Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i01.005
Year: 2016, Volume: 2, Issue: 1, Pages: 24-29
Original Article
Aparna R Dikondwar1, Aarti A Dani2
1Junior Resident, Department of Pathology, Superspeciality Hospital, Nagpur, Maharashtra, India,
2Associate Professor, Department of Pathology, Superspeciality Hospital, Nagpur, Maharashtra, India
Address for correspondence: Dr. Aparna R Dikondwar, Department of Pathology, Superspeciality Hospital, Nagpur, Maharashtra, India. Phone: +91-8888863689. E-mail: [email protected]
Background: Space occupying lesions(SOL) of spinal canal are usually managed by excision.However correct diagnosis is essential for management decision.Though spinal lesions can be localised and diagnosed precisely with the help of neuroimaging techniques, still the diagnosis of any central nervous system SOL must ultimately be made by histological examination of tissue removed by surgical biopsy.
Aims: To review the histologic spectrum of spinal space occupying lesions and to observe the relative frequency of different lesions along with their clinical profile with respect to age, sex, compartmental distribution, and spinal level involved.
Materials and methods: Over a period of 5-years, 72 specimens (biopsy as well as surgical) of spinal space occupying lesions were studied in a tertiary care hospital in central India.
Results: The most common age group affected was 41-60 years (35.08%) with a male preponderance. The majority of the lesions were neoplastic 61 (87%) mostly benign or low grade. The most common histologic diagnosis was benign nerve sheath tumor 22 (32.6%). All histopathological types, except meningioma, were more common in males as compared to females.
Conclusion: Tissue diagnosis is imperative due to a wide variety of lesions in this area with differing prognosis and treatment modalities.
KEY WORDS:Spinal space occupying lesion, Pathologic spectrum, Histopathology, spinal lesion
IntroductionSpace-occupying lesions (SOLs) of the spinal canal can lead to compression and distortion of the surrounding neural tissue. SOLs make their space by atrophy of adjacent spinal tissue with resultant neurological deficits. The advances in neuroimaging techniques over the last few decades has revolutionized the field of neurologic diagnosis, still the diagnosis of any central nervous system SOL must ultimately be made by histological examination of tissue removed by surgical biopsy.[1] Cytologic preparation as well as intraoperative frozen section, can provide a rapid diagnosis which can help the surgeon in management decision intraoperatively, but histology determines the nature of lesion whether it is a neoplastic or an inflammatory lesion as well as the prognosis and treatment modalities. Tumors are the most common spinal SOLs; they constitute 15-20% of central nervous system tumors.[2,3] The location of a spinal tumor and its cell of origin hasf an important anatomic correlation that serves to guide diagnosis and treatment. They may arise from neural tissue, meninges, surrounding bone and soft tissues, from embryonal rests or metastatic deposit. Based on the location, they are classified as extradural, intradural-extramedullary (IDEM), and intramedullary spinal cord tumors (IMSCT). Extradural lesions constitute the lesions of the osseous spine, epidural space, and paraspinal soft tissue. IDEM lesions are located under the dura mater but outside the spinal cord, whereas intramedullary lesions are located in the parenchyma of the spinal cord.[4] The histology of spinal cord tumors is similar to their intracranial counterparts however the incidence of various lesions varies. The objective of this study was to study the histologic spectrum of these lesions, to observe the relative frequency of different lesions along with their clinical profile with respect to age, sex, and compartmental distribution and spinal level involved.
