Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i02.007
Year: 2017, Volume: 3, Issue: 2, Pages: 27-28
Review Article
Perikal J Parichay1, Kiran Khanapure2, T J Aniruddha3, J V Mahendra4, Krishna C Joshi5, Sunil V Furtado3, A S Hegde2
1Senior Resident, Department of Neurosurgery, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India,
2Professor, Department of Neurosurgery, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India,
3Associate Professor, Department of Neurosurgery, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India,
4Associate Professor, Department of Neurology, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India,
5Assistant Professor, Department of Neurology, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India
Address for correspondence:
Dr. Perikal J Parichay, Department of Neurosurgery, Ramaiah Institute of Neurosciences, Ramaiah Medical College, Bengaluru, Karnataka, India. Phone: +91-9886778242. E-mail: [email protected]
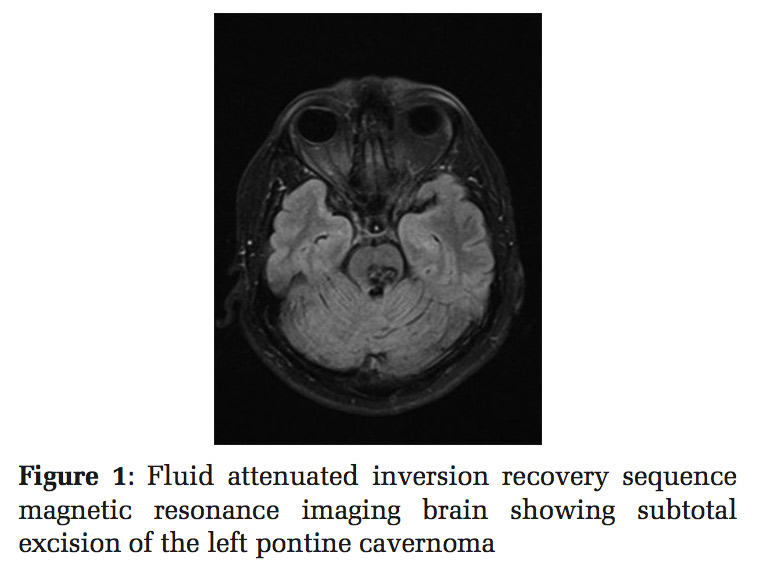
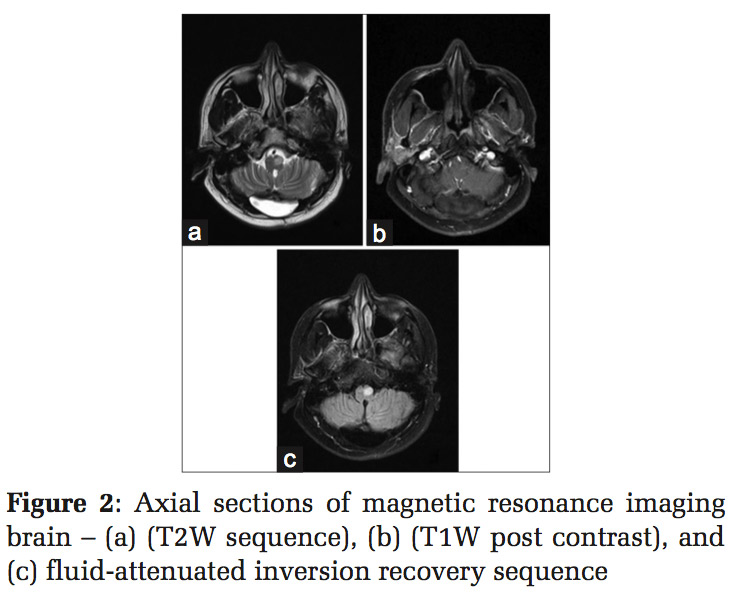
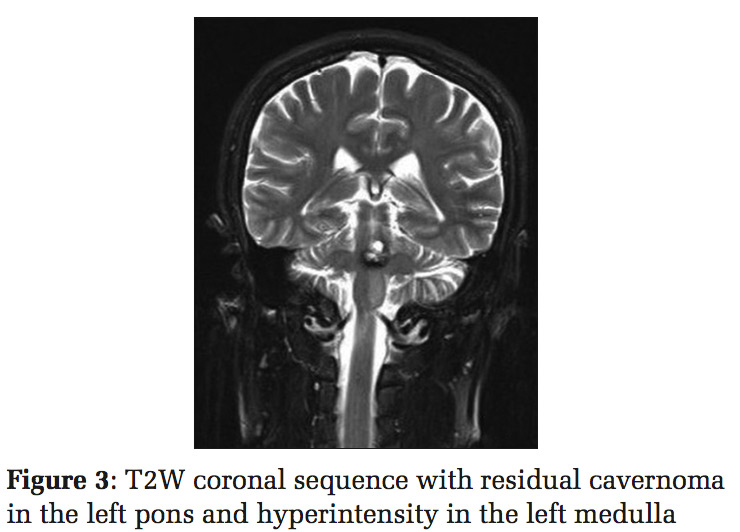
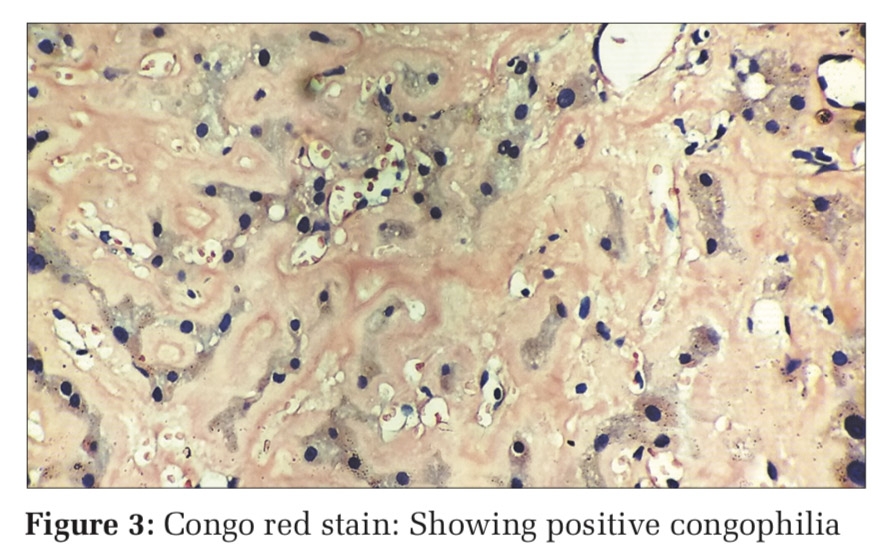
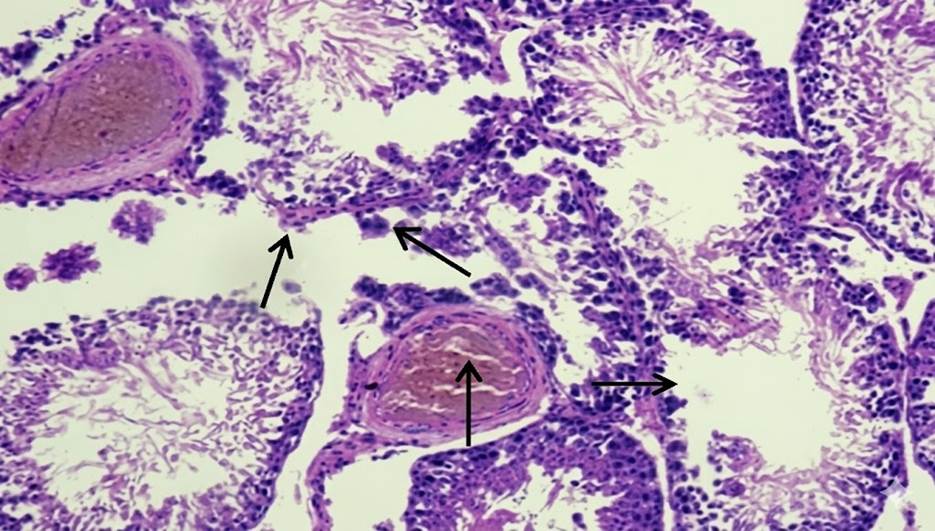
QuestionA 36-year-old gentleman, presented with right hemiparesis and internuclear ophthalmoplegia, was operated for left pontine cavernoma [Figure 1]. He followed up in outpatient department with gradual onset of palatal myoclonus 13 months post-surgery post-surgery [Figure 2 and 3]. Patient was evaluated with magnetic resonance imaging (MRI) brain which showed the above findings. Can you the guess the sequelae of pontine surgery in this patient? For answer turn to next page.
