Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i02.004
Year: 2015, Volume: 1, Issue: 2, Pages: 19-24
Original Article
Feroza Sultana1, Raja Parthiban2, Shameem Shariff3
1Intern, Department of Obstretics & Gynaecology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka,India,
2Professor, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India,
3Professor & Head, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India
Address for correspondence:
Dr. Raja Parthiban, Department of Pathology, MVJ Medical College & Research Hospital, Hoskote, Bengaluru - 562 114, Karnataka,
India. E-mail: [email protected]
Background: Pregnancy induced hypertension (PIH) is one of the most common causes of both maternal and neonatal morbidity. A variety of hematological abnormalities may occur in women with PIH of which thrombocytopenia is the most common.
Objectives: This study was done to estimate the incidence of thrombocytopenia in pregnant women diagnosed with PIH and to correlate the severity of PIH with the degree of thrombocytopenia. Materials and Methods: 2 years retrospective study on 100 pregnant women admitted in MVJMC and RH with a diagnosis of PIH from January 2012 to January 2014. Data from case files were collected, compiled, and analyzed. PIH cases were classified into: (1) Gestational hypertension (HTN), (2) mild preeclampsia, (3) severe preeclampsia, (4) eclampsia, (5) hemolysis, elevated liver enzyme levels, and low platelet levels (HELLP) syndrome. The incidence and severity of thrombocytopenia along with maternal and fetal complications encountered in the five groups were analyzed.
Results: Preeclampsia - mild (56%) and severe (36%), accounted for most of the cases followed by eclampsia (6%) and gestational HTN (2%). In the 100 cases, mild thrombocytopenia (41%), moderate thrombocytopenia (29%), severe thrombocytopenia (6%), and normal platelet counts (24%) were encountered. Varying platelet levels were seen in the five groups with 23.4% of severe eclampsia and 50% of eclampsia cases having normal platelet counts and 7.1% of mild preeclampsia cases showing severe thrombocytopenia. Poor maternal outcome was seen 11% cases due to HELLP syndrome, postpartum hemorrhage, and maternal death. Poor fetal outcome was seen in 18% cases due to intrauterine growth restriction and perinatal mortality.
Conclusion: Platelet count alone cannot be relied upon to assess the severity of PIH. The search for a simple cost effective test for prompt management and prevention of maternal and neonatal morbidity performable in a rural hospital set up still continues.
KEY WORDS: Eclampsia, preeclampsia thrombocytopenia, pregnancy induced hypertension, outcome
IntroductionPreeclampsia thrombocytopenia (PIH) is defined as hypertension (HTN) that occurs in pregnancy for the first time after 20 weeks of gestation, disappearing following delivery of the baby.[1] PIH is the most common medical disorder of pregnancy, that leads to a complicated multi-organ failure in the mother. It is one of the most common causes of both maternal and neonatal morbidity.[2] It is a global problem and complicates approximately 10-17% of pregnancies. The incidence of PIH in India ranges from 5% to 15%.[3] Hemorrhage occupies is an important factor in the etiology of maternal mortality and therefore, remains a major problem.[4] Currently, there is no screening test that would help in identifying which pregnancy will be associated with PIH or assess its severity.[5] A variety of hematological abnormalities may occur in women with PIH[6] of which thrombocytopenia is the most common.[5,7,8] Some investigators have proposed biochemical markers to predict the severity of PIH like Placental tissue protein 13 and Endoglin’s; but these tests cannot be used for simple, low-cost screening. Therefore, there is a need to identify a simple test specifically designed for routine use in a hospital environment[9] in particular those suitable at a rural setup. This study was done to estimate the incidence of thrombocytopenia in pregnant women diagnosed with PIH and to correlate the severity of PIH with the degree of thrombocytopenia.
Materials and MethodsThis retrospective study was carried out following approval by the Institutional Ethics Committee on 100 pregnant women who had been admitted to the labor and maternity wards of MVJMC and RH with a diagnosis of PIH over a period of 2 years from January 2012 to January 2014.