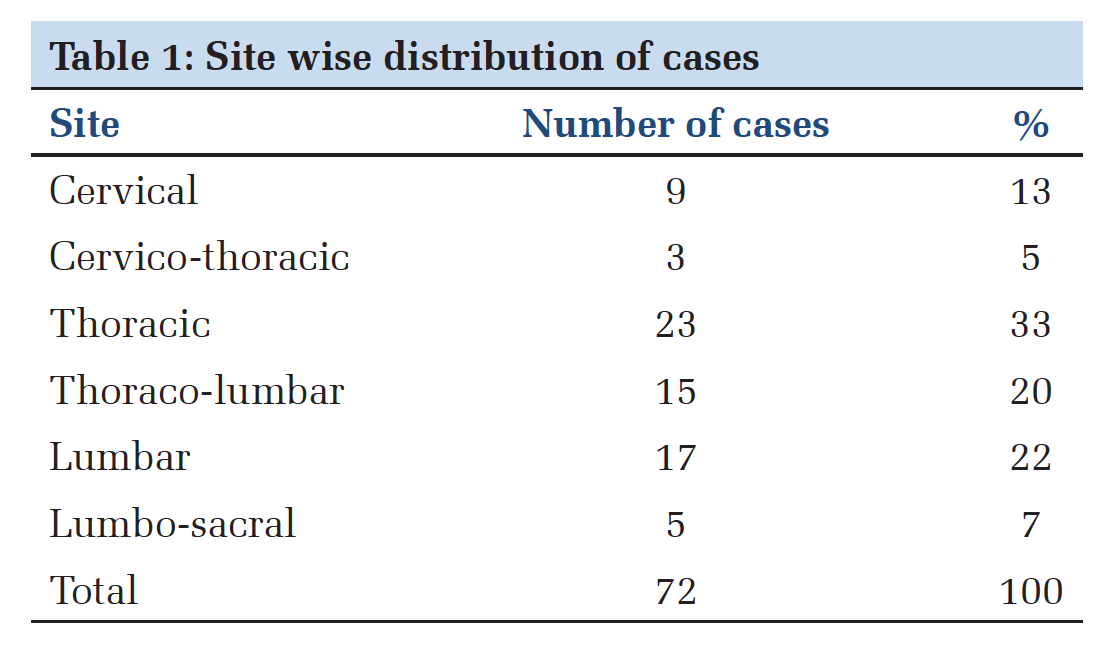
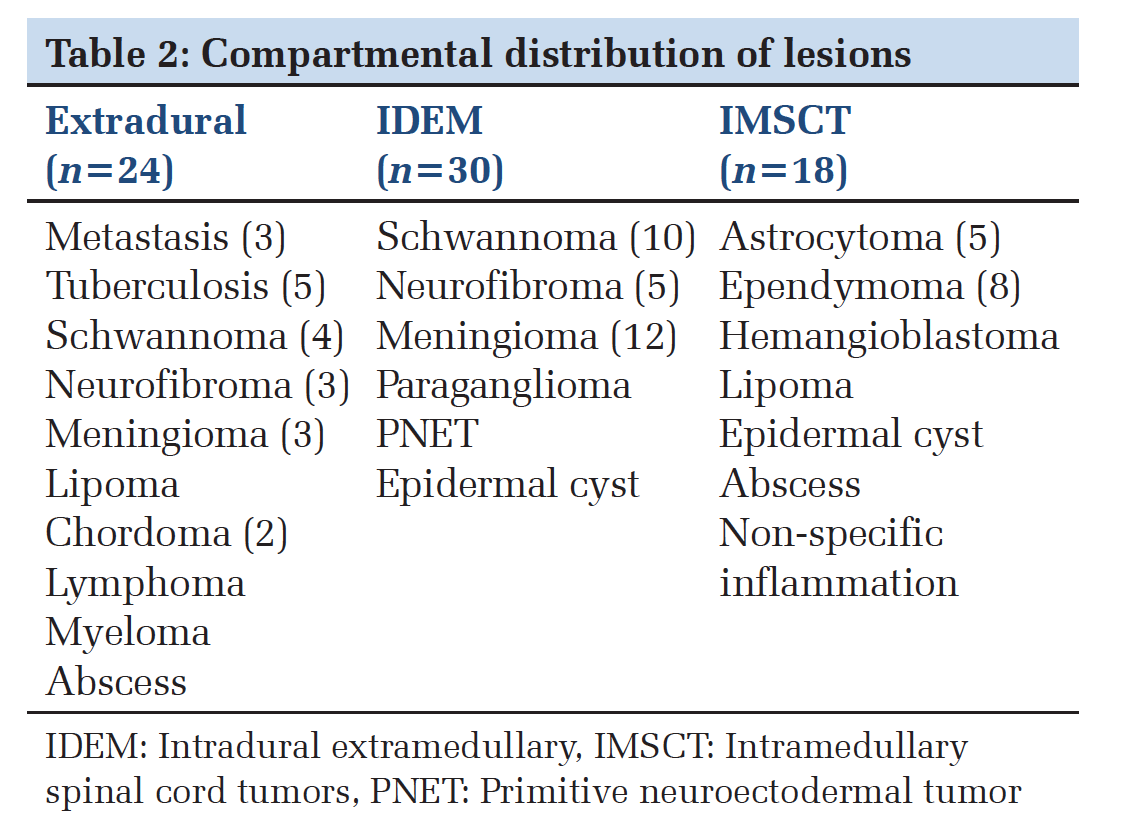
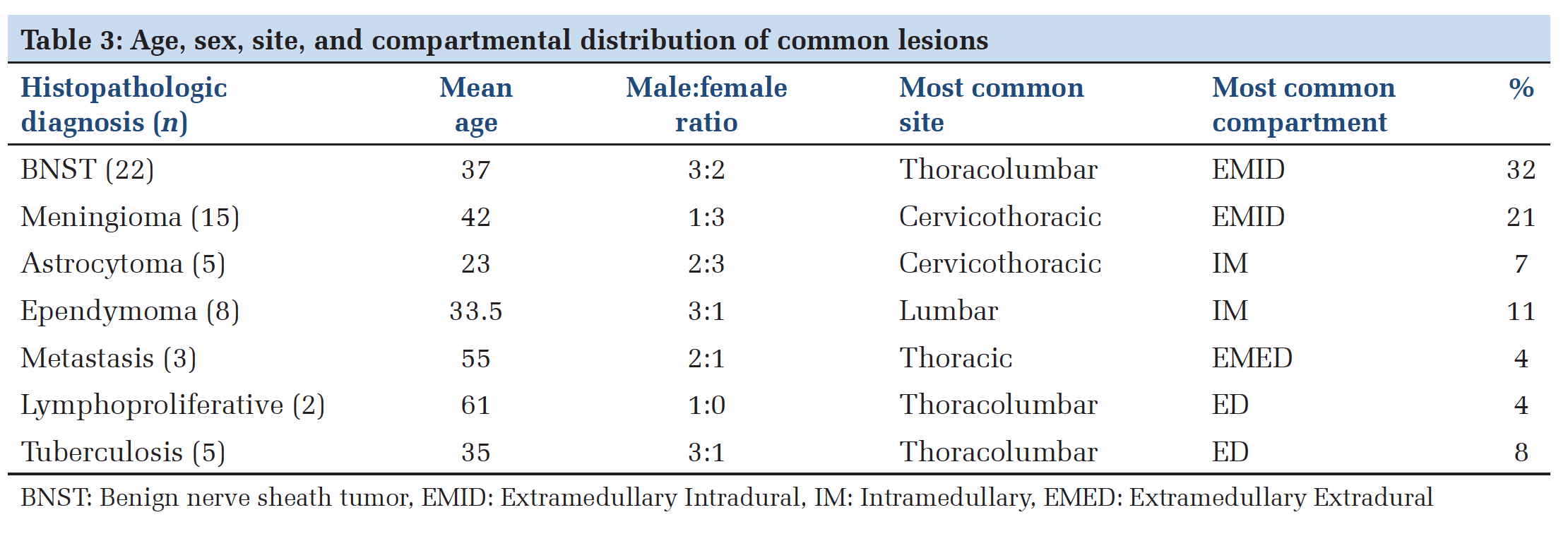
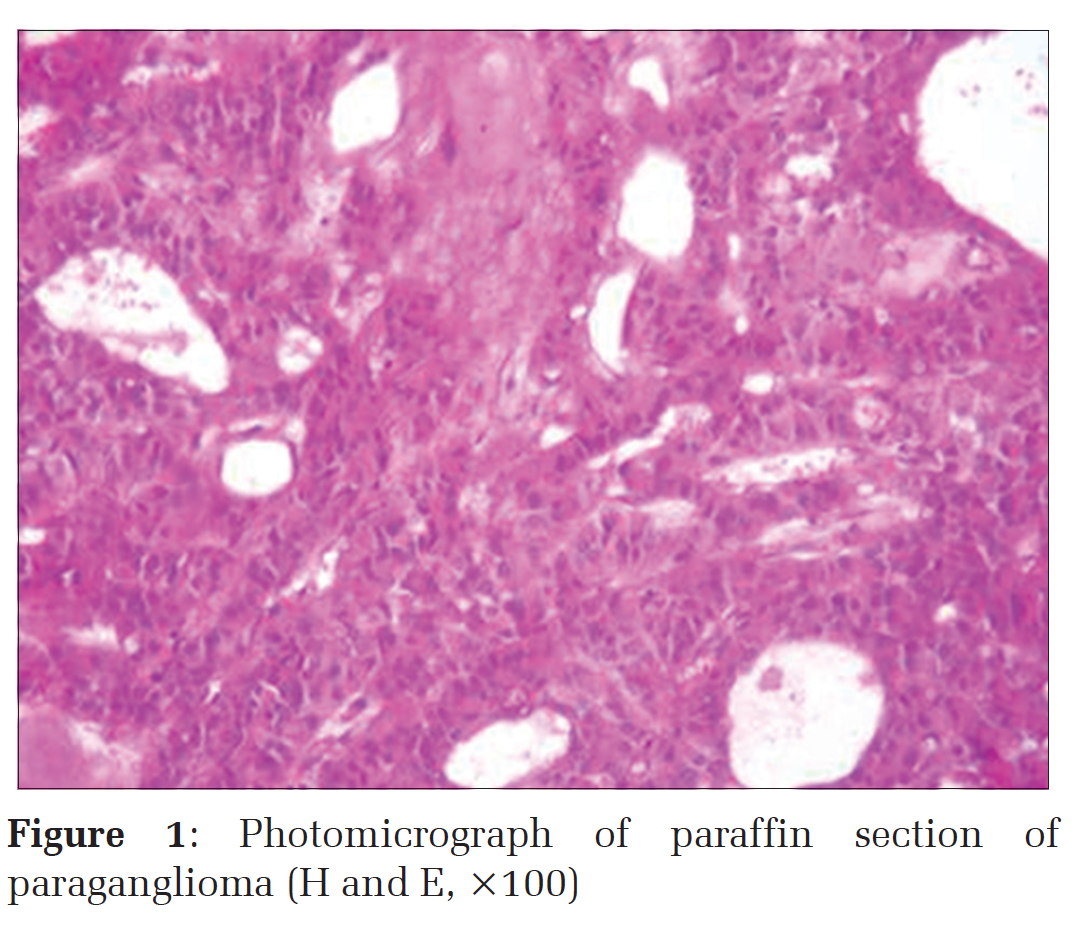
Materials and MethodsThis was a retrospective study of 5 years done in a tertiary care hospital of central India having a well-equipped neurosurgery department, operation theater and patient’s referral. During this period, we received 72 specimens (biopsy as well as surgical) from lesions of the spinal cord and adjacent structures. Cytological diagnosis was requested in 57 cases. All indoor patients from neurosurgery department having clinical signs and symptoms as well as imaging features suggestive of spinal SOL were included in the study while primary bone tumors and congenital anomalies including vascular malformations not involving cord were excluded.Patient’s medical history, physical examination findings, and radiological examination records were obtained. Specimen was fixed in 10% formalin. Routine histopathological processing was done. Hematoxylin and eosin stained sections were prepared. This was supplemented by appropriate special stains whenever required. Cytologic preparations were also made whenever requested for rapid diagnosis. The recent World Health Organization (WHO) Classification (2007)[5] of Central nervous system tumors was used for classification and grading of the tumor. ResultsWe reviewed 72 cases, of spinal SOLs. Age of the patients ranged from 9 to 75 years with mean age of 37 years at the time of surgery. The largest age group affected was 41-60 years (35.08%). There was a male preponderance with 46 (65%) patients being males and 26 (35%) patients being females. The most frequently involved spinal level was thoracic 23 (33.33%), followed by lumbar 17 (22%), thoracolumbar 15 (20%), and cervical 9 (13%) [Table 1]. Compartmental distribution of lesions showed 28 (40%) lesions were extramedullary intradural, 25 (35%) extradural, and 18 (25%) intramedullary [Table 2]. The most common complaint was nerve root pain (57.89%) followed by back pain (54%), paraparesis (47%), and paresthesia (43.85%). The demographic profile of patients is represented in Table 3.We observed a variety of benign, malignant, and inflammatory lesions. Out of total 72 cases in 61 (87%) cases lesions were neoplastic while nonneoplastic lesions constituted 11 cases (13%). The most common histologic diagnosis was benign nerve sheath tumor (BNST) 22 (32.6%) cases out of which 14 cases were diagnosed as schwannoma, 8 cases were diagnosed as neurofibroma. Mean age of presentation was 37 years with male:female ratio 3:2. The most common site was thoracolumbar with IDEM location being most common. There was a case of neurofibromatosis I in our study. Grossly, the lesions were globular and well-circumscribed. Histologically schwannoma showed a biphasic pattern, cellular Antoni A, and hypocellular Antoni B areas while neurofibroma showed spindleshaped cells arranged in short bundles having wavy nuclei against myxoid background. Meningioma was the second most common tumor 15 (22%) cases. Mean age of presentation was 42 years with male/female ratio 1:3. The most common site was cervicothoracic with IDEM location being most common. Psammomatous meningiomas constituted 50% of the cases. One case was of transitional meningioma while others were meningothelial meningiomas. Out of five (6.94%) cases of astrocytoma, two were low grade astrocytoma, diagnosed in a 14 years male and a 12 years female. Two were pilocytic astrocytoma, diagnosed