Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.007
Year: 2021, Volume: 7, Issue: 2, Pages: 39-42
Original Article
Ramesh Agrawal1 , Harshul Patidar2 , Ronak Jain3 , Pratik Akhani4
1 Assistant Professor, Department of Microbiology, Government Medical College, Khandwa, Madhya Pradesh, India,
2 Assistant Professor, Department of Pathology, Government Medical College, Khandwa, Madhya Pradesh, India,
3 Senior Resident, Department of Tuberculosis and Chest, Government Medical College, Ratlam, Madhya Pradesh, India,
4 Assistant Professor, Department of Physiology, Government Medical College, Khandwa, Madhya Pradesh, India
Address for correspondence:
Dr. Pratik Akhani, Assistant Professor, Department of Physiology, Government Medical College, Khandwa - 450 001, Madhya Pradesh, India. Phone: +91-9429665389. E-mail: [email protected]
Background: : Influenza is among the most important reasons of hospitalization and mortality in children. Compared to other age groups, children are excessively affected by influenza A (H1N1) pandemic. This study was planned to detect and study the clinical profile of H1N1 virus using real-time reverse transcriptase polymerase chain reaction (rRT-PCR) in pediatric patients.
Materials and Methods: The H1N1 virus was detected in nasopharyngeal or throat swabs in 510 children suspected with influenza such as illness, using rRT-PCR assays as recommended by the World Health Organization and Centers for Disease Control and Prevention protocol. Patients’ biodata and clinical history were recorded.
Results: Out of 510 suspected influenza cases, majority (61.9%) were males and of 1–5 years’ age (44.5%). H1N1 was positive in 100 (19.6%) cases. 6–10 years’ age group was most affected (24.1% H1N1 positive). Clinically, all children had flu-like illness
Conclusion: : The present study revealed that the 6–10 years’ age group children were highly susceptible to H1N1 infection. Therefore, early intervention results in good outcome in terms of reduced requirement of invasive ventilation and decreased mortality rate
KEY WORDS: : Child, H1N1 subtype, humans, influenza A virus, reverse transcriptase polymerase chain reaction, virus diseases.
Influenza is a very common, highly transmissible viral respiratory tract infection that usually causes yearly epidemics in most parts of the world with its peak prevalence being in winter.[1] The infection can present with a wide-ranging clinical features, from mild symptoms such as pyrexia, cough, and headache, to severe complications such as pneumonia, acute respiratory distress syndrome, or even death. Young children, elderly persons, immunocompromised patients, and pregnant females are more likely to develop such complications.[2] The novel influenza A (H1N1) Influenza virus caused a huge disease outbreak of swine flu in 2009 which was declared pandemic by the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC).[3] In India, Hyderabad was the first to report a laboratory-confirmed case of H1N1 on May 16, 2009, while Rajasthan, the largest state of India, reported its very first case on July 23, 2009.[4]
Children are the most susceptible population for Influenza and are most likely to transmit this infection. Especially the school going children aged 5–17 years are mainly affected during annual flu outbreaks.[5] Furthermore, highest deaths from Influenza are reported among children and elderly patients.[6] Influenza is commonly a vaccinepreventable viral infection. However, currently available vaccines induce only a short lived narrow immunological response.[7]
Influenza virus is an enveloped virus which contains a single-stranded ribonucleic acid (RNA) genome and belongs to the Orthomyxoviridae family of viruses. It displays not only genetic variations as a result of its segmented genome but also surface antigenic variation in both hemagglutinin and neuraminidase proteins. Hence, due to antigenic drifts and shifts, it can infect a wide range of hosts including humans, birds, domestic and wild animals and cause potential pandemics. Hence, this study was planned to detect and study the clinical profile of H1N1 virus using real-time reverse transcriptase polymerase chain reaction (rRT-PCR) in pediatric patients.
This study was done at virology research laboratory, Dr. Sampurnanand Medical College, Jodhpur, India, after ethical clearance from Institutional Ethics Committee. Children (1 month to 16 years) with suspected influenza-like illness were included in the study. Informed consent was obtained from parents/ legal guardians. Swabs were collected from throat and nasopharynx and sent to virology laboratory in a viral transport medium as per standard prevalent guidelines. Patients’ biodata and clinical history were also recorded.
The RT-PCR protocol was as per the WHO guidelines.[8] Sample processing was done in a negative pressure chamber Biosafety Cabinet as per the CDC standards.[9] RNA extraction was done from samples by column based RNA kit (QAIamp®, Germany). Primers and probes (Thermo Fisher Scientific, USA) were CDC approved. rRT-PCR machine (Applied Biosystems) was used with a PCR kit (2× master mix; Superscripts™ III enzyme mix; and primer-probe mix for H1N1). Template setup was done according to the PCR kit manufacturer’s (Applied Biosystems’) instructions.
Statistical analysis was performed using Microsoft Excel 2016 and SPSS® (Statistical Package for the Social Sciences) version 21.
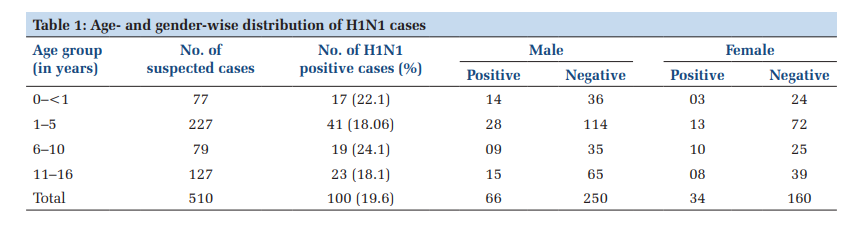
Out of 510 suspected cases of influenza reported during the study period, 100 (19.6%) were positive for H1N1. Among total cases majority (n = 316, 61.9%) were males whereas other were (n = 194, 38.1%) females.
