Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i01.001
Year: 2017, Volume: 3, Issue: 1, Pages: 1-6
Original Article
Mela Danjin1, Nafisa Usman Umar2, Danladi Adamu3
1Head of Department, Department of Anatomy and Physiology, College of Nursing and Midwifery, Gombe, Nigeria,
2Student, College of Nursing and Midwifery, Gombe, Nigeria,
3Principal, School of Nursing and Midwifery Gombe, Nigeria
Address for correspondence:
Mela Danjin, Department of Anatomy and Physiology, College of Nursing and Midwifery, Gombe, Nigeria. Phone: +2348063583988. E-mail: [email protected]
Aim: This study sought to determine the prevalence of diabetes mellitus (DM) among adult patients attending Specialist Hospital Gombe, Northern Nigeria. Materials and Methods: A 5-year (2010-2014) retrospective descriptive survey of cases of DM was conducted, using hospital record retrieved from the record (Institution). Diagnosed adult cases of DM were carefully identified and sorted from the general outpatient department morbidity register. Relevant data were then harvested on a specially designed pro forma/data collection template.
Results: A total of 40,083 medical cases were counted out of which 2069 cases of DM were identified. This implies an overall prevalence rate of 5.16%. However, the yearly prevalence of the disease revealed as high as 12.55% in the year 2012 and a least value of 1.22% in the year 2010. Age-specific case count of the disease was found to be highest, 1288 (62.25%) within the highest age range of 65-75 while the lowest age range of 25-34 was least affected, 33 (1.60%). Overall, more females, 1491 (72.06%) suffered from the disease than males, 578 (27.94%). The sex difference was found to be significant (χ2 = 449.15521, P < 0.001). Furthermore, the case burden of the disease was found to be significantly (χ2 = 39.02524, P < 0.001) highest among individuals living in urban areas, 663 (80.38%) than those living in rural areas, 406 (19.62%).
Conclusion: The disproportionately high case burdens of DM among females, urban dwellers and the aged are useful information for the design of targeted diabetes prevention programs by government and other stakeholders.
KEY WORDS:Adult patients, diabetes, prevalence, retrospective.
In developing countries such as Nigeria, diabetes mellitus (DM), and other non-communicable diseases (NCDs) continue to exhibit the “slow epidemic” surge. Based on the 2013 IDF global diabetes scorecard, raw national diabetes prevalence for Nigeria was estimated at 4.99%.[1] The national figure for some other African countries was put at 3.58% for Kenya, 3.93% for Guinea, 3.35% for Ghana, and 1.55% for The Gambia. Ethiopia had 4.36%, DR Congo 5.37%, Rep of Congo 5.48%, and Cameroun 4.88%.[1] From Abeokuta, South Western Nigeria, an overall prevalence rate of 14.8% was reported.[2] When segregated by age group an increasing trend from 2.9% in the age group of 18-27 years to a peak of 21.1% in the age group of 48-57 years was observed. Omorogiuwa et al. in a survey carried out on a university community, Ekpoma, Edo State southern Nigeria; reported an overall prevalence of as high as 9.8%.[3] In Umudike, Abia State South Eastern Nigeria in a study among adult Nigerians 18 years and above, a prevalence rate of 3.0% with higher rates reported among females (3.6%) than males (2.3%) was published.[4] In another study, among adults aged 18 years and above residing in five rural communities in Edo state an overall crude prevalence of 4.6% with sex differences (males 1.9%, females 5.8%, P = 0.012) was reported.[5] The overall prevalence of as high as 10.5% with male and female rates of 9.6% and 11.2%, respectively, was reported in Uyo, South Southern Nigeria.[6]
In northern Nigeria, the prevalence and incidence surveys also indicate varying figures. A5-year (2001-2005) retrospective study of hospital records in Katsina was conducted in which among the 281 cases reported in the period, more males (201 [71.53%]) suffered from the disease than females (80 [28.47%]).[7]
Although this study did not aim to segregate DM cases by type, extent data from other African countries and Nigeria reveals that about 90% of cases are Type 2 DM while Type 1 DM ranges between 5.7% and 10.0% with the remaining 0.0-4.3% being gestational DM.[8-14]
Despite the fact that there is no published work, anecdotal evidence has indicated high burden of DM in the study area. A cursory look at the morbidity register of State Specialist Hospital Gombe would show that DM is a disease of public health importance in the area. Hence, this study was an attempt to document scientific evidence and quantification of the problem within Gombe metropolis. The study also sought to find out trend of DM case prevalence in retrospect (2010-2014) and its seasonal pattern of occurrence. Again, what were the age group, gender, and place of residence patterns of the disease distribution among the study population?
