitis with pseudocyst formation and advised ultrasonography (USG) of abdomen-pelvis for further evaluation. Serum lipase was done which was marginally raised (215 U/L). USG performed on (Philips iU22 xMATRIX) revealed a cystic lesion measuring approximately 21 cm × 10 cm and extending between the levels of head of the pancreas to the pelvis craniocaudally. It showed few septations in the lower part and internal echoes within Figure 1. Head of the pancreas showed normal echogenicity. The patient underwent contrast-enhanced computed tomography (CT) scan to know the extent of the lesion and for further characterization. Three phase abdominal scan with 3 mm thick slices was performed on a multi-detector row CT scanner (Brilliance ICT 256, Philips Medical Systems, Best, The Netherlands) with multiplanar reconstruction. The thin-walled cystic lesion of average attenuation 17 HU was noted on the right side of the abdomen. There were few septations in the lower part with no obvious solid component or calcifications within. It was displacing duodenum and pancreas medially with maintained fat planes suggestive of the retroperitoneal location of the lesion. The pancreas was normal in size shape and attenuation. Posteriorly, the lesion was compressing over IVC, right renal vein, and right ureter with resultant mild hydronephrosis (Figure 2). Reviewing at the scan carefully, we found small collection in the bilateral scrotal sac and relatively well-defined hypodensities extending in retroperitoneum along pre-para aortic and right iliac vessels, which suggested bilateral mild hydrocele with possible dilated lymphatic channels (Figure 3a-c). Hence, we could rule out the diagnosis of pancreatic pseudocyst. The linear retroperitoneal hypodensities pointed the cyst to be of lymphatic origin with dilated lymphatic channels. Further, USG scrotum and Doppler revealed mild collection with multiple septations and moving internal echoes (Figure 4) in both scrotal sacs suggestive of classical filarial dance sign (Cine Loop 1) with associated thickened spermatic cord which made us think about the diagnosis of retroperitoneal cystic lymphangioma of filarial origin. However, clinically there was no scrotal swelling. A fine-needle aspiration cytology (FNAC) was performed under ultrasound guidance. Chocolatecolored fluid was aspirated, which revealed live microfilariae. Microscopic examination further confirmed our diagnosis (Figure 5). The patient was put on diethylcarbamazine therapy, 100 mg t.i.d for 3 weeks. As the cystic lesion was large enough causing abdominal discomfort, surgical intervention was considered, and the patient underwent laparotomy. On surgery, a well-defined retroperitoneal cyst was removed after careful dissection to release adhesions. Histopathology revealed the presence of microfilariae in the cyst. The post-operative period was uneventful, and the patient was discharged after 1 week. DiscussionFilariasis is a vector-borne disease. Lymphatic filariasis is caused by nematode filariae commonly seen in tropical and subtropical regions of the world. Both sexes are equally affected. W. bancrofti, Brugia malayi, or Brugia timori infect the lymphatic system of humans which are the definite host and mosquito being an intermediate host. Following filarial infection, there generates an inflammatory immune response that results in lymphatic obstruction.[1] In the clinical course, the patient may present as asymptomatic microfilaremia, acute phases of ADL or chronic, irreversible lymphedema.[5] Patients most commonly present with fever, lymphedema, hydrocele, scrotal/vulval, and lower limb swelling. It can also cause tropical eosinophilia in rare conditions. We report an unusual presentation of filariasis as a retroperitoneal cystic lesion with confirmation of diagnosis by the demonstration of live microfilariae in the cyst fluid. Clinical examination and imaging both play an important role in localization and accurate diagnosis of the condition. As in our case, ultrasound and CT scan were very helpful in narrowing the differential diagnosis. The various differential diagnoses in case of the retroperitoneal cystic lesion could be pancreatic pseudocyst, non-pancreatic pseudocyst, lymphangioma, urinoma, pancreatic cystic tumor (cystadenocarcinoma), pseudomyxoma peritonei, and parasitic cyst. In this patient, after confirming the retroperitoneal location of the cyst on CT scan with normal appearing pancreas, the possibility of pancreatic pseudocyst was excluded, and the dilated lymphatic channels with filarial dance sign on USG scrotum examination, the diagnosis of lymphatic origin of the cyst was suspected. Diagnosis of filariasis is confirmed by demonstration of microfilariae in blood, urine in case of chyluria or hydrocele fluid. On ultrasound, the presence of live worms is seen to be in continuous motion, i.e. the filarial dance sign, which is diagnostic of lymphatic filariasis.[6] In our case, there was no associated scrotal swelling, but the dilated lymphatic channels and filarial dance sign suggested the possibility of a cyst of filarial origin, with presence of sheathed microfilariae on FNAC and microscopy further confirming the diagnosis. Filariasis presenting as a retroperitoneal cyst is a rare location with reported incidence of 1 in 1,05,000 hospitalized patients.[7] The exact etiopathogenesis of the development of primary filarial retroperitoneal cyst is not known. However, the dilatation of retroperitoneal lymphatic channels due to obstruction and their rupture may be one of the reasons for its development. To the best of our knowledge, only a few case reports have been reported in the literature.[8-11] In lymphatic filariasis, diethylcarbamazine is the drug of choice. Other drugs used are antihistamines, steroids (to soften the edema and reduce the swelling), and intravenous antibiotics for superadded infections.[12] Surgical resections are required when the lesions are large, and patients are symptomatic, as in our case.[11]
|
ConclusionA case of filariasis presenting as the retroperitoneal cyst is unusual. It is difficult to comment on the origin of the retroperitoneal cyst on CT scan, but whenever there is an ill-defined non-enhancing hypodensity extending along the para-aortic region in retroperitoneum, one should suspect of the dilated lymphatic channels which will be helpful in diagnosis and appropriate management. |
Subscribe now for latest articles and news.