Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.002
Year: 2021, Volume: 7, Issue: 3, Pages: 6-12
Review Article
Naveen Narayan1 , Ravi Hullamballi Shivaiah2 , Vikram Ramamurthy3 , Prema Dhanraj4
1Associate Professor, Department of Plastic & Reconstructive Surgery, Adichunchanagiri Institute of Medical Sciences, B G Nagara, Mandya, Karnataka, India,
2Associate Professor, Department of Plastic & Reconstructive Surgery, JSS Academy of Higher Education & Research, Mysuru, Karnataka, India,
3Assistant Professor, Department of General Surgery, Sri Siddhartha Institute Of Medical Sciences, Bengaluru Rural, Karnataka, India,
4Professor and Head, Department of Plastic & Reconstructive Surgery, Raja Rajeswari Medical College & Hospital, Bengaluru, Karnataka, India
Address for correspondence:
Vikram Ramamurthy, Assistant Professor, Department of General Surgery, Sri Siddhartha Institute Of Medical Sciences, Bengaluru Rural, Karnataka, India. E-mail: [email protected]
Context: Nipple areola complex (NAC) is an essential part of breast reconstruction. It functions as an imperative aesthetic unit for the breast. Numerous surgical techniques to the gamut of NAC reconstruction such as skate flap, star flap, Swiss Roll flap, C-V flap, silicone rods, spiral flap made of residual scar tissue and tissue engineering and many others have been added. Despite the availability of surfeit of techniques, a simple reliable method to maintain nipple projection remains obscure. The purpose of this study was to demonstrate the advantages of Skate flap and tattooing in NAC reconstruction. Methods and Material: The NAC reconstruction Skate flap technique involved marking of the flap design on the patient’s breast in afore tattooed scar tissue. Dermal flaps were raised with subcutaneous pedicle and closed with inverted dermal absorbable sutures followed by simple interrupted non-absorbable sutures. After this, full thickness skin graft was used to cover the adjacent donor defect to recreate the areola. The newly constructed nipple was guarded using a syringe barrel. This was done to avert compression on the anew nipple. This was left in place for up to 6 weeks. Surgical outcome was evaluated by recording post-operative complications, nipple projection at intervals and surgical revisions, if needed. Callipers were used to record projection of the nipple at the time of surgery and at 1, 3 and 6 months post-operatively. Results: A total of 26 NAC reconstructions in 19 post burn breast patients were performed over duration of 18 months employing Skate flap and tattooing. Mean nipple projection at time of surgery was 6.77 mm and 4.66 mm at end of 6 months follow up. There was a mean net projection loss of 31% at the end of 6 months post-operatively. Overall patient satisfaction on the outcome of reconstruction was generally favourable. No post-operative complications were noted. Conclusion: The study shows that the use of a Skate flap is a safe, easily performed, reliable and reproducible technique for maintaining projection in reconstructed nipples for a long period. Using the burnt scarred tissue helps in achieving excellent projection since contracture is somewhat lessened and also a more aesthetically pleasing nipple reconstruction is achieved matching the surrounding topography.
Keywords: Post Burned breast, NAC reconstruction, Nipple areola reconstruction, Skate flap
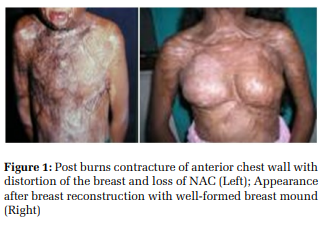
Burn injuries to the breast with involvement of the nipple areola complex (NAC) in females can be confounding. Scarring and contracture of the NAC frequently has severe psychological impact on the patient. In female children with burns on the chest, future breast development is an important issue. Involvement of the NAC always leads to questions related to breast development in the child. Thus management of the burn injury during the acute phase of treatment is of paramount importance. The need for identifying and preservation of the breast buds during debridement in acute phase of burns is thus very crucial for later breast development. Majority of patients with burns to breast involving NAC will require surgical intervention to support breast development. In an adult female patient, such injury which can be severe in nature can lead to severe distortion of the involved breasts. (Figure 1)
Nipple presence on a post burn reconstructed breast is psychosocially pleasing for women especially in young adults and boosts their morale.[1] Nipple is an essential and defining anatomic marker and plays an important role in breast aesthetic unit.[2] Reconstruction of the burned breast can be addressed in two parts - Reconstruction of the breast mound and reconstruction of the NAC. Choosing the best option available is dependent upon the age at which the patient sustained injury, extent of surgical management during the acute phase and age at which patient presents to the reconstructive surgeon. An obvious restriction in the breast development as a result of scar contracture is the indication for surgical intervention. However the timing of such intervention varies with each patient.