Table 1 shows the age- and gender-wise distribution of H1N1 cases. Most of the suspected children were in the 1–5 years’ age group (n = 227, 44.5%) while the mean age was 5.94 years. Maximum percentage (n = 19, 24.1%) of H1N1 positive cases was observed in the 6–10 years of age group.
Geographically, the maximum number of cases was reported from Jodhpur, Western Rajasthan (57.25%). Details of geographical distribution are shown in Figure 1.
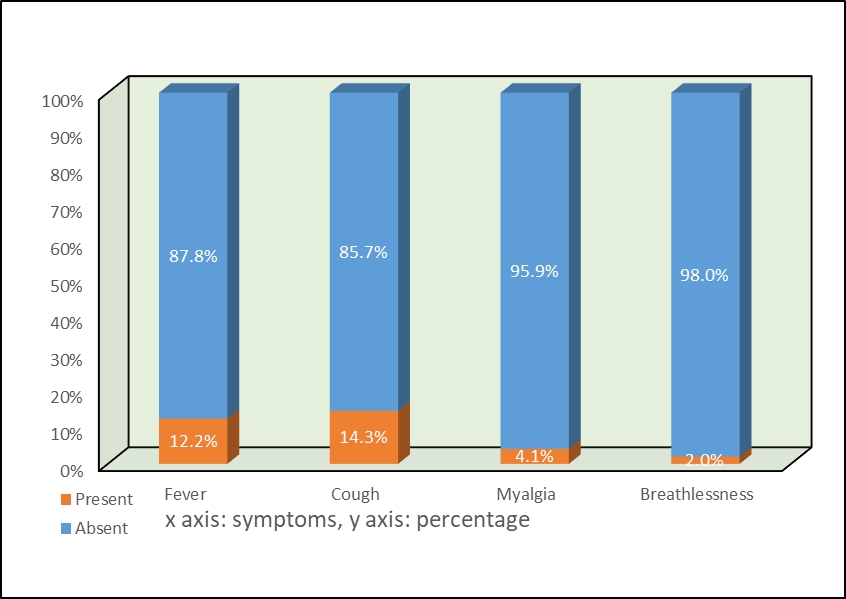
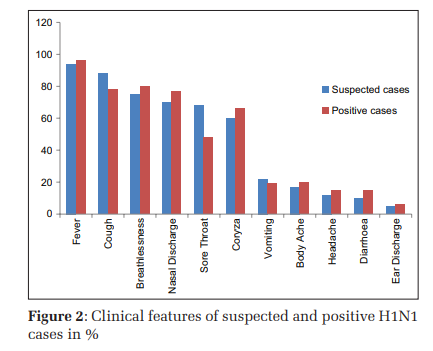
Following symptoms were observed in suspected patients in the decreasing order of frequency: Fever (94%), cough (88%), breathlessness (75%), nasal discharge (70%), sore throat (68%), coryza (60%), vomiting (22%) body ache (17%), headache (12%), and diarrhea (10%), and ear discharge (5%). In contrast, nasal discharge and cough were prominent in positive influenza cases. Following symptoms were observed in positive H1N1 patients in decreasing order of frequency: Fever (96%), breathlessness (80%), cough (78%), nasal discharge (77%), coryza (66%), sore throat (48%), body ache (20%), vomiting (19%), headache (15%), diarrhea (15%), and ear discharge (6%).
Comparison of clinical features of suspected and H1N1 positive patients is shown in Figure 2.
Influenza still remains a common cause of respiratory tract infection which seriously threatens pediatric health. While most children show mild illness with flu-like symptoms, some may develop severe pneumonia and/or neurological problems that can be fatal. So early identification of influenza virus is of paramount importance to minimize child mortality. In our study 19.6% os suspected children were found positive for H1N1 which was in accordance to Li et al. [10] and Tresoldi et al.,[11] while Mandal et al. [12] observed higher positivity rate (47.5%). We found that majority of patients (44.5%) were of 1–5 years’ age and were males; similar findings were reported by Pushpalatha et al. [13] and Mishra et al. [14] We observed that maximum H1N1 positivity (24.1%) was found in the 6–10 years of age group, presumably because they go to schools and hence have a transition in environmental exposure. Chaitanya et al. [15] showed highest H1N1 positivity (66.6%) in 1–6 years’ age groups of children.
Infantile infection by Influenza virus is usually more frequent in 6–12 months’ age group compared to 0–6 months of life, mainly because of circulating maternal influenza antibodies acquired either through placenta or breastfeeding.[16]
We observed that the foremost common clinical features of H1N1 Influenza were fever, cough, breathlessness, rhinorrhea, and coryza. Similar findings were suggested by Mehta et al. [17] and Prakash et al. [18] However, various studies have reported that amount of rainfall, relative humidity temperatures differences influence the Influenza outbreaks.[19]
We did not include neonates in our study as the sampling is difficult in this age group. As we used convenient sampling method, all the geographical areas could not be represented in our study population. We included only symptomatic cases; hence, asymptomatic carriers could not be detected.

The present study revealed that children belonging to 6–10 years’ age group were most vulnerable to H1N1 infection, and common symptoms were fever, cough, breathlessness, rhinorrhea, and coryza. Therefore, early interventions may result in better outcomes in terms of reduced requirement of invasive ventilation and decreased mortality rate. It is of great significance to develop strategies for the prevention and control of Influenza by measures such as social distancing, and educating school children about health and hand hygiene.
Subscribe now for latest articles and news.