Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i1.22.492
Year: 2023, Volume: 9, Issue: 1, Pages: 110-117
Review Article
B M Soumya1 , Lalita Sharma2 , Vardendra Kulkarni3 , C R Preethi4
1Associate Professor of Pathology, Department of Pathology, JJM Medical College, Davangere, Karnataka, India,
2Postgraduate of Pathology, Department of Pathology, JJM Medical College, Davangere, Karnataka, India,
3Professor and Head, Department of Pathology, JJM Medical College, Davangere, Karnataka, India,
4Professor of Pathology, Department of Pathology, JJM Medical College, Davangere, Karnataka, India
Address for correspondence:
Lalita Sharma, Postgraduate of Pathology, Department of Pathology, JJM Medical College, Davangere, Karnataka, India.
E-mail: [email protected]
Received Date:19 September 2022, Accepted Date:12 April 2023, Published Date:15 May 2023
The spectrum of lipomatous lesions ranges from benign to highly malignant disease. Differentiation between these mesenchymal lesions is important for pathologist as well as clinician to indicate prognosis and choose the most appropriate treatment. Hemosiderotic firohistiocytic lipomatous tumor (HFLT) is a rare subtype of lipomatous tumor. The diagnosis is usually based on clinical, histological, and immunohistochemical (IHC) information. We reported a case of 56 years old man with a painful mass in the dorsal aspect of the thigh showing an unusal clinical presentation but a characteristic histological and IHC features. In this article we have retrospectively reviewed the 67 cases of HFLT reported in literature so far along with one case reported at our institution. The review focuses on clinicopathological and histomorphological characteristics of HFLT and the related entities. The hallmark of HFLT and its related lesions is complex admixture of mature adipose tissue, spindle tumor cells with striking deposition of hemosiderin pigment. Even though HFLT shows marked predeliction for the distal extremeties especially the foot/ ankle with a female preponderance, they can occur at uncommon site such as thigh and also in males as seen in our case.
Keywords: Pleomorphic hyalinizing angiectatic tumor, Hemosiderotic fibrolipomatous tumor, Myxoinflammatory Fibroblastic Sarcoma, Hemosiderin, Lipoma
Hemosiderotic Fibrohistiocytic Lipomatous Tumor (HFLT), Pleomorphic Hyalinizing Angiectatic Tumor (PHAT), and Myxoinflammatory Fibroblastic Sarcoma (MIFS) are rare mesenchymal neoplasms with a tendency for the distal lower extremities. Although each of these entities have been described independently in literature, various histological and genetic observations over the past two decades have led to speculation that these tumors may be interrelated. This hypothesis is based on both histomorphological and genetic features, but the exact relationship between these three entities remains a topic of controversy and debate for the scholars. In this article, we have analyzed the key histomorphologic and immunohistochemical (IHC) features of a case of HFLT which showed an unusual clinical presentation and a discussion about the closest differentials which easily confuses the pathologist and lead to chances of misdiagnosis. Since the available literature over these entities are limited, we hereby will evaluate the relationship between these tumors.
The spectrum of lipomatous lesions ranges from
A 63-year-old male presented to surgery department of our institution with a painless swelling over upper one third of right thigh. The patient had noticed the lesion one and a half year before, which has gradually progressed to the present size (24×12 cm). There was no significant medical history or history of trauma. Family history was noncontributory. On physical examination, swelling was 24x12 cm with ill-defined margins, which was non tender, with no local rise of temperature. On further examination, patient had difficulty in flexion and external rotation of thigh and a resistance involving half the anterior medial side of the thigh was present. MR imaging revealed lipomatous lesion of the right thigh measuring 28× 13 × 10 cm with irregular boundaries. The lesion showed multiple far-reaching intramuscular and subfascial extensions. The assessment of internal structures showed a homogeneous, lobulated lesion suspicious of liposarcoma.
Complete tumor resection was performed with free margins. After resection the specimen was subjected to histopathological evaluation.
The specimen was fixed in 10% neutral formalin, then conventional paraffin sectioning and hematoxylin and eosin (H&E) staining were performed. The morphology of tumor tissue was observed under a light microscope.
On gross examination, lipomatous lesion measured 28×13×10cm. It was darker yellow than the normal surrounding fat. External surface was well circumscribed, congested and showed blood vessels. Cut surface showed collated appearance. Cystic areas were filled with necrotic debris and hemorrhagic areas were made out (Figure 1).

