Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i02.007
Year: 2020, Volume: 6, Issue: 2, Pages: 36-42
Original Article
inu Rose Mani1, Avita Rose Johnson2, Joselin Joseph3, S Jyothis3, Lijo Joseph3, Rigile P Cleetus3, T Sulekha4
1 Postgraduate student 2. Assistant Professor, 3.Intern. 4. Professor, Department of Community Health, St. John’s Medical College, Bengaluru, Karnataka, India
Address for correspondence:
Dr. Sulekha T, Department of Community Health, St. John’s Medical College, Sarjapur Road, Bangalore-34, Karnataka, India. Phone: +91-9844476638. E-mail: [email protected]
Introduction: The mother and child protection card (MCP card) have been developed as a tool to learn, understand, and follow positive practices for achieving good health of pregnant women, young mothers, and children.
Objectives: The objectives of the study were to assess the level of knowledge regarding pregnancy and child health care among mothers in possession of MCP card.
Materials and Methods:This was a cross-sectional study done among pregnant and post-natal mothers availing health services in a rural maternity hospital in Karnataka, using a structured interview schedule, capturing socio-demographic details and knowledge regarding pregnancy care, danger signs, infant care, institutional delivery, benefit schemes, and family planning based on information provided by MCP card. Each correct response was awarded a score of one, giving a maximum possible knowledge score of 71. Independent t-test, one-way ANOVA, and Pearson’s correlation were used to find association between total knowledge score and different socio-demographic variables.