In patients with anterior chest wall burns, the goal is to allow breast development to proceed in an unimpeded fashion. NAC reconstruction forms the vital final component in functional and aesthetic restoration of the female breast following burns injury.[3] NAC reconstruction is usually belated until the recreated breast mound matures of the scars and breasts are fully developed. NAC reconstruction should be done only after acceptable symmetry and shape of the reconstructed breast has been obtained. The reconstructed breast may have complications such as NAC malposition, retracted nipple and partial or total absence of the NAC. Z plasty may be used to correct malposition to match the NAC on contralateral unburned breast, if available.
However a total loss of NAC, presents a difficult problem in the anterior chest wall burned patients. Even though several techniques are available to address this, no single method is found to give reliable and consistent outcome. Different techniques include intradermal tattooing, variations of ‘pullout’ local tissue flaps such as tripod / quadripod flaps / Skate flaps, skin grafts (inner thigh, buttock crease), cartilage grafts, nipple sharing and tissue engineered materials. Skate flap was described by Little in 1984 for NAC reconstruction. However skate flap was less considered in reconstruction of NAC in burn patients. Skate flap found revived use after McCauley and Robson accounted its successful use in reconstruction of the nipple in the burned breast. They re-established the notion of a sufficient subdermal plexus in burned patients even after being resurfaced previously with skin grafts.
Fundamentally the projected nipple recreated, with all the described nipple reconstruction techniques, will succumb to some degree of flattening in the postoperative period due to volume loss.[4] Factors such as lack of durable support, skin surface tension and centrifugal forces have been quoted to explain this eventuality. Patient satisfaction in burned breast reconstruction highly correlates with the degree of near normal correction of the NAC. This study intends to study the benefits of Skate flap (and tattooing) in NAC reconstruction in terms of providing long-lasting, satisfactory reconstruction with minimal morbidity.
This prospective study was conducted at our institution on patients with burned breast who were intended to undergo tattooing and Skate flap nipple reconstruction between October 2018 and March 2021. Only those patients agreeing for a minimal follow-up period of 6 months after the procedure were included in the study and those who failed to comply were excluded. Also patients below 18 years and above 60 were not included in the study.
Institutional ethical committee clearance was taken for the study. Written informed consent was obtained from each patient prior to their inclusion in the study. Patient demographic data was collected as needed.
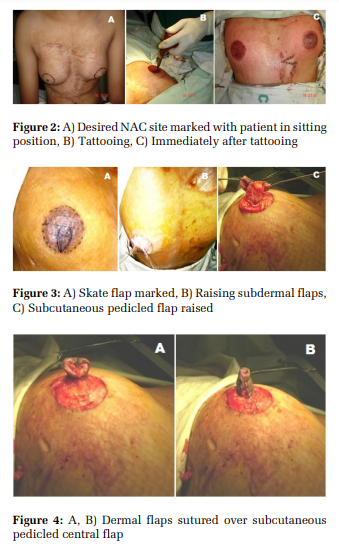
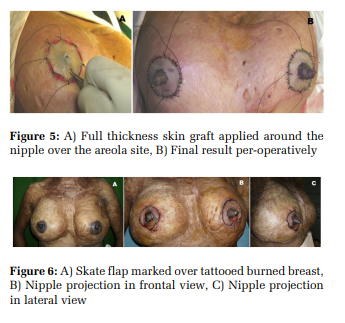
Nipple areolar tattooing as a part of NAC reconstruction was done at least after 3 months of breast reconstruction (Figure 1). 3 months thereafter Skate flap was performed. Surgical outcome evaluations included post-operative complications, nipple projection measurements using callipers and need for surgical revision. Follow up was performed at 1, 3 and 6 months postoperatively to record the size, projection and symmetry of the reconstructed NAC. The patients also assessed the results, and were asked to grade indices of overall satisfaction as bad (0), satisfactory (1), good (2) or excellent (3) at the end of 6 months post-operatively.
