Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.016
Year: 2021, Volume: 7, Issue: 2, Pages: 96-100
Original Article
Khaneja Poorna, Mohan Sneha, Sarwat Tarana, Dutta Renu
Department of Microbiology, School of Medical Sciences and Research, Sharda University, Greater Noida, Uttar Pradesh, India
Address for correspondence:
Poorna Khaneja, School of Medical Sciences and Research, Sharda University, Greater Noida, Uttar Pradesh, India. E-mail: [email protected]
Context: Cytomegalovirus (CMV) infection enhances hepatitis C virus (HCV) pathogenesis as it prevents the normal mechanisms which are responsible for HCV clearance, thus plays a key role in HCV persistence and pathogenicity.
Aims: An individual develops lifetime CMV (immunoglobulin G [IgG]) seropositivity, after primary infection after which CMV establishes latency with intermittent reactivation. Thus, the present study was undertaken to look for coinfection of CMV (IgG) in HCV seropositive cases in the hospital. Research Design: This cross-sectional study was conducted at the Department of Microbiology, SMSR, Sharda Hospital and University.
Methods and Materials: A total of 250 serum samples (age and sex matched) collected during the study period were divided into Group A (125 HCV seropositive) and Group B (125 HCV seronegative) which were tested for HCV antibody and anti-CMV IgG level. Statistical Analysis Used: The Chi-square test was used for assessing the two proportions. P < 0.05 was considered statistically significant. PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, USA) was used for analysis.
Results: Among 125 Group A samples (HCV seropositive), anti-CMV IgG seropositivity 110 (88%) subjects most commonly belonged to middle socioeconomic status 57 (51.8%). Among 125 Group B samples (HCV seronegative), anti-CMV IgG seropositivity 94 (75.2%) subjects most commonly belonged to low socioeconomic status 32 (57.1%). Subjects from both Groups A and B most commonly hailed from rural areas (64; 58.2% and 35; 62.5%). Diabetes was the most common associated risk factor in both Groups A and B (53% and 83.4%, respectively). Conclusion: A statistically significant association between CMV and HCV was observed in the present study and diabetes, liver inflammation, and tuberculosis were identified as associated risk factors. CMV is a preventable infection and appropriate preventive measures will help to reduce the morbidity rate.
KEY WORDS: Cytomegalovirus, enzyme-linked immunosorbent assay, hepatitis C virus, risk factors
Cytomegalovirus (CMV) is a ubiquitous virus that infects most humans at some time in their lifetime.[1] CMV is a human β herpesvirus with tropism for a wide range of cell types in which life long, persistent infection is established.[2] Hepatitis C virus (HCV) infection has a highly variable natural course and it ranges clinically from asymptomatic to fulminate and with regard to the status of infection from silent to self-limited to viremia.[3]
CMV (immunoglobulin G [IgG]) and HCV coinfection – CMV infection enhances HCV pathogenesis as it prevents the normal mechanisms which are responsible for HCV clearance, thus plays a key role in HCV persistence and pathogenicity.[4] An individual develops lifetime CMV (IgG) seropositivity, after primary infection after which CMV establishes latency with intermittent reactivation.[5] Reactivated latent infection is defined as (IgG) positivity and (immunoglobulin M [IgM]) negativity.[6] There is a paucity of literature on the detection of CMV (IgG) antibodies as an indicator of coinfection with HCV. Thus, the present study was undertaken to look for coinfection of CMV (IgG) in HCV seropositive cases in our hospital.
It was a cross-sectional study conducted at the Department of Microbiology and Sharda Hospital for 6 months (May 2019–October 2019). A total of 250 samples were included which were divided into two groups – Group A – HCV seropositive and Group B – HCV seronegative; 125 in each (age and sex matched each). The serum samples from the study population were tested for HCV antibodies using a commercially available 4th Generation HCV TRI-DOT kit (Diagnostic Enterprises. Plot No.: 26, Indl. Estate, Sector-1, Parwanoo – 173 220, [H.P.]). Both the groups were further tested for CMV IgG antibodies using ELISA (Calbiotech Inc., 1935 Cordell Ct., El Cajon, CA 92020) following the manufacturer’s instructions.
