Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 88-92
Review Article
Hamsaveena1 , M V Rashmi2
1Professor & HOD, Department of Biochemistry, Sridevi Institute of Medical Sciences & Research Hospital, Tumkur, Karnataka, India,
2Professor & HOD, Department of Pathology, Sri Siddhartha Institute of Medical Sciences & Research Centre, T Begur, Tumkur, Karnataka, India
Address for correspondence: M V Rashmi, Professor & HOD, Department of Pathology, Sri Siddhartha Institute of Medical Sciences & Research Centre, T Begur, Tumkur, Karnataka, India. E-mail: [email protected]
The new CBME curriculum differs from the older one by being more learner and patient centric, outcome based, aligned & integrated, and emphasis on skill development, attitudes, ethics & communication. The affective domain which was implicit in the curriculum, is now to be taught explicitly. Newer additions like foundation course, early clinical exposure and self-directed learning are introduced. The curriculum implementation support programme is making tremendous efforts in inculcating the new curriculum into day-to-day teaching. The curriculum committee has a huge task to train the faculty in their respective colleges for a smooth transition. Hence, a thorough understanding of the new curriculum by these members is very essential.
Keywords: Harden’s ladder, Integration
The introduction of Competency Based Medical Education 2019 by the Medical council of India has brought about remarkable changes into undergraduate medical education. Alignment and Integration are part of this new curriculum which is included across the phases. It helps an Indian Medical Graduate to achieve a holistic approach in patient care which reflects the real world.
Integration is defined as the organization of teaching matter to interrelate or unify the subjects which are frequently taught in separate academic periods or departments. It is education that cuts across subject lines & brings various aspects of curriculum together for meaningful association to focus upon broad areas of study. It brings a holistic approach to learning and draws together knowledge, skills, attitudes, communication and other soft skills for better understanding of the key concepts. Horizontal & vertical integration are the two types. Horizontal integration brings together disciplines/topics & subjects to deliver a meaningful & holistic learning. Vertical integration brings basic & clinical sciences together to break the traditional divide between basic & clinical sciences. The basic sciences are explicitly represented in all the years of undergraduate education & even in post graduate training & continued professional development.[1]
Integrated teaching has advantages in terms of: Reduction in fragmentation of medical subjects; prevents redundancy; helps students to apply their knowledge to clinical practice; promotes interdepartmental collaboration; rationalizes use of available resources.[2]
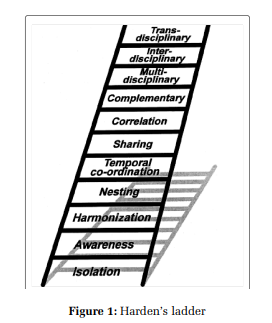
Professor Ronald M Harden was an endocrinologist before moving to become a full-time medical educationist. He is a renowned personality in medical education and with immense contribution to the field. Professor Harden has described the 11 steps in integration, which is called the Harden’s ladder (Figure 1). Subject / Discipline – based teaching at the lower four levels of the ladder and moving up the ladder, the emphasis is on integration across several disciplines. In the last step of the ladder, it’s the responsibility of the student to integrate in a given situation.[2,3]
Harden’ s ladder has been found to be a useful tool in getting a better understanding of integration. But, in our experience, we had difficulty making the participants have a clear concept of various steps. We felt the understanding was better when examples from practical experience were used. We have made an attempt to share such examples which could make a better understanding of various steps.
Step 1: Isolation
Faculty of each department work individually while planning and also during implementation.
Example: 1
st year disciplines - the topics scheduled: Department of Anatomy: Cardiovascular system. Department of Physiology: Endocrine system. Department of Biochemistry: Metabolic diseases. Here, one can see that there is no alignment of any topics and no attention is paid to related subjects. The major disadvantage is that the students don’t develop any relationship between subjects when taught in isolation. [3]
Step 2: Awareness
In awareness, the teacher in one subject is made aware of what is covered in other subjects in the curriculum. The teacher can take account of what colleagues cover in other parts of the course when planning for a class, avoiding redundancy and crossreferring. But there is no explicit attempt to provide integrated view of the subject to the student.[3]
Example: Dept. of Physiology: Physiology of thyroid glands - synthesis, secretion, transport, physiological actions, regulation and effect of altered (hypo and hyper) secretion of thyroid hormones. Department of Biochemistry - The functions of the thyroid, the tests that are commonly done in clinical practice to assess the functions of thyroid gland, abnormalities of thyroid gland.