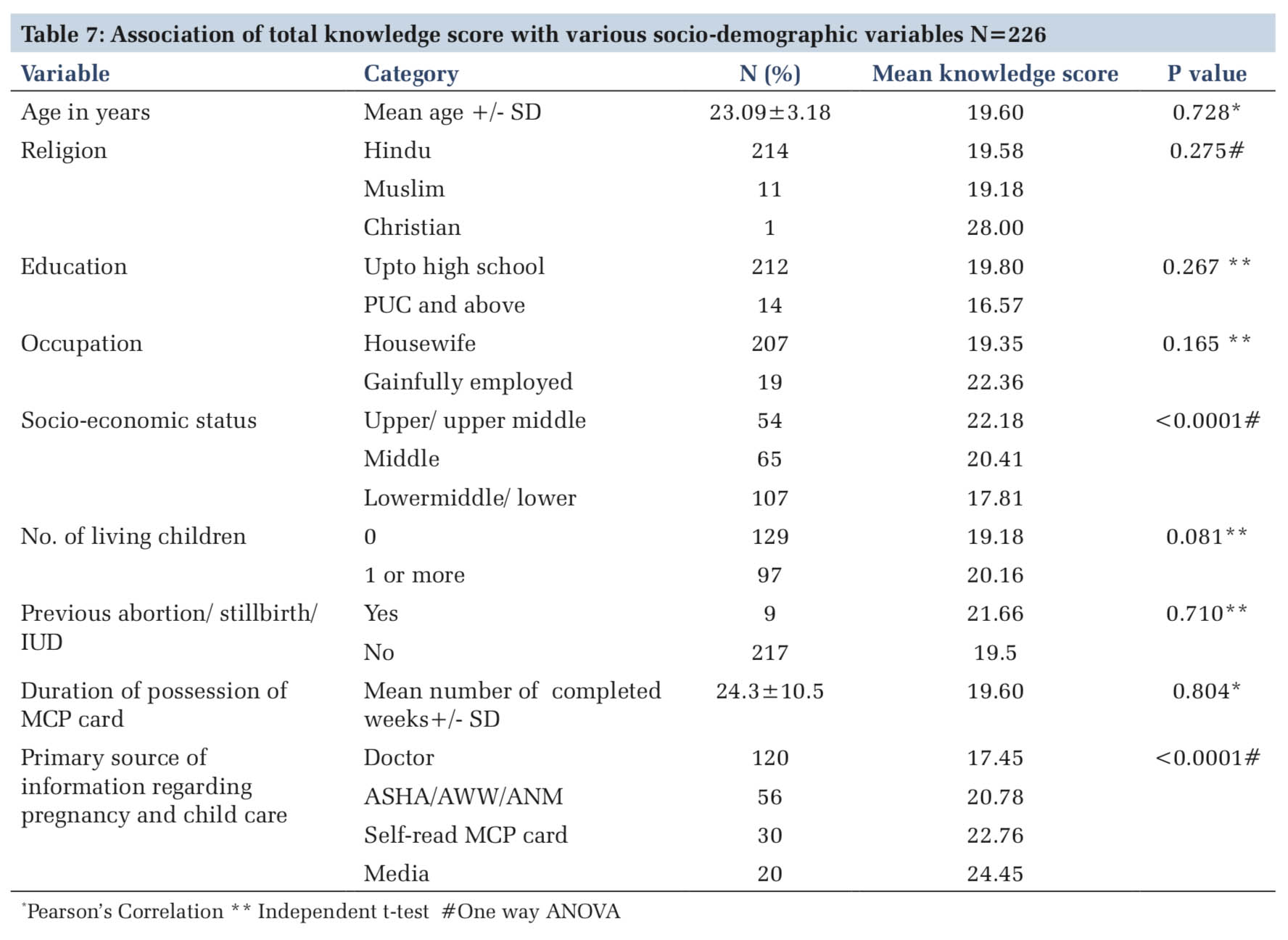
Results:Of the 226 participants, all had MCP card, but only 13.3% mothers had read the MCP card. The overall mean knowledge score of the participants was 19.6 ± 5.5 and median knowledge score was 19.0 (IQR=16, 23). All the women in our study were found to have poor knowledge as none of the subjects had a knowledge score of 35 or above. Higher socio-economic status of the mother was significantly associated with higher mean knowledge score regarding pregnancy and child care (P < 0.0001). The mean knowledge score was higher among women who said that their primary source was village level workers (ASHA/AWW/ ANM), media, and self-reading the MCP card (P < 0.0001), as compared to doctor.
Conclusion: This study has shown that in spite of MCP card having being developed as a tool for health education, maternal awareness remains poor among the mothers in possession of an MCP card. There is a need for re-enforcing among village level and primary healthcare workers that the MCP is an excellent resource for transferring knowledge regarding pregnancy and child care to rural mothers.
KEY WORDS:Child health, mother and child protection card, pregnancy.
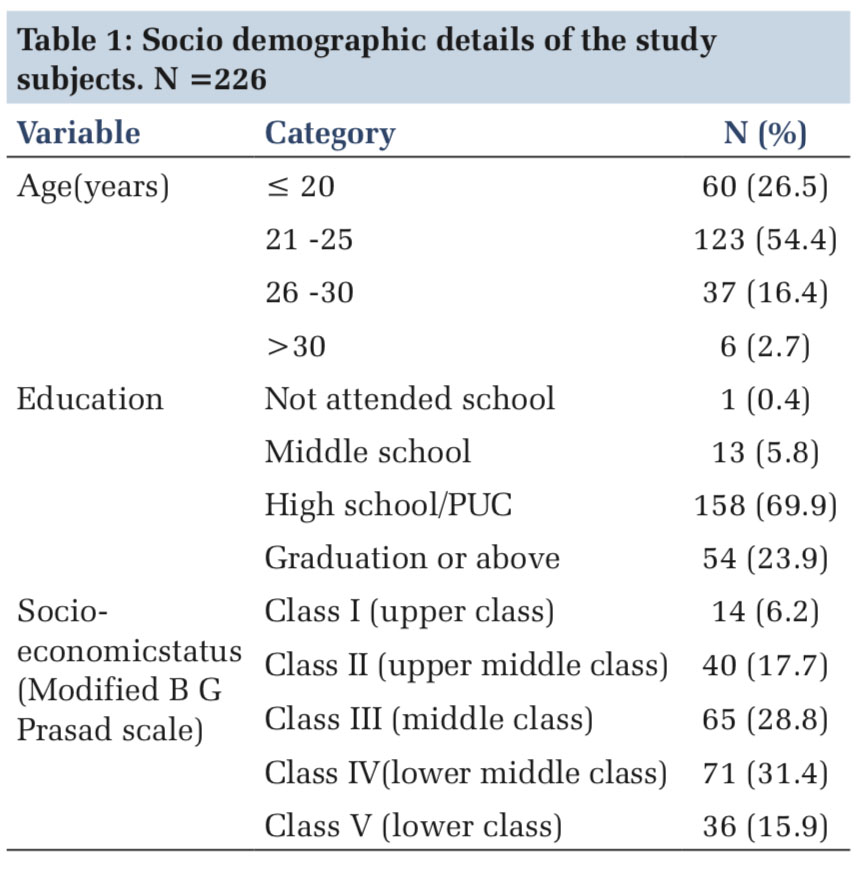
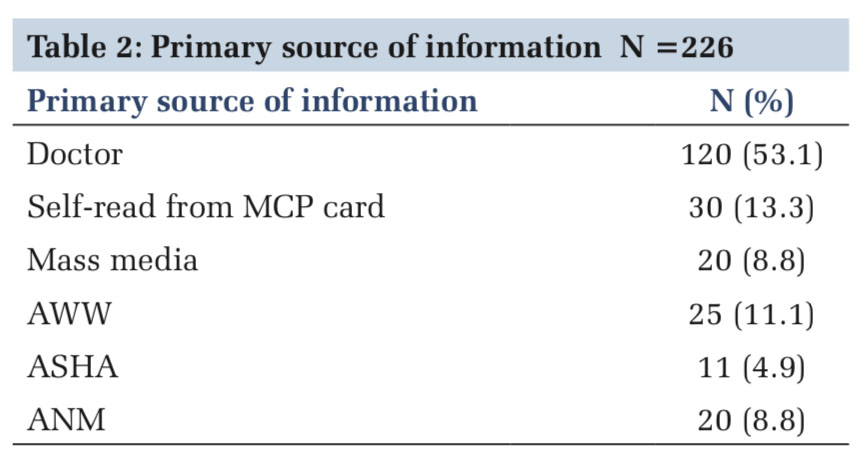