in a 31 years male and a 20 years female with tumor involving lower cervical and upper thoracic cord, respectively and one was high-grade glioma (in 17 years male). Male:female ratio was 2:3. There were 8 cases of ependymoma; mean age of presentation was 33.5 years with male:female ratio 3:1. The most common spinal level involved was lumbar, and chief complaint was back pain. There was one case of myxopapillary ependymoma, four cases of classic low-grade ependymoma while three cases were of high-grade ependymoma. Myxopapillary ependymoma was seen in filum terminale. Histology showed perivascular pseudo papillae lined by columnar cells and perivascular and intracellular mucin. Three cases (6.52%) of metastasis were diagnosed. In all these cases, the lesion was extradural and thoracic spine was involved. Patients presented with back pain being the most common complaint. All were metastasis of adenocarcinoma from the breast, colon, and lung. There was one case (2%) of multiple myeloma (T11-12). He was a 63-year-old male who presented with back pain and paraparesis. One case (2%) of lymphoma (T4) was diagnosed in a 60-yearold male patient. He was a known case of non- Hodgkin’s lymphoma (HIV negative) who presented with a history of back pain followed by paraplegia. Magnetic resonance imaging (MRI) showed irregular lobulated mass compressing the spinal cord. Chordoma, a tumor arising from remnants of notochord was seen in three cases, 2 males (56 and 65 years) involving lumber spine, and a female of 28 years with the cervical lesion. One case of paraganglioma was also diagnosed in a 52-year-old male who presented with back pain and radicular pain since 10 months. MRI revealed uniformly enhancing well-circumscribed intradural lesion at L3 