The Chi-square test was used for assessing the two proportions. P < 0.05 was considered statistically significant. PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, USA) was used for analysis.
The present study was conducted at the Department of Microbiology, School of Medical Sciences and Research, Sharda University, Sharda Hospital, Greater Noida, from May 1, 2019, to October 31, 2019. A total of 125 subjects were included in each of the two groups – Group A (HCV seropositive) and Group B (age and sex matched, HCV seronegative) subjects. Anti-CMV IgG was determined in the sera of both the groups which ranged from the age group of 18–85 years. The correlation of age and gender is demonstrated in Table 1.
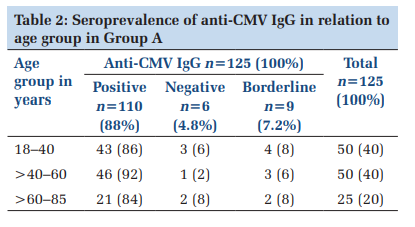
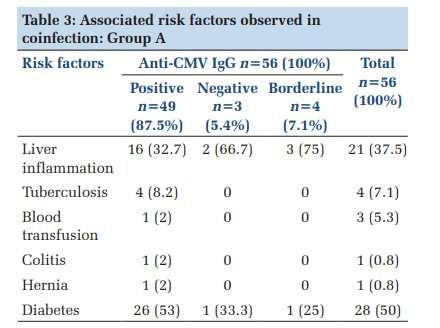
Among 125 Group A patients (HCV seropositive), 110 (88%) tested positive, 6 (4.8%) tested negative, and remaining 9 (7.2%) tested borderline for antiCMV IgG (Table 2). Anti-CMV IgG seropositivity was observed most commonly in females 67 (60.9%) as compared to males and the most commonly affected age group was 18–40 years 30 (44.8%) (P ≥ 0.05). Various associated risk factors such as diabetes, liver inflammation and tuberculosis were observed and are depicted in Table 3.
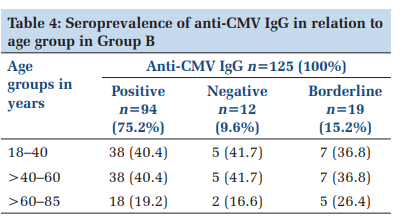
Among 125 Group B patients (HCV seronegative), 94 (75.2%) tested positive, 12 (9.6%) tested negative, and remaining 19 (15.2%) tested borderline for anti-CMV IgG (Table 4). Anti-CMV IgG seropositivity was observed most commonly in females 55 (58.5%) as compared to males and the most commonly affected age group was 18–40 years 26 (47.3%) (P ≤ 0.05). The associated risk factors observed were diabetes, liver inflammation, and tuberculosis, and are shown in Table 5.
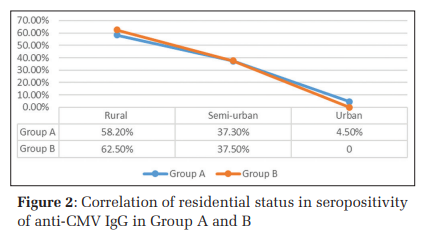
The correlation between socioeconomic status and residential status of anti-CMV IgG seropositivity of Groups A and B is shown in Figures 1 and 2, respectively.
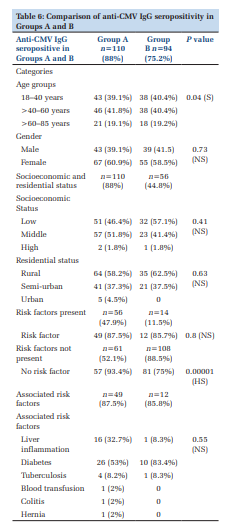
The various parameters of the patients who tested anti-CMV IgG seropositive in Groups A and B are summarized in Table 6.