Step 3: Harmonization
The faculty from the concerned departments consult through informal discussions between teachers or through curriculum planning committees. This encourages teachers to adapt their programs so that each course makes an appropriate contribution to the curriculum and overall curriculum objectives are more likely to be achieved.[3]
Example:
Department of Microbiology: Describe the etiopathogenesis and discuss the clinical evolution and the laboratory diagnosis of malaria. Department of Pathology: Define and describe the pathogenesis and pathology of malaria.
The staff in Department of Pathology make reference to malaria in brief and refresh the memory of what is learnt in microbiology during their topic on infections & infestations. Thus, an explicit connection with topics already learnt in other subjects is made.[3]
Step 4: Nesting
The teacher tries to bring in concepts from other subjects within a subject based course. It could be the clinical skills/concepts brought into a pre/para clinicals subjects or a basic skill introduced in clinicals subjects.[3–5]
Example 1: Department of Biochemistry: Tests that are commonly done in clinical practice to assess the functions of liver.
In the above class a relevance to clinical practice is introduced through - A case of alcoholic liver disease may be discussed during this class to bring in relevance of LFTs.
Example 2:
Department of Obstetrics & Gynaecology: Changes in the genital tract, cardiovascular system, respiratory, haematology, renal and gastrointestinal system in pregnancy.
In the above class, a relevance to basic knowledge/skill is introduced through - A discussion on normal physiology of the above systems before proceeding to the changes in pregnancy.
Step 5: Temporal Coordination The related organ systems or topics/diseases in subjects are scheduled around the same time. This is done in consultation with other disciplines. Though the concepts in each subject are learnt separately, the students have a high scope to relate the concepts while learning.[3–5]
Example for Organ Systems based Department of Anatomy: Anatomy of the heart. Department of Physiology: Properties of cardiac muscle including its morphology, electrical, mechanical and metabolic functions.
Department of Biochemistry: Basis and rationale of biochemical tests in cardiovascular systems.
Example for Topics/ Disease based:
Department of Pathology: Etiopathogenesis and pathology of myocardial infarction.
Department of Pharmacology: Anti angina drugs. The topic of heart is scheduled at the same time in the time table, so that the students can correlate better.
Step 6: Sharing
The faculty from two disciplines come together and share a class so as to avoid repetitions. Such sharing of classes is effective and efficient in imparting knowledge/skills to the students.
Example:
Department of Physiology: Physiology of liver function. Department of Biochemistry: Metabolism of bilirubin. Since, these two topics have many overlapping specific learning objectives, the SLOs may be clubbed together and a common consensus arrived at. The SLOs may be divided among the staff of respective departments depending on the importance in their subjects. Then the staff in each discipline may come together and teach in the same class.[3–5]
Step 7: Correlation
The topics dealt are subject or discipline based and they take up most part of the curriculum time. In a separate session on correlation, only areas of common interest are brought together. Example: Department of Anatomy: Anatomy of pancreas (1 hr) Department of Physiology: Physiology of pancreas (1hr) Department of Biochemistry: Biochemical changes by pancreatic hormones (1hr) Horizontal Integration Class: Case of Diabetes/diabetic coma/complications – is used as a linker for the integration class (2 hrs) with contribution from all the three departments. In a single session, all the three disciplines should come together and will stress on the importance of the above topics with regard to diabetes. The facilitators shall avoid teaching again the topics on pancreas but stress the role of pancreas only in diabetes. During assessment, questions are more focused on topics covered in individual subject class rather than on integration class.[3,4]
Step 8: Complementary
This type of integration is both subject based as well as integrated. The focus of teaching is a theme or topic to which the disciplines will contribute.