Study setting This survey was conducted in the State Specialist Hospital, domiciled within Gombe metropolis which is the state capital of Gombe state in northern Nigeria. The Metropolis lies between latitude 110°81 N and 110°241 N, longitude 110°021 E and 110°181 E. The temperature averages 30°C with an annual rainfall of 52 cm. The hospital is the only state government-owned tertiary health facility that is meant to cater for referral cases from other secondary (General Hospitals) and primary health facilities scattered over the 11 local governments of the state. Hence, to a large extent, the hospital patient demographics may be a fair reflection of the entire state. Some of the specialist units or departments include general outpatient department which serves as a filter where all cases are first seen, Paediatrics Department, a Standard Laboratory, Eye Clinic, Dental Clinic, Obstaetric and Gynaecology Department, Health Records Department, etc. Based on the Nigerian National Population Commission Census 2006 figures projected to 2014, Gombe state has an estimated total population of about three Million at an annual growth rate of 3.2%.[8] The metropolis has a projected population of 344,804 inhabitants.
Study design A retrospective descriptive survey of DM was conducted in specialist hospital where the records in the health record department of the hospital were retrieved, reviewed, and analyzed with the aim of determining overall prevalence of the disease as well as characterizing trends and patterns of its distribution based on some selected demographics of the patients.
Target population Inclusion criteria To be included in the survey, a case record must be that of an adult patient seen in the outpatient department of Specialist Hospital Gombe with medical diagnosisof DM within the period of 2010-2014; and must be within the age range of 25-74 years (well over 90% of all DM cases retrieved). The record of all other medical cases seen within the same period qualified for the overall all-cases count.
Exclusion criteria A case record will be excluded especially if patient was seen before the year 2010 or after the year 2014. Only very few diagnosed DM cases fell outside the age range of 25 and 75 years. For the general all- cases count cases outside the study period (2010- 2014) were excluded from the study.