level. Microscopy showed a trabecular pattern of cells within a prominent vascular network [Figure 1]. We also had rare tumors such as the primitive neuroectodermal tumor (PNET) in one case (2%). She was a 16-year-old female who presented with lower back pain radiating bilaterally toward legs since 3 months. MRI of the spine showed intramedullary tumor extending from L5 to S1. One case of hemangioblastoma was also diagnosed in 20 years female. It presented as a mural nodule on MRI at L1-2. It was not associated with Von Hippel- Lindau Disease. Histology showed large pale stromal cells packed between blood vessels of varying sizes. There were two cases of lipoma. Both were male. One was extradural while another was intramedullary. Both were in the thoracic region. Journal of Medical Sciences and Health/Jan-Apr 2016/Volume 2/Issue 1 27 Two cases were diagnosed as an epidermal cyst. The site of involvement was thoracic spine in both cases. One was located intradurally while other was intramedullary. Grossly, it was thin walled, unilocular pearly white in color due to keratin content. Histologically, they showed cyst lined by stratified squamous epithelium. The lesion has a benign course but may cause pressure effect. Diagnosis of tuberculosis was given in five cases (6.94%), it was the most common inflammation followed by pyogenic abscess two cases (2.7%) while one case was of non-specific chronic inflammation.
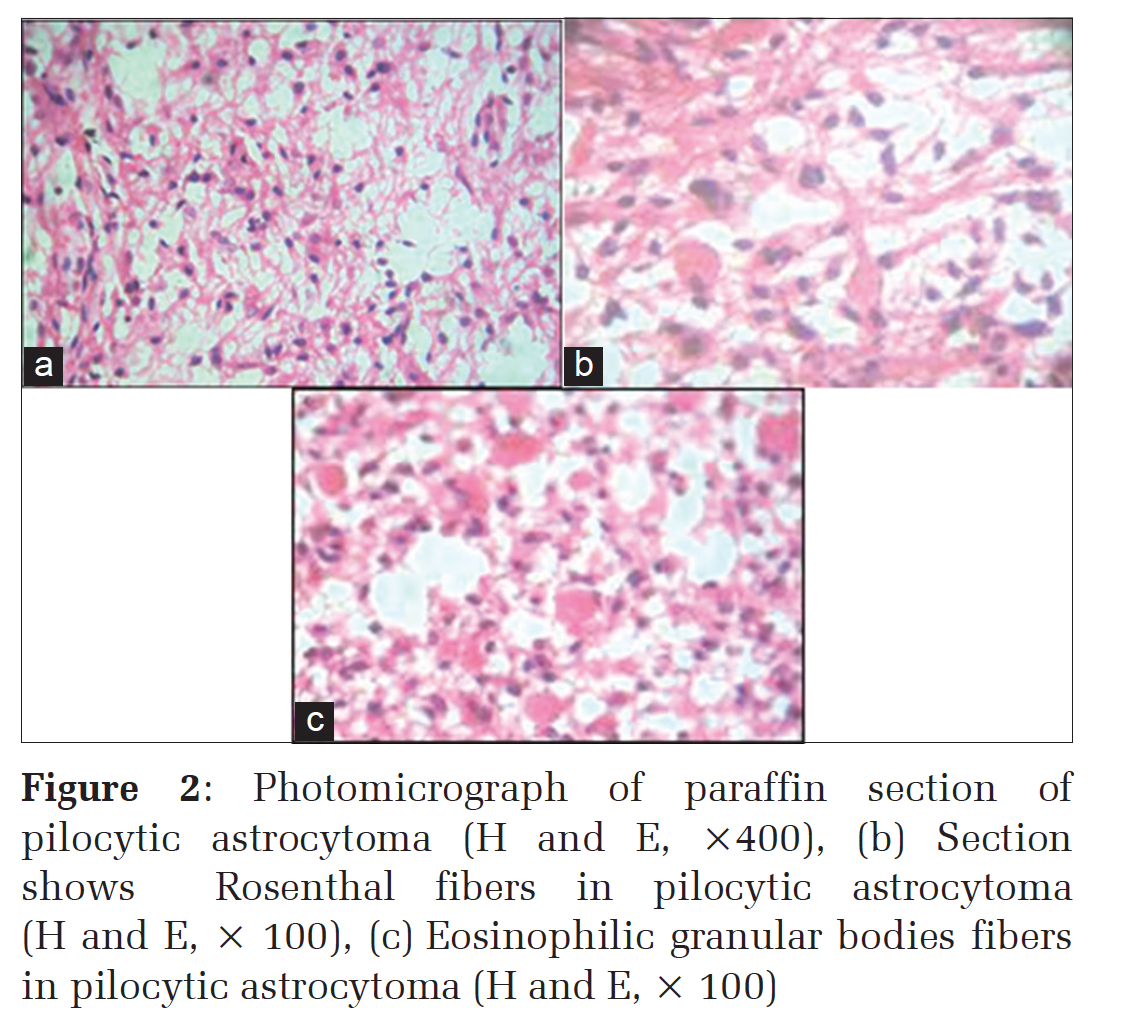
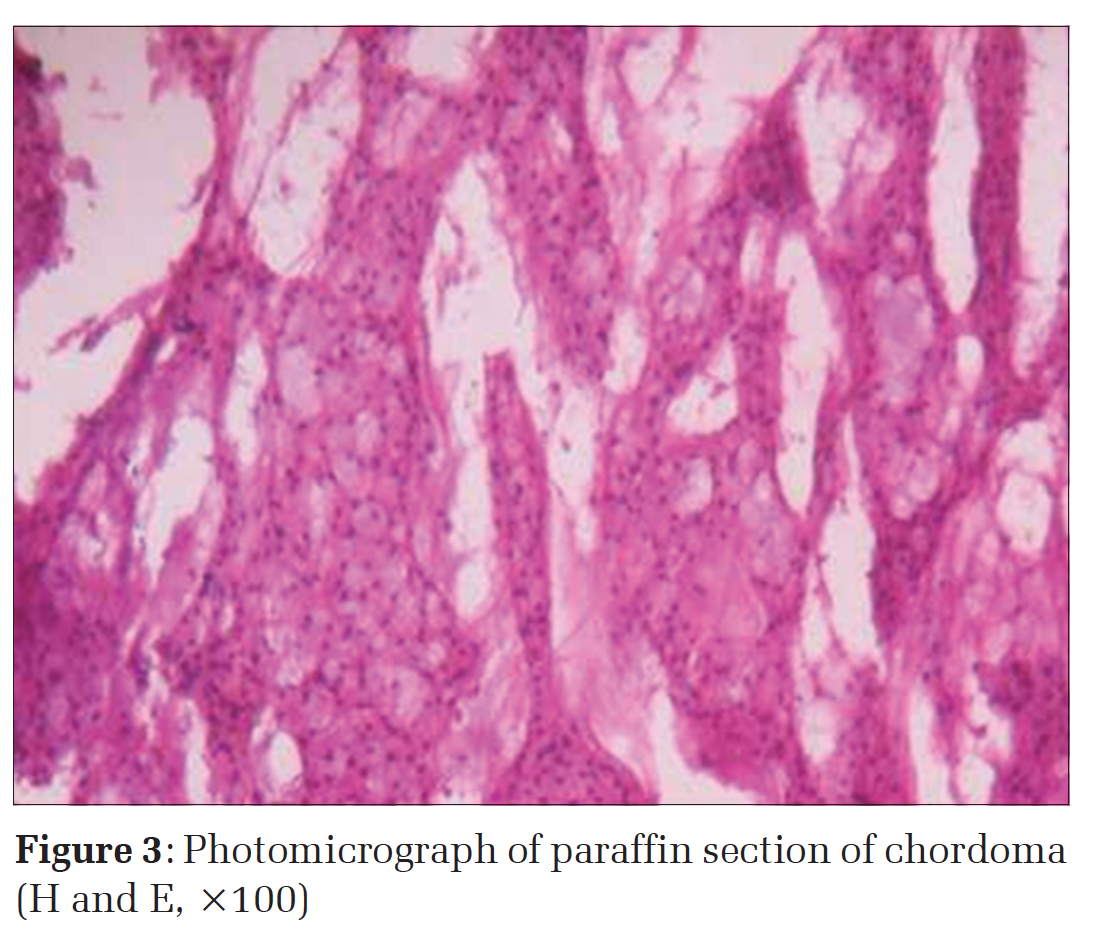
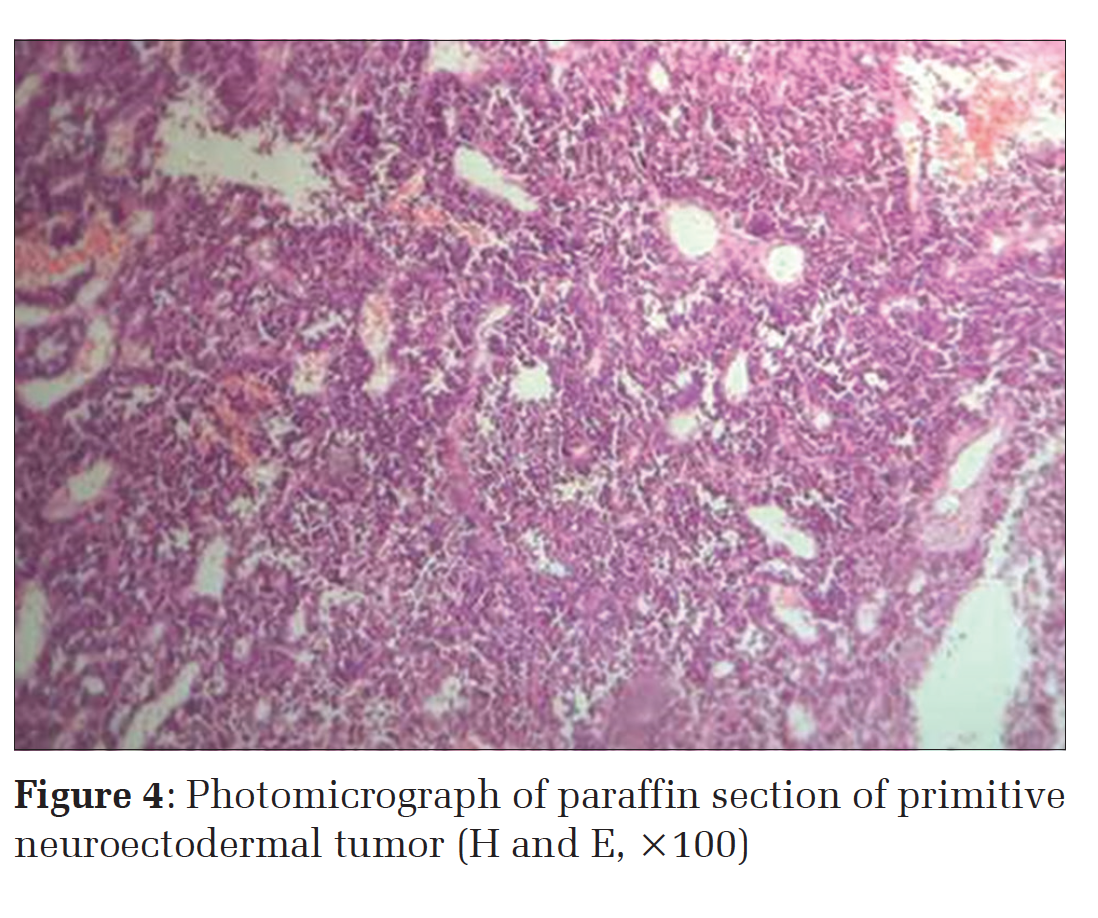