Relevant data were obtained from case files and compiled by a common proforma that included socio-demographic characteristics of mothers, obstetric history, signs and symptoms in mother at presentation, laboratory data, and maternal and perinatal outcomes. The data collection was followed by analysis of the collected data. Any illness in the mother like chronic HTN or illness likely to cause changes in the platelet counts like connective tissue diseases, and those who received drugs like aspirin were excluded from the study. Only cases where the blood pressure (BP) and platelet counts that were seen to be consistently abnormal even on retesting following an interval of 6 h and no more than 1 week apart, as observed in the case files were included in the study. Based on the criteria described by the National High BP Education Working Group in 2000, the PIH cases in our study were classified into five groups as described by Wolde et al.[10] into: i. Gestational HTN: Systolic BP ≥140 or diastolic BP ≥90 mm Hg for first time during pregnancy with no proteinuria and BP returned to normal before 12 weeks postpartum • Evidence of hemolysis on peripheral smear, • Serum glutamic oxaloacetic transaminase >72 IU/L, • Total bilirubin >1.2 mg/dl, • Lactate dehydrogenase level >600 mg/dl, and • Platelet count < 100,000/ml. Thrombocytopenia was classified as mild when platelet count was found to be 1-1.5 lakh/cumm, moderate at 50,000-1 lakh/cumm and severe with < 50000/cumm.[11] Platelet counts had been estimated in EDTA anticoagulated blood by SYSMEX KX21 hematology 3 part analyzer. In patients with very low platelet count, the counts had been rechecked by peripheral smear examination. The patient files were analyzed to look for any maternal or neonatal complications. 
|
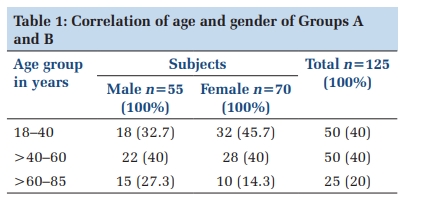
ResultsThe present study included 100 cases of PIH of which 2% were diagnosed with gestational HTN, 56% with mild preeclampsia, 36% severe preeclampsia, and 6% had eclampsia. Six cases of 36 cases of severe preeclampsia had features of HELLP syndrome. The cases ranged from 18 to 32 years of age with a mean age of 22 years (Table 1). Case of preeclampsia, eclampsia, and HELLP syndrome were found to be more common in the primigravida patients (67%), while gestational HTN was seen only in multiparous patients (Table 2). Of the 100 PIH cases, 24 cases showed normal platelet count and 76 cases showed deranged platelet count. Mild thrombocytopenia was seen in 41%, moderate thrombocytopenia was seen in 29% and severe thrombocytopenia was seen in 6%. In the 2 cases of gestational HTN, 1 case (50%) had mild thrombocytopenia while the other had a normal platelet count. In the 56 cases of mild preeclampsia, 43 cases (76.8%) had thrombocytopenia while the rest (23.2%) had normal platelet counts. Of these 56 cases, 29 cases (51.8%) showed mild thrombocytopenia, 10 (17.9%) showed moderate thrombocytopenia, and 4 (7.1%) cases had severe thrombocytopenia. In the 30 cases of severe preeclampsia, 23 cases (76.6%) had thrombocytopenia while the rest (23.4%) had normal platelet counts. Of these 30 cases, 8 cases (26.6%) showed mild thrombocytopenia, 15 (50%) showed moderate thrombocytopenia, and none had severe thrombocytopenia. Six cases of severe preeclampsia manifested with findings of HELLP syndrome and all had thrombocytopenia. Of these 6 cases 2 cases (33.3%) showed mild thrombocytopenia, 3 (50%) showed moderate thrombocytopenia, and 1 (16.7%) had severe thrombocytopenia. In the 6 cases of eclampsia, 3 cases (50%) had thrombocytopenia while the rest (50%) had normal platelet counts. Of these 6 cases, 1 case each (16.7%) showed mild, moderate, and severe thrombocytopenia (Table 3). In the various types of PIH, 11% of cases showed poor maternal outcome and 18% cases showed poor fetal outcome. Maternal complications were only seen in eclampsia (4/6 cases, 66.7%) and severe preeclampsia cases (7/36 cases, 19.4%). Of maternal complications there was one maternal death following development of disseminated intravascular coagulation (DIC) (1/6 cases 16.7%) and 3 cases (50%) with postpartum hemorrhage (PPH) in the 6 cases of eclampsia. Six cases of severe preeclampsia had features of HELLP syndrome (16.7%) and one case had PPH (2.8%). There were no maternal complications observed in the gestational and mild preeclampsia cases. An incidence of 18% fetal complications were observed in which perinatal mortality was seen in 2 cases belonging to eclampsia group followed by 10 cases and 6 cases of intrauterine growth restriction Journal of Medical Sciences and Health/May-Aug 2015/Volume 1/Issue 2 22 (IUGR) in the severe and mild preeclampsia group. None of the cases with gestational HTN showed any fetal complications. |