Data collection The relevant hospital records of all medical cases including DM in the state (institute), from 2010 to 2014, were carefully sorted with the aim of investigating the prevalence of the DM in Gombe. A total of 40,083 medical cases were counted, out of which 2069 cases of DM were identified. The key variables on which data were collected include; number of all medical cases seen, number of cases of DM seen, age range, sex, place of residence, month and year.
A structured pro forma with columns under the aforementioned key variable headings was designed and used for the data collection on all identified diagnosed DM cases.
Data analysis The raw data were entered on Microsoft excel spreadsheet for preliminary analysis. Thereafter, it was exported to Epi Info 7 (CDC, Atlanta, GA, USA, 2011) for further analysis. Data were presented as frequency tables, bar charts, and graphs. Associations were tested using chi-square within 95% confidence interval (CI).
Ethical consideration Ethical clearance for this work was obtained from the Research and Ethics Committee of College of Nursing and Midwifery Gombe, while consent of relevant authorities of the hospital was properly secured.
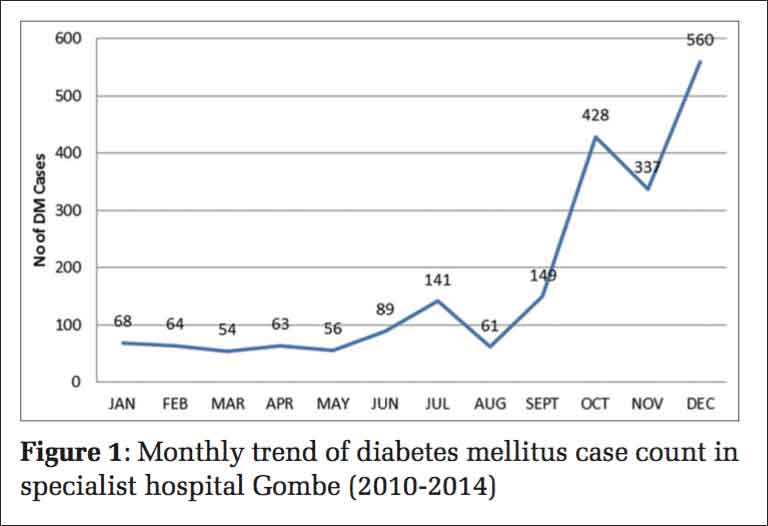
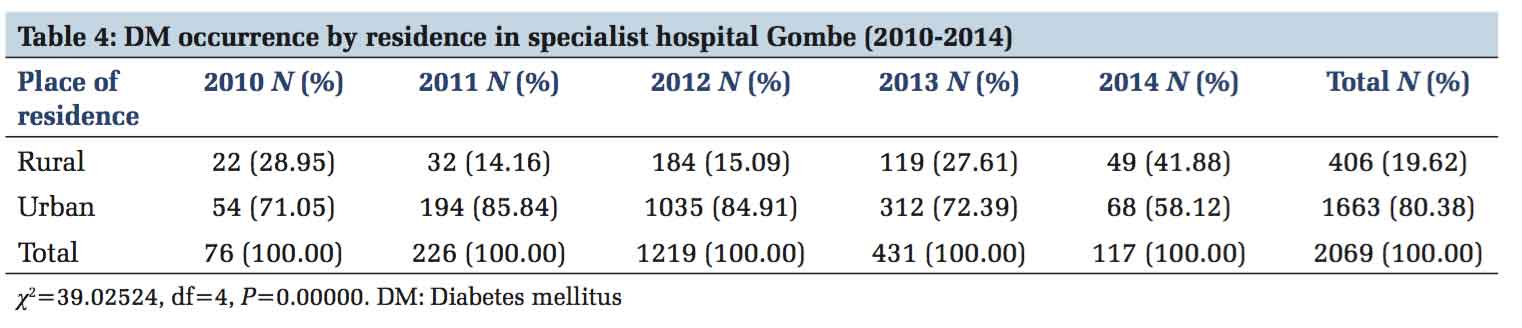
The results of this study showed a total number of all medical cases seen in the hospital within the study period (2010-2014) as 40,083 out of which 2069 were cases of DM (Table 1). This represented an overall DM prevalence of 5.16%. The yearly trend of DM prevalence is also shown in Table 1, 2010 (1.22%; 76/6212), 2011 (3.96%; 226/5704), 2012 (12.55%; 1219/9710), 2013 (3.33%; 431/12944), and 2014 (2. 12; 117/5513). Table 2 shows DM cases seen within the study period according to age group as, 25-34 (33; 1.60%), 35-44 (127; 6.14%), 45-54 (162; 7.83%), 55-64(459; 22.18%), and 65-75(1288; 62.25%). The increases in the disease burden with age was significant (χ2 = 24.5502, P = 0.000002). In Table 3, sex distribution of DM cases within the study period was shown with significant (χ2 = 449.15521, P = 0.00000) female majority, male (578; 27.94%) and female (1491; 72.06%). Figure 1 displays the cumulative monthly