DiscussionThis study shows that the spinal lesions occur over a wide age range, with mean age at surgery being 37 years. Debnath et al. and Arora and Kumar also found similar wide age range in their study.[6,7] The largest age group affected was 41-60 years (35.08%). There was a male preponderance. In western population, primary spinal tumors are seen more commonly in females, whereas in Asia, male preponderance is seen.[8,9] We had a male to female ratio of 2:1 which is similar to other studies reported from Asia.[6,7] The literature suggests that 90% of the spinal tumors are IDEM while only 10% are IMSCT.[10] In the present study, most of the lesions were IDEM. Our results correlate well with previous studies done in Asia.[6,8,11,12] In the present study, BNST - schwannomas/ neurofibromas form the largest category of tumors 32% and the most common IDEM tumor followed by meningiomas. Other studies also found that these lesions are mostly IDEM and rarely intramedullary.[6,7] The differential diagnosis includes schwannoma and meningioma.[13] Debnath et al. also found schwannoma as the most common tumor after metastasis. Meningiomas formed the next largest group 22%; the incidence of meningioma is comparable to that reported in the world literature, the mean age was 42 years, and male/female ratio was 1:3 suggesting female preponderance. The most common site was cervicothoracic with most of the lesions being located intradurally. Our findings are comparable with other studies,[8,11] which show female preponderance in meningioma. Spinal meningiomas are mostly IDEM; psammoma bodies are seen in almost all meningiomas. A psammomatous variant is more common in the spine and most have the benign course but can lead to pressure effects and segmental neurologic deficits.