In the present study, the anti-CMV IgG positivity rate among the HCV-infected patients (Group A) was 88% which was comparable to the previous studies.[2,6,7] The anti-CMV IgG prevalence in the general population (Group B) was 75.2% which was also comparable to the previous studies.[8-10] Looking at the age distribution of the anti-CMV IgG-positive cases in Group A, 46 (92%) cases were in the age group of >40–60 years, 43 (86%) cases were in the age group of 18–40 years, and 21 (84%) cases were in the age group of >60–85 years. The previous authors have also reported similar findings.[6,10] In Group B, the anti-CMV IgG seropositivity was similar in the age groups of 18–40 years and >40–60 years 38 (40.4% each, respectively) and 18 (19.2%) in the age group of >60–85 years. Other authors have reported a higher number of subjects testing seropositive in reproductive age groups. This difference may be because they have enrolled antenatal women.[11,12]
In the present study, we have observed that in the HCV seropositive (Group A) subjects, females were more anti-CMV IgG positive than males (67/110 [60.9%] and 43/110 [39.1%]), respectively. In a study done by Tabll et al. (2011), similar findings were reported.[7] In the HCV seronegative (Group B) subjects, 55/94 (58.5%) were female and 39/94 (41.5%) were male, that is, more number of females. Vaithegi et al. (2015) reported 83% of males and 80% of females which is not similar to the findings of this study.[12] The socioeconomic status among Group A says that the majority of the patients were in middle socioeconomic status 57(51.8%). This may be due to a large number of subjects from that status in this study. Among Group B subjects, 32 (57.1%) subjects were in low socioeconomic status, 23 (41.4%) in middle socioeconomic status, and 1 (1.8%) in high socioeconomic status. Similar findings were reported by the previous studies by Swanson EC and Jin Q.[13,14]
The residential status in the Group A subjects is distributed in rural 64 (58.2%), semi-urban 41 (37.3%), and urban 5 (4.5%). None of the previous studies have reported the residential status among anti-CMV IgG seropositive subjects. In the Group B subjects, 62.8% seropositivity for anti-CMV IgG was observed in rural areas, 37.5% in semiurban areas, and none of them reside in urban areas. Higher prevalence was reported by Jin (2017), from urban areas (93.8%) and downtown areas (95.7%),[14] whereas Vilibic et al. (2017) reported no difference in the participants residing in urban (74.4%) and suburban/rural regions (74.3%).[8]
Comparing the presence and absence of associated risk factors in both Groups A and B, 49/56 (87.5%) anti-CMV IgG seropositive subjects were having the associated risk factors and 57/61 (93.4%) anti-CMV IgG seropositive subjects did not show any associated risk factor in Group A. In Group B, 12/14 (85.7%) subjects show the presence of associated risk factors and 81/108 (81%) subjects had no associated risk factor in them. Moreover, the difference was statistically highly significant.
In this study, the identified associated risk factors in HCV seropositive subjects were diabetes 53% followed by liver inflammation 32.7% and tuberculosis 8.2%. In HCV seronegative subjects, diabetes was found in 83.4% of subjects and liver inflammation and tuberculosis were seen in 1 patient each (8.3%). The previous studies have not identified any associated risk factors. Thus, we can say that diabetes and liver inflammation are the most commonly found associated risk factor among the anti-CMV IgG seropositive patients.
The coinfection of HCV and CMV increases the morbidity rate. Detection of CMV becomes important in preventing infection in HCV patients. One of the most common and sensitive tools is ELISA but for more specific results, molecular methods should be used as they are more confirmatory. This was a limiting factor in this study. The study can be further extended by testing the samples through molecular techniques.



Few studies have been conducted in India and this is the first study in this region to examine the coinfection of CMV and HCV. A statistically significant association between CMV and HCV was observed in the present study and diabetes, liver inflammation, and tuberculosis were identified as associated risk factors.
CMV is a preventable infection and appropriate preventive measures will help to reduce the morbidity rate. CMV infection promotes HCV pathogenesis by the prohibition of the normal mechanism responsible for HCV elimination. A better understanding of HCV and CMV coinfection would lead to better management strategies for HCV-infected individuals.
Subscribe now for latest articles and news.