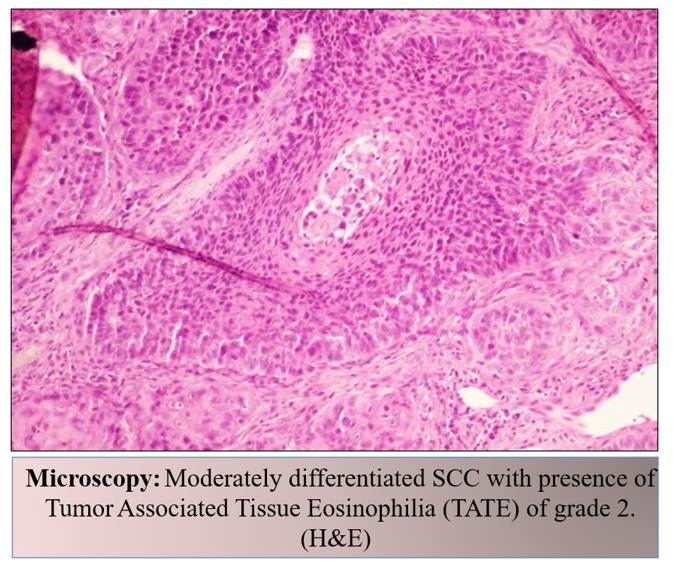
Microscopically, ten representative samples throughout the whole tumor were reviewed. Histopathological examination revealed a neoplastic lesion composed of spindle cells infiltrating into adipocytic component in a honey comb pattern . These spindle cells had elongated, vesicular nuclei, inconspicuous nucleoli and scanty cytoplasm. The adipocytic component was mature without atypia and no lipoblasts were seen. There were numerous small to large ectatic blood vessels with a number of them showing organising thrombi, aggregates of histiocytes containing hemosiderin pigment (Figure 2). No evidence of increased mitotic activity was noted. On IHC staining of CD34, a notable diffuse staining primarily of the spindle cells, fibrocytes and vascular endothelium was seen (Figure 3). On staining with CD68 we found out positive staining for macrophage lineage such as tissue histiocytes. (Figure 4)



By combining histology and IHC features of resected specimen with clinical information, the diagnosis of HFLT was established. There were no operative or post-operative complications noted. Eighteen months after the excision, the patient continued to show no signs of recurrence.
We reviewed 67 cases of HFLT from the literature, published in English and Portuguese language which were available at Pubmed data base (Table 1).
Case reports, articles that diagnosed HFLT with adequate evidence supported by gross examination, histology, biopsy and previous recurrrences were included. Demographic data such as age at diagnosis, gender, location and size were recorded. An attempt to look for clinico-pathologic features of HFLT along with IHC features was done. All the 67 cases were studied using descriptive statistics.
|
Data base |
Results |
|
Pubmed |
8 Original articles 3 Letter to editor 1 Updating article 3 Case series 7 Case reports 4 Review articles 1 Research article 1 Short communication 1 Scientific article |
The demographic characteristics of all HFLT included were studied and tabulated (Table 2). Our review of the literature suggests that HFLT predominately presents in middle-aged women (median age being 50 years and mean age being 51 years). Age group ranged from 7 months to 78 years, the ratio of male to female was 1: 2.6 with close to half (46%) the cases having a history of trauma or vascular disease.
HFLT occurs within the soft tissue of limb extremities, with foot/ankle accounts for 77%, but also involves the hands,1, 2, 3 forearm,4, 5 wrist6 and one case involving cheek and finger. 7
It has been reported that majority cases of HFLT are characterized by CD34 expression in spindle cells and vascular endothelium.
It was noted that HFLT needs to be pathologically distinguished from related adipocytic lesions such as PHAT and MIFS which share similar location and morphologic characteristics. Summary of key morphological and genetic features of adipocytic lesions are tabulated in Table 3.