[14] Astrocytoma [Figure 2a] and ependymoma represent the most common intramedullary neoplasms. Astrocytoma is rare in the spine as compared to the cranial cavity where it is the most common primary malignancy. There were five cases of astrocytoma, out of which two were low-grade astrocytomas, two pilocytic astrocytomas, and one high-grade glioma. Pilocytic astrocytoma showed elongated eosinophilic structures called Rosenthal fibers [Figure 2b] and also eosinophilic granular bodies [Figure 2c]. Grading of astrocytoma was done according to the WHO central nervous system (CNS) Tumor Classification 2007. Grade I and II are low-grade lesions while Grade III and IV are high-grade lesions and have a poor prognosis. The majority of primary spinal cord tumors are classified as low grade (Grades I and II) according to the WHO CNS tumor classification.[5] There were three cases of metastatic adenocarcinoma. Metastasis constitutes the most common extradural tumor. The incidence is less as compared to other studies.[6] It may be due to the relative exclusion of bony metastasis not involving the cord in the present study. Metastatic deposits are most of the time solitary. In carcinomatosis, cord lesions are frequent but due to difficult access to the site, biopsy is obtained from other sites for diagnosis. Chordoma (3 cases) arises from notochordal remnants.[15] Grossly, it’s a lobulated and infiltrative lesion. Microscopy shows phenotypically mixed cells having mesenchymal and epithelial immunoreactivity. Epithelial cells arranged in cords and typical physaliphorous cells lying in the mucoid matrix are seen [Figure 3]. Sometimes it is difficult to differentiate it from chondrosarcoma. PNETs of the spine are rare. Most are secondary to metastatic spread through the subarachnoid space from a primary intracranial tumor. PNETs are aggressive embryonal tumors. Histologically, they are composed of small round undifferentiated cells. Occasional differentiation