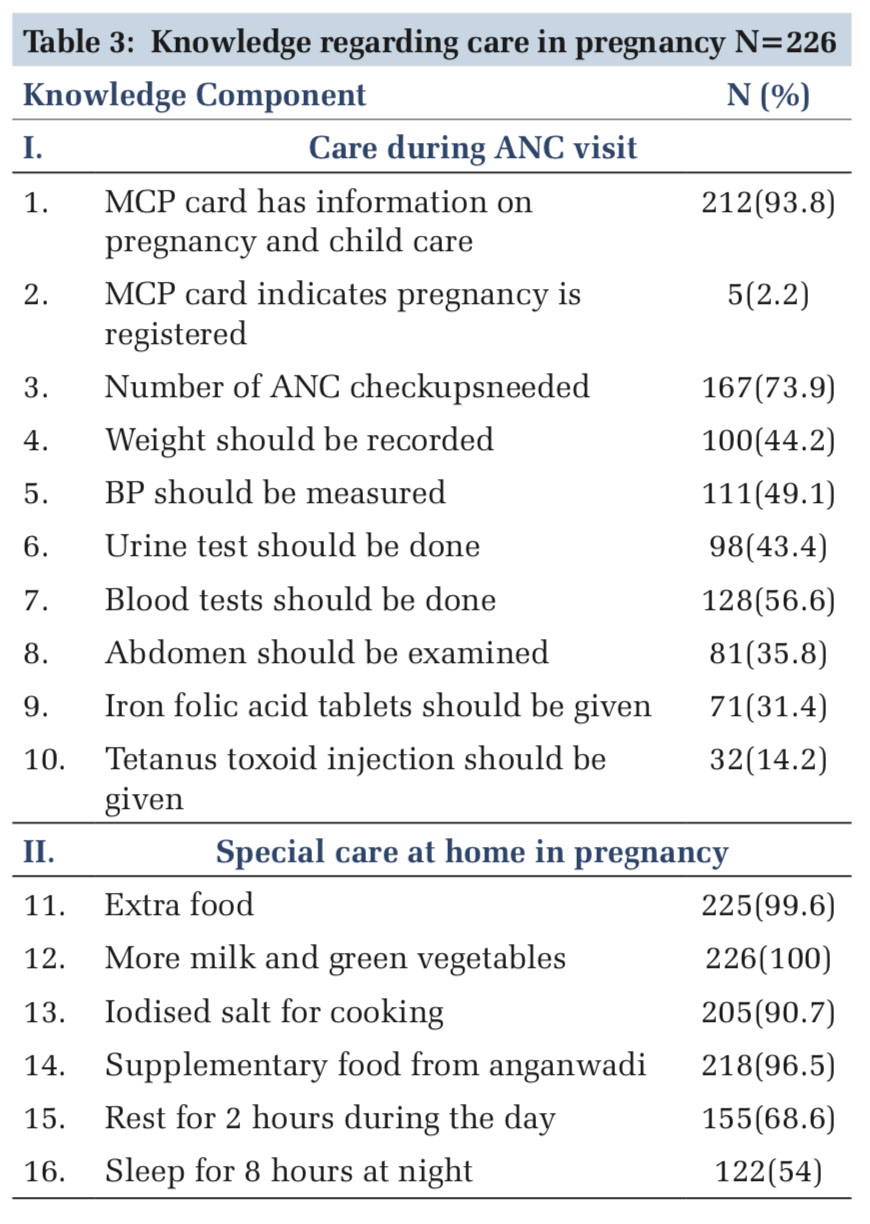
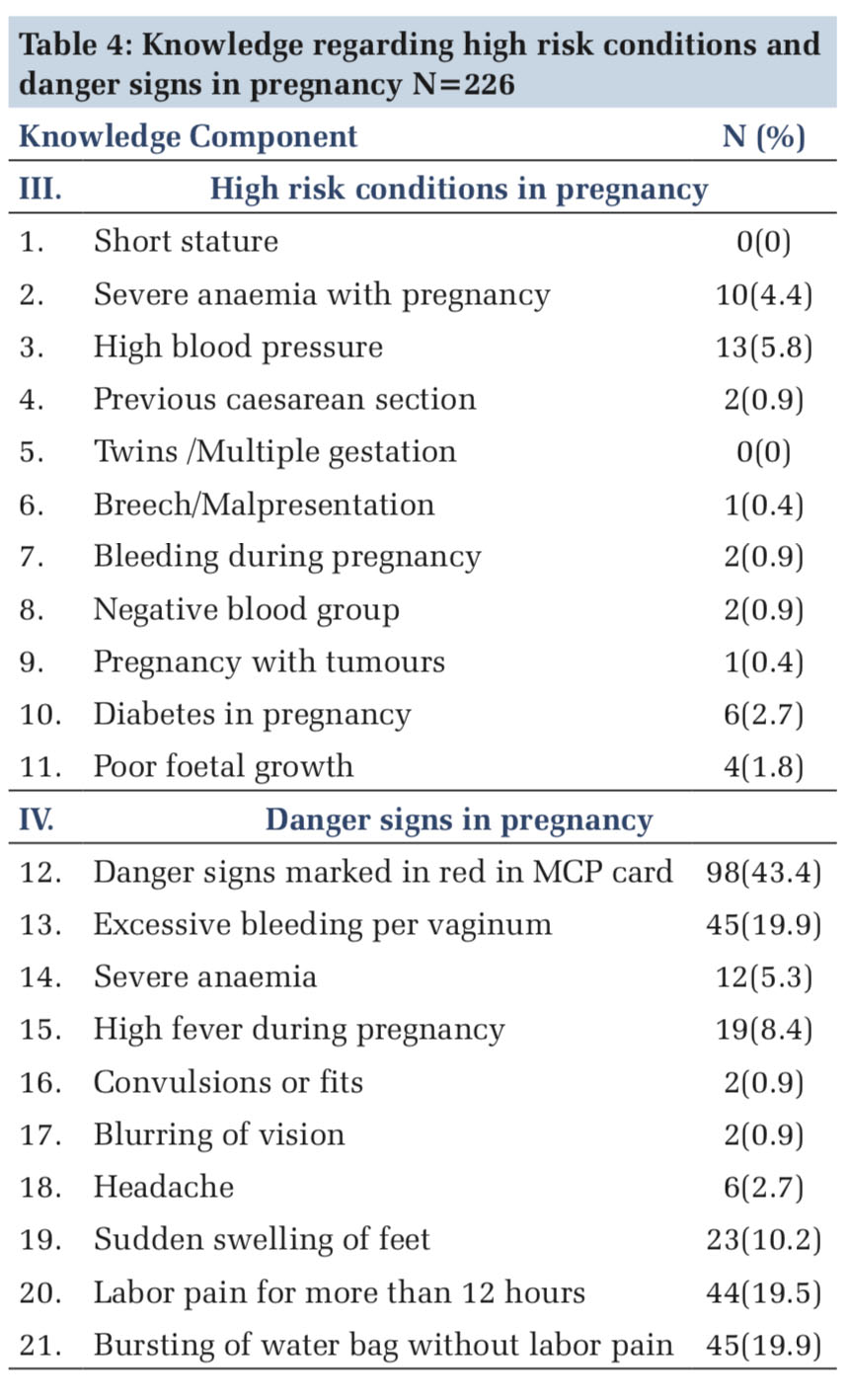
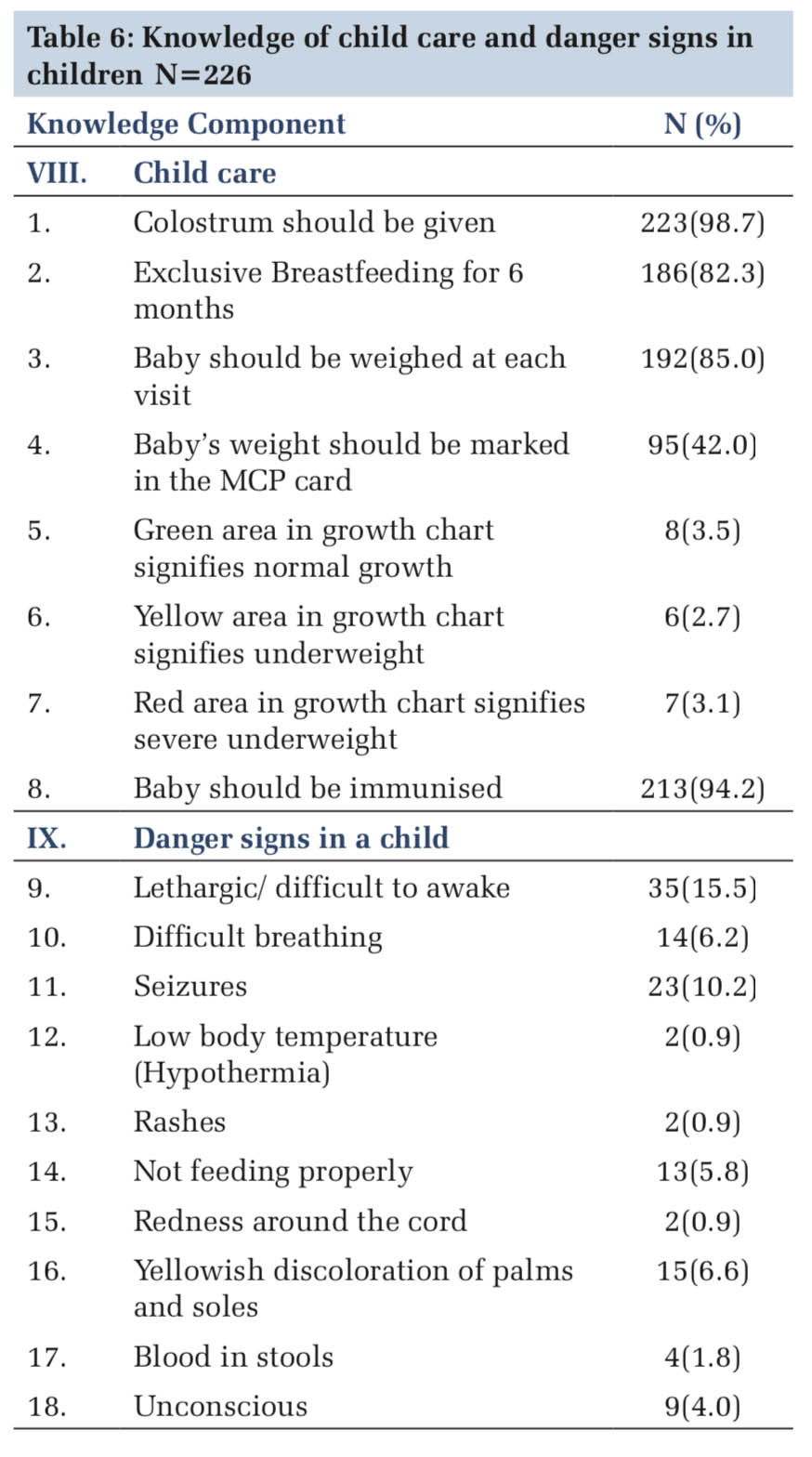
IntroductionMaternal and child health indicators are key in measuring the health status of any country and have been included in the Sustainable Developmental Goals for 2030.[1] While the health status of mothers and children in India have improved over the past two decades, maternal mortality ratio (122/1,00,000),[2] neonatal mortality rate (23/1000), and infant mortality rate (30/1000)[3] remain unacceptably high. The mother and child protection card (MCP card) and the mother and child tracking system were introduced under the National Rural Health Mission (NRHM) in 2010 as part of the efforts by the Ministry of Health and Family Welfare to improve coverage and utilization of maternal and child health services. The MCP card, known as Mamata card, JacchaBaccha card, or Thayi card (in Karnataka), is not only a detailed record of antenatal visits, immunization and growth monitoring for the infant, as well as other services rendered during pregnancy, postpartum, and childhood but also has been developed as a health education tool for families to learn, understand and follow positive practices for achieving health and well-being of pregnant women, mothers, and children till the age of five.[4] The MCP card provides information about services which can be accessed, and details about the care of mothers and children including recognition of danger signs, to empower families to make decisions for care of womenandchildren.