|
Study |
Year |
Number of patients |
Gender |
Average age in years |
Localisation |
Size |
|
Marshall et al. 7 |
2000 |
10 |
2 - Male 8- Female |
50.6 |
8 - Foot 1 - Cheek, 1- Finger |
Range 2.5 -17cm |
|
Kazakov et al. 8 |
2005 |
2 |
2 - Female |
54 |
1- Foot 1- Foot |
6x5x4 cm |
|
Browne et al. 1 |
2005 |
13 |
6 - Male 7 - Female |
49 |
12- Ankle/foot 1 - Hand |
Range 1- 13cm |
|
Luzar et al. 9 |
2006 |
1 |
Female |
47 |
Ankle |
1.9x1.2 cm |
|
West et al. 10 |
2007 |
1 |
Female |
38 |
Foot |
NA |
|
de Vreeze et al. 11 |
2008 |
1 |
Male |
66 |
Thigh |
19x8x4 cm |
|
Wettach et al. 12 |
2008 |
1 |
Female |
35 |
Foot |
NA |
|
Hallor et al. 13 |
2008 |
1 |
Female |
40 |
Ankle |
NA |
|
Ramalho et al. 14 |
2009 |
1 |
Female |
33 |
Knee |
10x8x6 cm |
|
Moretti et al. 15 |
2010 |
1 |
Female |
56 |
Foot |
7x5x2 cm |
|
Antonescu et al. 2 |
2011 |
14 |
2 - Male 12 - Female |
45 |
13 - Foot 1 - Hand |
NA |
|
Sawalha Setal. 3 |
2011 |
1 |
Female |
55 |
Hand |
3x1 cm |
|
Carter et al. 4 |
2014 |
7 |
3 - Male 4 - Female |
53 |
4 - Foot 3 - Forearm |
NA |
|
O’Driscoll et al. 5 |
2014 |
5 |
3 - Male 2 - Female |
60 |
4 - Foot 1 - Forearm |
18 cm |
|
Marusic Z et al. 16 |
2014 |
1 |
Female |
57 |
Ankle |
15x5 cm |
|
Zreik et al. 17 |
2016 |
1 |
Female |
77 |
Foot |
NA |
|
Morency et al. 18 |
2016 |
1 |
Female |
55 |
Foot |
3x1 cm |
|
Wilk et al. 19 |
2016 |
1 |
Female |
45 |
Foot |
14x6 cm |
|
Etchebehere et al. 20 |
2016 |
1 |
Female |
38 |
Thigh |
22x18x11cm |
|
Hou et al. 21 |
2018 |
1 |
Male |
50 |
Knee joint |
4x2.5x1.9cm |
|
Bourhroum N et al. 22 |
2019 |
1 |
Female |
50 |
Ankle |
7 cm |
|
Pang CY et al. 6 |
2021 |
1 |
Female |
45 |
Wrist |
NA |
|
Current study |
2022 |
1 |
Male |
63 |
Thigh |
28x13x10cm |
NA - Not available
HFLT is a rare benign fibrolipomatous lesion first described as an entity in 2000 by Marshall - Taylor and Fanburg - Smith. It accounts for 0.2% of benign lipomatous lesion. 7
HFLT generally affects the ankle and the dorsum of the foot, although it may appear in other locations such as cheeks and hands. It typically affects adults, more commonly females, in the 5th and 6th decades of life. The distinct feature about our case is its huge size, site and occurrence in male. Thigh is not the usual site of presentation. Our case and only two other cases in literature (de Vreeze et al. 11 and Etchebehere et al.20) have reportedthigh as the location.
Histologically, it is characterized by a lipomatous lesion composed of three elements occurring in varying proportions. These elements include mature adipocytes, spindle cells and hemosiderin pigment, which is present predominantly in macrophages within the spindle cell areas, whose original deposit is unclear. The mature adipose tissue is infiltrated by strands of fibrous tissue featuring fibroblastic spindle cells and hemosiderin deposits.
Scattered areas with atypical pleomorphic cells may be present. Focal clusters of ectatic blood vessels as seen in PHAT are not uncommon. Chronic inflammatory cells are usually seen in the background. Mitosis or necrosis are usually not seen. CD34 positivity clearly differentiates the fibroblastic differentiation while CD68 positivity shows diffuse staining for the macrophages. 1
There is an ongoing debate about the resemblance of early PHAT and HFLT; some consider HFLT a precursor lesion of PHAT, implicating HFLT to be a neoplastic lesion, 8, 23others consider HFLT an individual more reactive lesion. 1, 9
The hypothesis that PHATis related to HFLT was first suggested by Folpe and Weiss 24 in their 2004 study on 41 PHAT cases. These investigators noted that in nearly 50% of their cases, there was the presence of areas which were morphologically indistinguishable from HFLT at the periphery.
These HFLT-like areas were labeled “early PHAT,” and were felt to represent the precursor lesion to classic PHAT 24.PHAT and HFLT both shares recurrent t(1;10) (p22;q24) rearrangement involving the TGFBR3 and MGEA5 genes. 13, 2
Same as HFLT, PHAT also has usually middle-aged adults preponderance and a proclivity for the lower extremities, though a few cases has occurred at the sites such as the arm, thigh, buttocks, or trunk with a median size of approximately 6cm. Becauseangiectatic vessels is a prominent feature, PHAT quite a few times is clinically mistaken for a hematoma or vascular neoplasm. PHAT is a vaguely circumscribed mass composed of spindled or pleomorphic cells surrounding clusters of thin-walled, ectatic vessels with sub-endothelial and intraluminal fibrin deposits and perivascular hyalinization.