Technique - Pre-operatively nipple position was determined with the patient in a relaxed sitting position and tattooed (Figure 2). Skate flap pattern was marked onto the tattooed area of the breast mound. Nipple cylinder of 7-8 mm in diameter and 1-1.2cm length for an over projection of the future nipple was planned. If unaffected contralateral nipple were to be present, nipple over projection of at least 30% and maximum of 50% (arbitrary) compared to the unaffected nipple was planned accounting the subsequent flattening. In bilateral NAC reconstruction, the overall size of the reconstructed breast and patient’s desired final appearance were taken into account along with future shrinkage while planning and marking of the pattern. Dermal flaps and subcutaneous pedicle were raised (Figure 3). Heaved flaps were approximated using inverted dermal Vicryl 4-0 sutures and simple interrupted Nylon 5-0 sutures (Figure 4). For the areolar reconstruction, the adjacent donor site was covered using a full thickness skin graft (Figure 5). To prevent compressive forces pressuring on the newly constructed nipple, a syringe barrel was used for protection and left in situ for up to 6 weeks (Figure 6). Patient post-operatively was put on antibiotics and analgesics as per standard hospital protocol. Patients were followed up at regular intervals as per the proforma and relevant data collected.
Statistical Analysis
Qualitative data was summarized using percentage and quantitative data was summarized using mean.
A total of 26 skate flap reconstructions were performed in 19 post burned breast patients included in the study.
Patients’ age in the study averaged 31.3 years, with the youngest being 19 years old and oldest 47 years old. Out of the 19 patients included in our study, 7 patients underwent bilateral and 12 patients underwent unilateral NAC reconstruction. Out of the 12 unilateral cases, 7 were right sided and 5 were left sided NAC reconstruction.
All the cases were performed under local anesthesia. No patient had post-operative complications such as infection, oedema, seroma, hematoma, flap loss due to necrosis or any other untoward complications. During follow up new nipple areola was assessed in terms of projection, invagination, symmetry in relation to the opposite side and patient’s overall satisfaction.
Neo-nipple projection was measured in millimetres. Nipple projection immediately in the post-operative period ranged from 6 to 8 mm with a mean of 6.77 mm. At end of 1 month and 3 months post operatively nipple projection averaged 5.77 mm and 5.04 mm, respectively in the study group. The overall nipple projection at the end of 6 months follow up from the time of surgery varied with decrease in projection being 1mm in 1 patient, 2mm in 20 patients, 3mm in 5 patients. Nevertheless no patient in our study group needed surgical revision due to nipple projection loss. Average nipple projection at 6 months was 3 to 6 mm with an average of 4.62 mm. Overall patient satisfaction scoring by 19 patients at the end of 6 months was excellent by 2, good by 7, satisfactory by 8 and bad by 2. (Table 1)
Breast in women is not only of functional significance for breast feeding but also is a mark of womanhood. Thus the treating surgeon has to keep both functional restoration and aesthetic reconstruction in mind while treating post burns breast deformities. Aesthetically satisfying nipple reconstruction helps in betterment of the profile of the reconstructed burned breast and plays an important role in restoring patient’s psychosocial status.
Nipple projection has been difficult to achieve and more arduous to maintain. The ideal NAC reconstruction technique should maintain shape, texture, colour, nipple projection for long, and as in any reconstructive procedure have minimal donor site morbidity. None of the currently available techniques fulfil the said criteria satisfactorily. Hence the choice of method for NAC reconstruction is surgeon’s choice currently. No one procedure is superior over other as per very few comparative studies. There are differences in results, complications, and the ultimate yardstick – degree of loss of projection with time.