DiscussionOne of the most common medical complications of pregnancy is PIH; generally more common in the developing countries than in the developed countries.[10,12] Risk factors like extreme age, nulliparity, and race have been documented to be associated with this condition by various studies.[10] In a study from Ethiopia 66.7% of cases with PIH studied by Wolde et al.[10] were nulliparous that is similar to our study where 63% of cases were primigravida and studies by Riaz where 60% of the cases were primigravida.[13] More severe forms of PIH were found to be more common in nulliparous ladies as seen in our study. The preponderance of primigravida cases accounts for the young age group of the present study group. Similar findings have been observed by Vinodhini and Kumari[14] (24‑29 years) and Meshram et al.[5] (mean age of patients with preeclampsia 24.55 years and eclampsia 24.30 years). Annually around 1 lakh women die worldwide due to eclampsia with an estimated rate of one death every 3 min worldwide caused by preeclampsia and eclampsia. Preeclampsia causes poor maternal and fetal outcomes having a predictable onset and progression that may be cured by termination of pregnancy.[5] In India, PIH continues to be responsible for the largest proportion of perinatal deaths resulting from prematurity and IUGR; and is a major contributor to perinatal mortality. Though most of these conditions can be prevented, or identified and treated early by good antenatal care; the situation is still not very bright in rural India.[5] Various systems of classifications are noted in literature with modifications being made constantly[14] making comparison difficult. Bangal et al.[15] excluded gestational HTN and clubbed mild and severe PIH. While Mohammed et al.[16] have studied the variations of platelet indices in PIH in a fixed study group of 20 cases each under each category, whereby the incidence of each cannot be commented upon and Parmar et al.[12] have categorized PIH cases into mild, moderate and severe PIH. Wolde et al.’s[10] method to categorize cases with PIH based on the National High BP Education Working Group (2000) criteria has been done in this study owing to feasibility and simplicity of categorization into the five mentioned groups. In a study from Bhopal by Anand and Kirshnanand et al.,[3] majority of the cases had preeclampsia (66.36%) and the rest eclampsia (33.64%). Wolde et al.’s[10] study showed preeclampsia as the most common hypertensive disorder of pregnancy (51.9%); followed by eclampsia (23.4%), HELLP syndrome (8.9%), mild preeclampsia (7.6%), and simple gestational HTN (5.1%). In our study, most cases belonged to the mild preeclampsia (56%) group followed by cases with severe preeclampsia (30%). The incidence of eclampsia however was much lower in our study (6%). These differences could be due to small sample size of our study and the social ethnic and cultural difference in group of population studied as noted by Wolde et al.[10] who has quoted black race as one of the risk factors for PIH. It has been shown by earlier researchers that hematological aberrations such as thrombocytopenia and reduction in some plasma clotting factors may develop in preeclampsia women.[17,18] A transient mild thrombocytopenia is seen due to increased platelet consumption during pregnancy. Thrombocytopenia is found in approximately 6% of pregnancies and most common cause of thrombocytopenia in pregnancy is preeclampsia and eclampsia. A continuous decline in platelet count as pregnancy advances was shown by Fay et al. in 198319 and Shah A R et al in 201320. indicated that there is possibility of platelet hyper destruction during pregnancy. This together with hemodilution and platelet trapping results in decreased platelet.