trend of the 2069 DM cases identified within the 5-year study period (2010-2014). The lowest case count (54) was in the month of March, while the three peaks were recorded in the months of July (141), October (428), and December (560). Table 4 shows DM case burden according to place of residence in which 80.38% (1663/2069) of the patients domiciled in urban areas while the remaining 19.62% (406/2069) resided in rural areas. This variation was quite significant with χ2 = 39.02524, P = 0.00000.
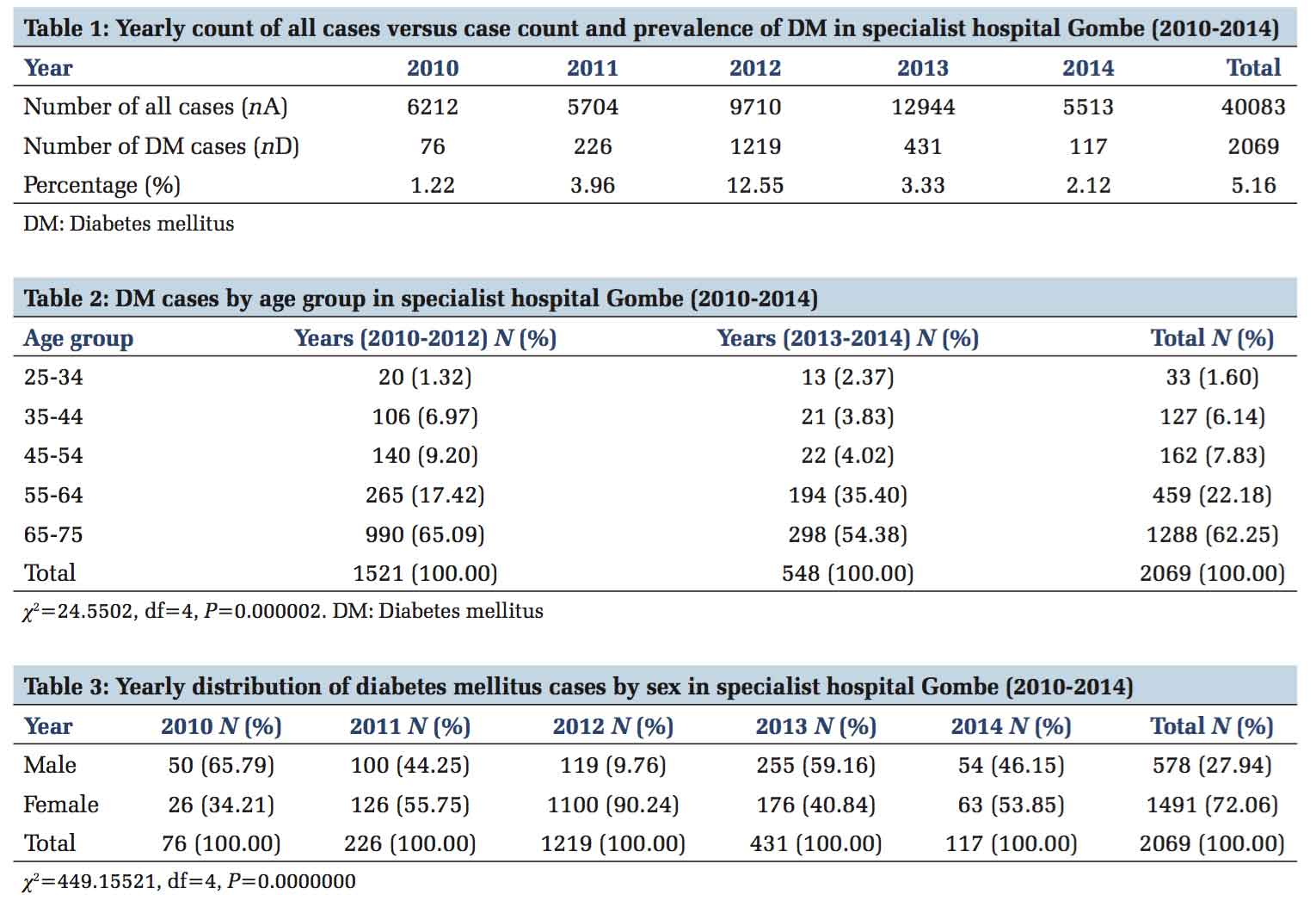
Overall and yearly prevalence of DM With a computed overall DM prevalence of 5.16% and a census population figure of Gombe state (3,028,459) cited in the study setting, we can say that there is an estimated population of not < 156,269 people in Gombe State that are suffering from the disease (Table 1). This rate appears to be on the high side compared to the Nigerian national prevalence rate of 4.99% according to the International Diabetes Federation (IDF).[1] When determined according to individual years covered in this study, there was a steep rise from an initial lowest rate of 1.22% in the year 2010 to 3.96% in 2011. This rising trend continued to a peak of 12.55% in the year 2012. This sharp rise in cases may have been occasioned by heightened sensitization activities by DM clubs and societies in the state at about the same period, thereby leaving the possibility of existence of an iceberg of non-reported cases of the disease in the hospital catchment communities. Thereafter, the disease prevalence nosedived to 3.33% in the year 2013 and finally to 2.12% in the year 2014. This picture contrasts with findings at global, regional and national levels where both developed and developing countries are experiencing an almost linear rising trend in the prevalence of diabetes, cardiovascular diseases, and other NCDs.[1,15] However, on the prevalence of diabetes in Nigeria, Oputa and Chinyere states in a review that, “The diabetes prevalence of 4.9% has more than doubled when compared with the 2.2% prevalence of the Professor Akinkugbe-led National Survey Report of 1997.”[16] Hence, the fluctuating trend observed in this study need to be further substantiated by other more rigorous studies in the study area.