|
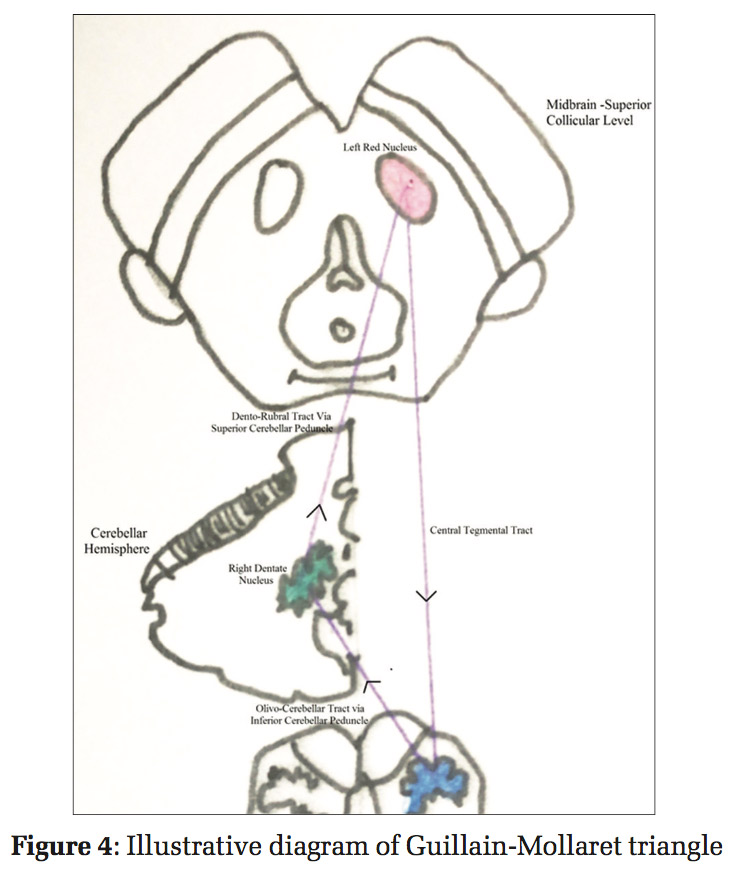
AnswerLeft sided hypertrophic olivary degeneration (HOD).ExplanationThe patient was evaluated with MRI brain which showed a hyperintensity in the left inferior olivary nucleus (ION). With a precedent history of brainstem surgery, a rare manifestation of pathology in the Guillain-Mollaret triangle causing HOD was ascertained. Figure 4 depicts the Guillain-Mollaret triangle and its connections.[1,2] With unilateral hypertrophy of ION, pathology is either in the red nucleus or the central tegmental tract (CTT). In this case, it is more likely the CTT on the left side is affected following the surgery Figure 4: Illustrative diagram of Guillain-Mollaret triangle of the left pontine lesion.[3] There is transsynaptic transneuronal degeneration of the left ION. This degeneration is unique as it causes hypertrophy of the ION rather than atrophy. Focal signal changes seen in the inferior medulla are not pathognomonic for HOD. Non-enhancement on contrast MRI differentiates it from other likely causes such as infarction, demyelinating disease, malignancy, infections, and inflammatory processes could also produce similar signal changes.[3,4] Symptomatic patients are difficult to treat and rarely resolve, but successful management of symptoms with benzodiazepines and carbamazepine has been reported. |
Subscribe now for latest articles and news.