Although PHAT could appear circumscribed at low power, the margin is typically infiltrative. The lesional cells range from spindled to strikingly pleomorphic and shows frequent intranuclear inclusions. Mitotic activity in PHAT is very low (<1/50 HPF). Hemosiderin deposits can be seen in macrophages or in the cytoplasm of the lesional cells. Scattered inflammatory cells are usually present. 25
Myxoid stroma is focally present and usually there is a prominent inflammatory component. Cytologically, HFLT is consists of bland fibroblasts without significant mitotic activity and may contain scattered osteoclast-type giant cells. Small ectatic vessels with mural hyalinization or fibrinous thrombi may be present. 1, 24 HFLT-like areas can be found at the periphery or admixed with otherwise typical examples of PHAT. This observation led to a hypothesis that HFLT may well be a precursor lesion to PHAT. 24
In few rare cases it is seen that, PHAT and HFLT has progressed to a sarcoma of variable histologic grade, more often with in the setting of recurrences.13, 2, 4, 17 The sarcomas in such cases have myxoid stroma and a prominent inflammatory infiltrate and shows morphologic resemblance to MIFS. Solid, undifferentiated spindle cell sarcoma-like morphology has also been reported. 17
Most PHATs and HFLTs are both positive for CD34 and negative for S100, SMA, and desmin. 7, 4, 23, 24
MIFS also referred as “inflammatory myxohyaline tumor of the distal extremities,” 26 “acralMIFS,”27 and “inflammatory myxoid tumor of the soft parts with bizarre giant cells,”28 is a locally aggressive, rarely metastasizing, fibroblastic tumor of borderline malignancy that typically involves the distal extremities of middle-aged adults.
The marginal region of a PHAT, and MIFS demonstrates overlapping histomorphogy with HFLT. There is seen relatively mild spindle-cell infiltration of adipose tissue and deposition of hemosiderin. However, PHAT shows obvious plexiform expansion of thin-walled vessels with fibrin-like material deposition, and cytoplasmic pseudo inclusion bodies seen with in the nuclei of tumor cells. MIFS lesions contain high mucus-but low adipose-content, while usually little or no mucus is produced in HFLT
Literature suggests that there does not seem to be a direct morphologic link between HFLT and MIFS, and the available molecular genetic data within the literature are contradictory, likely attributable to the use of different morphologic criteria for the diagnosis of MIFS by different investigators. Although cases are described as representing “hybrid HFLT-PHAT,” the preponderance of evidence suggests that such lesions are way more closely associated with HFLT and PHAT representing a sort of morphologic progression to high grade myxoid sarcoma.
Ambiguity existed about reactive or neoplastic origin of HFLT. It is now well-established on the basis of histomorphology and molecular genetic evidence that HFLT and PHAT represent different manifestations of a single entity, with HFLT representing the precursor or “early” lesion of classic PHAT. The hallmark of these lesions is complex admixture of mature adipose tissue, spindle tumor cells with striking deposition of hemosiderin pigment. Even though HFLT shows marked prediliction for the distal extremeties especially the foot/ ankle and female gender, they can occur at uncommon site such as thigh and in a male patient as seen in our case.
|
Diagnosis |
Morphologic Features |
Association with HFLT |
Molecular alteration |
|
HFLT |
Mature adipose tissue, myxoid stroma CD34-positive spindled cells with intracytoplasmic hemosiderin deposition CD68 -positive macrophagesseen Small aggregates of variable sized blood vessels Areas resembling “miniature” PHATs |
Not applicable |
Frequent |
|
PHAT |
Clusters of thin-walled, ectatic blood vessels, containing organizing thrombi and surrounded by amorphous eosinophilic material Pleomorphism seen, CD34-positive tumor cells with intranuclear pseudoinclusions and intracytoplasmic hemosiderin deposition Low-mitotic activity Chronic inflammatory cell infiltrate Peripheral areas identical to HFLT |
Yes |
Frequent |
|
MIFS |
Multinodular and poorly circumscribed hyalinized zones, typically containing bizarreappearing cells with prominent macronucleoli Areas of dense chronic inflammation myxoid nodules, often containing multivacuolated (“lipoblast-like”) fibroblastic cells Mitotic activity is low Necrosis not seen Arborizing, thick-walled vessels as seen in myxofifibrosarcoma is usually absent here CD34 positive |
No |
Infrequent |
|
HFLT with progression to myxoid srcoma (“hybrid HFLT-MIFS) |
Areas of typical HFLT Myxoid sarcoma showing a well-developed, thick-walled vasculature Pseudolipoblasts may be seen Absence of hyalinized zones Absence of “Reed-Sternberg-like” or “virocytelike” cells |
Yes |
Frequent |
Adapted from: Boland & Folpe 25
HFLT: Hemosiderotic Fibrohistiocytic Lipomatous Tumor; PHAT: Pleomorphic Hyalinizing Angiectatic Tumor, MIFS: Myxoinflammatory Fibroblastic Sarcoma; TGFBR3: Transforming Growth Factor Beta Receptor 3; MGEA5: Meningioma Expressed Antigen 5; IHC: Immunohistochemical
Nil
References
Subscribe now for latest articles and news.