The teaching is subject based and in individual classes the focus is on the theme (not on the subject as in correlation). Running parallel to these individual classes is an integrated class where each subject teacher shall emphasize on the theme so that the student has a holistic approach to the theme. Individual subjects are given less importance in terms of time, resources and assessment.[3–5]
Example:
Theme: Diabetes in pregnancy Subject based classes are conducted individually in different departments: Department of Obstetrics & Gynaecology – Incidence, management and complications of DM in pregnancy (1 hr)
Department of Paediatrics: Management of neonates born to diabetic mothers (1 hr) Dept. of Community medicine: Burden of DM in the community (2 hr) Department of Medicine: Recent advances in the treatment of DM (1hr) Complementary teaching session on the Theme ‘Diabetes in Pregnancy’ (8 hr): A case of Gestational diabetes is used and various departments discuss around the theme in detail. During assessment, questions are based on integrated session rather than on individual sessions. In contrast to correlation which is subject based and each topic is dealt in detail and a common session brings in the relevance with a linker, the complementary integration places importance to the theme.
Step 9: Multidisciplinary
The topic is not dealt subject-based and it transcends subject boundaries. In one session the staffs from various departments impart knowledge as much necessary for the theme. Courses are developed around systems. The scenarios, a professional may have to deal in real time may be considered for such integrations.[3–5]
Example:
In the thyroid module of the endocrine system block, the contributions from different departments may be as follows:
Department of Physiology: To thyroid hormone synthesis and its regulation.
Department of Pathology: To the underlying pathophysiology of the processes.
Department of Pharmacology: To the action of antithyroid drugs.
Department of Surgery: To the management of goitre.
Department of Medicine: To the clinical manifestations and investigations of thyroid disease.
This kind of integration helps the students in as to what to expect and how to approach a case of thyroid disease.
CMEs where talks are arranged around a particular theme are examples of such multidisciplinary integration.
Example:
Topic of CME: Diabetes Department of Biochemistry: Regulation of blood glucose
Department of Pathology: Pathophysiology of Diabetes
Department of Medicine: Management of Diabetes and complications
Department of Surgery: Diabetic Foot management
Department of OBG: Gestational diabetes
Department of Paediatrics: Diabetes in children Step 10: Interdisciplinary
As Jarvis et al have described, it is ‘a study of a phenomenon that involves the use of two or more academic disciplines simultaneously’. This is a higher level of integration where the content of all or most subjects is combined into a new course. There is no subject demarcation in this level.[3,4]
Example:
Approach to acute abdomen: A case of acute abdomen in middle aged women is used for induction.
Department of Medicine, Surgery and OBG will discuss their approach towards diagnosis and management of that particular case without any subject
demarcation. Emergency medicine (initially started as a course, only in the recent past was converted as a degree) where there is no demarcation between the two subjects of medicine and anaesthesia and is an amalgamation of the above two mentioned disciplines. Another example being courses like geriatric medicine, laboratory medicine etc.
Step 11: Transdisciplinary
This is the highest level of integration. The emphasis is here on knowledge as exemplified in real world. It is the responsibility of the student to integrate all that is learnt in different disciplines when a real-life situation is encountered.[3,4]
Example:
When an intern sees a case of myocardial infarction in emergency, he integrates his knowledge of various disciplines like:
Department of Anatomy: Anatomy of the heart. Department of Biochemistry: Biochemical markers for diagnosis of MI.
Department of Pathology: Pathophysiology and investigations in a case of myocardial infarction. Dept of Pharmacology: Drugs used in MI.
Department of Medicine: Management of a case of MI.
With this understanding of different disciplines during the various phases of the course, the student should be able to manage a case of MI during internship.
Here, we have made an effort to explain the various steps of Harden’s ladder with suitable examples. It has been a difficult task to find examples especially for higher order. Unless these are explained with examples which are applicable in day-to-day practice, it is difficult for medical educators to understand and implement it. This would give an opportunity for the faculty to use similar examples from their subjects to understand different levels of integration
Alignment and Integration is integral part CBME curriculum. A thorough understanding of different levels of integration is essential for effective implementation of new curriculum. It needs more training and clarity in this aspect to all medical educators, as it requires faculty from across phases to work in coordination to make it effective and relevant.
Subscribe now for latest articles and news.