along neuronal or glial lines may be seen [Figure 4]. Origin of PNETs is thought to be from neoplastic transformation of primitive neuroepithelial cells in subependymal zones. Five cases were diagnosed as tuberculous inflammation. Mostly it is the extension of adjacent tuberculous inflammation from vertebrae, although it can be secondary to tuberculous meningitis. This leads to the destruction of cartilage and collapse of the intervertebral disc, sometimes forming cold abscess leading to pressure effect. In such cases, fine-needle aspiration may be equally effective for cytologic diagnosis and culture of organisms[16], but open biopsy definitely yields more tissue for confirmation of diagnosis on histopathology. Two cases of epidermoid cyst were diagnosed; one was intradural while other was intramedullary. Mostly, they are located intracranially. A rare intraspinal case report exists in world literature.[17] |
ConclusionTumors constitute the major part of spinal SOLs. Mostly, they are benign or low grade. All histopathological types, except meningioma, are more common in males as compared to females. Many times clinical and radiological features are suggestive of spinal cord tumor but on histology, it turns out to be inflammatory lesion and viz. Hence, tissue diagnosis is mandatory because of the wide variety of lesions in this area with differing prognosis and treatment modalities. The extent of surgical resection depends on the histology and location of the tumor. Though PNET is rare in the spine, it can be considered in the differential diagnosis of spinal tumors. Neuro-imaging technique and cytologic preparation have a complementary role in the rapid and accurate diagnosis of spinal lesions. |
Subscribe now for latest articles and news.