[8] McCrae[22] has suggested that thrombocytopenia may precede the various other manifestations of preeclampsia, and thus should be considered in the event of isolated thrombocytopenia seen in the late second or third trimester. Some authors have suggested that thrombocytopenia is caused due to peripheral consumption, endothelial damage, and reduced life span. Altered platelet membrane with accelerated aggregation and destruction have also been suggested.[8] Meshram et al.[5] in an hospital based study found lower platelet counts in preeclampsia and eclampsia that in healthy pregnant controls. Low platelet count was seen in 29.31% of cases with preeclampsia and in 44.44% of cases with eclampsia. Studies by Khan A et al. from Pakistan found a fall in platelet counts in cases with PIH. The authors in their study have documented similar findings from India by Annam V et al. and Turkey by Yaprak EU et al.23 In our study though thrombocytopenia was a consistent finding, a systematic fall in platelet counts in relation to the severity of PIH however was not noted, with 50% in cases with milder form of disease i.e. gestational HTN and 50% in severe form of disease i.e. eclampsia, showing normal platelet counts. Majority of cases with preeclampsia had thrombocytopenia and all cases complicated with HELLP syndrome had thrombocytopenia. Hence though thrombocytopenia may help in identifying progression of disease, but its absence does not rule out a severe disease. Hence, an overall consideration of various laboratory tests than just one test has been made obvious. In the present study, the incidence of HELLP syndrome was 6%, the values of present study are consistent with that of Riaz et al.[13] who reported an incidence of 5%. Meshram et al reported an incidence of 10.63% and in their study documented similar findings by Sibai et al. 9.8% and J Prakash et al. findings of 2-12%. 5 The incidence of maternal mortality in our study was 1% which well co-relates with that conducted by Shazia Riaz et al.13 1% and Meshram et al. 2.12%.5 Studies by Odegard et al. have shown pregnancies complicated by severe preeclampsia to have infants born with low birth weights; being around 12% below than expected, while pregnancies with mild preeclampsia showing no significant difference from expected range.[24] The “Born Too Soon” report by Raina and Mehta[25] provides estimates for global comparisons. According to this report, annually 15 million babies are born before 37 weeks gestation with one of the causes being PIH. In our study the incidence of IUGR in preeclamptic patients was found to be 16% which was comparable to Ludec et al. (21%) and Samantha et al. (15.5%) and Meshram et al. (19.14%).[5] The incidence of PPH as a complication in PIH was found to be 4% in our study. The incidence rate is lesser than those observed by Meshram et al. (8.5%) and Ludec et al. (10.20%). Similarly, the incidence of DIC has been reported as 3.19% by Meshram et al. and 3% by Ludec et al. (1992) as to 1% noted in our study.[5] These differences could stem from the variations in therapeutic strategies at an individual level down to an Institutional level and to the possible genetic factors that may have a role in affecting progression of disease or help in an adaptive response preventing complications. |
ConclusionPlatelet count is a simple, low cost, and rapid routine screening test. Varied conclusions have been drawn linking platelet count to severity of PIH. As a normal count does not rule out a severe disease our study shows that platelet count alone cannot be relied upon to assess the severity of PIH. Uniformity in utilization of classification and categorization of cases with PIH is also needed for better understanding of the disease process. The search for one marker that would identify and gauge the severity of PIH still continues. |
Subscribe now for latest articles and news.