The intended goal of this study was to demonstrate the potential benefits of Skate flap using pre-tattooed local scar tissue. Survival is dependent on an adequate blood supply from the dermal-subdermal plexus. Though, patients with burn injury may have questionable blood supply at this level but, however, Skate flaps can be successfully designed in burned patients. Advantages of the skate flap include efficient use of local tissue, simple, safe, reliable, maintenance of projection due to use of already contracted scar tissue and contralateral normal nipple, if present, is not disturbed. Also surgery can be performed quickly and with minimal morbidity and can be performed as an office procedure. However no substantial long-term followup is documented. In case of substantial loss of nipple projection, revision of the nipple reconstruction can be done with use of dermal fat grafts or dermal fillers. Also acellular dermal matrix or collagen cylinder can be used at the time of nipple reconstruction or later to strengthen nipple projection. Secondary skin flap elevation may allow improved nipple projection and contour.
In our study group, average nipple projection at the time of surgery ranged from 6 to 8 mm and average projection range at the end of 6 months post operatively was 3 to 6 mm, with net projection loss ranging from 17% to 50%, averaging 31% loss. Thence, many authors advise nipple projection at the time of surgery to be twice the ultimately desired size taking into account eventual loss of projection due to volume loss.[5,6] Lee LQ Pu opine that NAC recreation in an implant-based reconstruction is challenging as there is not enough tissue over the breast implant which can be utilized for a nipple reconstruction with any available techniques currently. Even though commonly skate or a C-V flap is performed for nipple reconstruction long-term result from either has not been good.[7]
We acknowledge that the relative short follow-up time of 6 months in our study constrains us from commenting on long lasting aesthetic outcome and nipple projection, definitively.
Along with lack of long term nipple projection maintenance, colour mismatch, unattractive shape, size and texture and nipple malposition also have been ascribed to undesired effects of NAC reconstruction.[8]To sustain projection of the reconstructed nipples use of autologous, allogenic, and alloplastic materials have been mentioned in literature, with lower rates of projection loss in alloplastic grafts followed by autologous and allogenic.[9]Guaranteed best colour & texture match with contralateral side is provided by composite nipple grafts even at long-term follow-up and is also better choice in case of implant based breast reconstruction wherein the skin envelope is usually tight and thin as local flaps would be more prone to contraction because of tension.[10] Optionally other treatments to nipple cylinder reconstruction include cosmetic tattooing with differential texturing of the areola only, autologous or composite grafts such as contra lateral nipple / fat / cartilage grafting.[11,12] Also use of other biologic materials such as human dermis, collagen[13] , hyaluronic acid[14] , or polylactic acid.[15]
In our study, overall patients’ satisfaction with the aesthetic appearance of reconstructed NAC has been largely satisfactory with an average of 1.5 for the study group with points ranging from 0 (Bad) to 3 (Excellent). With 1 point being satisfactory and 2 being good, we determined that the overall score of 1.5 (mean) indicates more than satisfactory on patient’s view of procedure outcome. Collective outcome in our study in early post-operative and later follow up has been satisfactory. (Figure 7)


Nipple reconstructed from the burned tissue using skate flap is effective and simple. The advantage of use of burned tissue is that scared tissue is rigid and so there is less chance of shrinkage and retraction and this helps to maintain a lasting nipple projection. Planning of oversized nipple to allow for subsequent shrinkage is important to maintain a lasting nipple projection. Pre-operative tattooing of the nipple does not affect flap survival. Short coming in our study is short term follow up. Reconstruction of NAC to match native breast is currently attainable goal, though, functional restoration is goal for the future.
Nipple reconstructed from the burned tissue using skate flap is effective and simple. The advantage of use of burned tissue is that scared tissue is rigid and hence lesser chance of shrinkage and retraction which helps to maintain a lasting nipple projection.
Subscribe now for latest articles and news.