Age pattern of DM occurrence When stratified by age group, this study established a consistently rising pattern of DM burden with age in which the oldest age group (65-75) was responsible for 62.25% of cases, while the lowest age rung (25-34) accounted for the smallest percentage (1.60%) of DM cases. The association between age and DM occurrence was found to be quite significant (χ2 = 24.5502, P = 0.000002). This concurs with findings of other studies from different parts of the world and within Nigeria.[10] In a study on Type 2 diabetes and its correlates among adults in Bangladesh, respondents within the age group of 55-59 years had higher odds of having diabetes (odds ratios = 2.37, 95% CI: 1.76- 3.21) than the age group of 35-39 years.[17] In a study in Uyo Southern Nigeria, subjects in the highest age group in the study (46-60) were about twice more likely to have diabetes than all the others in the lower age groups.[6] In another DM prevalence study in Port Harcourt, Southern Nigeria aging was also found to be associated with Type 2 diabetes.[9]
Sex distribution of DM cases When segregated by sex this study showed that more females were affected than males in a ratio of 2.58:1 (72.06%/27.94%) (Table3). This sex differential was found to be quite significant (χ2=449.15521, P=0.0000). This agrees with several other studies that revealed higher female ratio in different proportions. Findings from Port Harcourt by Tamunopriye and Iroro showed 70% females and 30% males with a male-female ratio of 1:2.3.[18] Uloko et al. reported from a multi-center study in Nigeria where out of a total of 531 DM patients, 209 (39.4%) were males and 322 (60.6%) were females.[19] From Enugu, Southern Nigeria Chukwu etal. reported a higher proportion or cases of DM among females (56.0%) than the males (44.0%).[20] However, there were reports of higher male prevalence even Nigeria. In a hospital-based retrospective survey in Katsina Northern Nigeria Suleiman and Abdulkarim recorded more males that suffered from the diseases (201, 71.53%) than females (80, 28.47%).[7] A report from Abeokuta, southern Nigeria states that “Male subjects had higher prevalence of diabetes (1.85%) than females with 1.19% prevalence.”[2] Omorogiuwa et al. also reported higher male prevalence ratio, “The male/ female diabetic ratio were 1.4:1 and 1.3:1 for senior staff and junior staff, respectively,” among university staff in Ekpoma southern Nigeria.[3] A sedentary lifestyle of women in this part of the country could be a possible explanation to our findings of a feminine preponderance of DM case burden. Men are adjudged to be more physically active than women, and this probably could enhance insulin sensitivity in the men than women. Ekpengyong et al. and Nyenwe et al. found physical inactivity to be significantly associated with the incidence of diabetes in their study.[6,9] The male preponderance in other studies may not reflect the real situation because the pattern of hospital medical admissions may also need to be examined in such studies. The male bias may, therefore, be related to cultural, geographic and socioeconomic factors rather than the gender-related prevalence of DM.[21]
Monthly trend of DM cases Cumulative monthly trend of cases within the study period (2010-2014) exhibited an overall rising pattern of DM case occurrence from January to December. Three remarkable peaks were recorded - in July (141 cases), October (428 cases) and December (560cases), while two troughs were observed in August (61 cases) and November (337 cases). October and December peaks were more pronounced, suggesting a seasonal predilection of DM case occurrence toward the end of raining season and the peak of harvest and festive period of the year. This tendency for having high reports of cases of the disease within these periods could be due to the high likelihood of locals breaching dietary control habits during festivities and harvest seasons when varieties of food abound. A seasonality of Type 1 diabetes has been reported in Tanzania, with most cases presenting between August and November.[22] From the University of Benin Teaching Hospital, Benin City, Nigeria, Edo et al. reported peak cases in July and December, with the highest in December.[23] In a 6 years study on, “Seasonal Incidence of DM in Tropical Africa” the peak months of presentation were August through to November, with the greatest number of patients presenting in September.[24] In a slightly varied scenario Tamunopriye and Iroro from Port Harcourt reported in their study that, “67% of patients were diagnosed in the rainy season.”[18]
Prevalence of DM by place of residence This study recorded more urban (1663, 80.38%) than rural (406, 19.62%) cases of DM. The differences were statistically significant (χ2 = 39.02524, P=0.00000). This agrees with the majority of findings at various levels. A retrospective hospital- based study in Katsina, Northern Nigeria, established an overwhelmingly higher case burden in the urban (82.56%) than rural (17.44%) areas.[7] In Lagos South Western Nigeria, Oguoma et al. also reported higher urban (5.4%) than rural (1.8%) prevalence figures of DM.[25] Moreover, the explanation to this discrepancy has consistently been fast changing lifestyle due to the overwhelming influence of westernization cum urbanization in most developing countries. “Urbanization tends to decrease physical activity as very little physical activity is required for daily living whereas rural populations rely on foot walk as transportation means and often have intense agricultural activities as their main occupation.”[11]
The findings of this study show clearly that the prevalence of DM in the study area is consistent with the national prevalence according to the IDF. However, the yearly trend which exhibited a sharp rise in the year 2012 and a nosedive thereafter might be indicative of some dramatic progress in the control efforts occasioned by massive media and community sensitization programs on appropriate lifestyle modifications. In any case, the disproportionate distribution of the disease burden with obvious bias toward females, urban dwellers and the aged are useful information for the design of more targeted prevention programs by the government and other stakeholders.
Subscribe now for latest articles and news.