[5]TheMCPcardisalsoused by village level workers such as ANMs, Anganwadi workers, ASHA workers, doctors, nurses, and ICDS supervisors. As the first contact point between a pregnant woman and the health system, the MCP card has the potential to create awareness, facilitate community dialogue and generate demand for uptake of vital services being provided.[6] Materials and MethodsThis was a cross-sectional study done from March to May 2017, among women in possession of an MCP card provided by Government of Karnataka, availing maternal and child health services from a rural, secondary level maternity hospital in Ramnagara District, South Karnataka. Approval was obtained from St. John’s Medical College Ethics Committee. Subjects included in the study were pregnant women attending the antenatal outpatient clinic (gestational age >20 weeks), pregnant women admitted for delivery and post-natal mothers up to 6 weeks following delivery. Inclusion criteria were possession of MCP card for at least 4 weeks. Women in active labor were excluded from the study. Based on a previous study,[6] where 63% of pregnant women with MCP card had heard of anemia in pregnancy, the sample size was calculated to be 226 with 10% relative precision and 95% confidence limits. Consecutive sampling was employed. After obtaining informed consent, the respondents were interviewed using a pre-tested, face-validated structured interview schedule in the local language Kannada. The interview schedule consisted of socio-demographic and obstetric details and questions to assess knowledge on care during pregnancy and delivery, post-natal and childcare based on information provided in the MCP card (2012 edition).[10] There were nine components with a total of 71 questions to assess knowledge: I. Care during ANC visit (10 questions) II. Special care at home in pregnancy (6) III. High risk conditions in pregnancy (11) IV. Danger signs in pregnancy (10) V. Institutional delivery (6) VI. Maternity Benefit schemes (6) VII.Family planning in postnatal period(4) VIII. Childcare (8) IX. Danger signs in a child (10). Each correct response was awarded a score of one, giving a maximum possible knowledge score of 71. If women were able to answer at least half of the questions, that is, a score of 35 or higher, they were considered to have adequate knowledge. Scores < 35 were considered as poor knowledge. The data were entered into Microsoft Excel and analyzed using SPSS v17. The exposure variables (socio- demographic and obstetric factors) were described using proportions, mean and standard deviation. The outcome variable (knowledge regarding care in pregnancy and delivery, post-natal and child care, as per MCP card) was described as mean knowledge score with standard deviation, and median score with inter-quartile range. Data were normally distributed; therefore, independent –t-test, one-way ANOVA test and Pearson’s correlation were used to determine association between mean knowledge scores and the various socio-demographic and obstetric variables. P < 0.05 was considered statistically significant. ResultsA total of 226 subjects participated in this study. This included 183 (81%) pregnant women and 43 (19%) post-natal mothers. The mean age of the study subjects was 23.09 ± 3.18 years with most (54.4%) belonging to the age group of 21–25 years. Most of them (94.7%) were Hindu by religion, most (93.8%) had completed high school or higher and most (91.6%) were homemakers. Most of the subjects belonged to middle or lower middle class according to modified BG Prasad scale[11] [Table 1]. All the women were married. Among the spouses of the study subjects, 89.3% had a minimum of high school education. About 46.9% were salaried employees, 24.8% were self-employed, 17.7% were farmers, and 10.6% were daily wage laborers. All the study subjects had MCP card which was given to them at the time of registration of pregnancy. Only 30 (13.3%) said that self-reading the MCP card was their primary source of information regarding pregnancy and childcare. For most, the primary source of information regarding pregnancy and child healthcare was the doctor [Table 2]. The overall mean knowledge score of the participants was 19.6 ± 5.5 and median knowledge score was 19.0 (IQR=16, 23). All the women in our study were found to have poor knowledge as none of the subjects had a knowledge score of 35 or above. Awareness regarding tetanus immunization and iron and folic acid (IFA) tablets were low. More than half of the mothers were unaware that blood pressure, weight, and abdomen should be examined at each ANC visit [Table 3]. Knowledge regarding high risk conditions in pregnancy and danger signs in pregnancy was abysmally low [Table 4]. Knowledge about the various components of institutional delivery and maternity benefit schemes was poor; however, mothers were aware of 108 ambulance facility. Knowledge regarding spacing of births and contraception in the post-natal period was better, but postpartum intrauterine contraceptive device (PPIUCD) awareness was non-existent [Table 5]. While knowledge regarding breastfeeding and immunization was adequate, mothers were unaware of how to interpret the growth chart of the child. Awareness of danger signs in a child was also unacceptably low [Table 6]. DiscussionThis study estimated the level of knowledge among pregnant and postnatal mothers in possession of MCP card, regarding care during pregnancy and delivery, post-natal care, and childcare care, based on the information provided by the MCP card. All the study subjects had an MCP card, yet it was found that MCP card was the primary source of information regarding pregnancy and childcare for only 13.3%. This could be the reason for the overall low mean knowledge score of 19.6 (out of a maximum of 71). Since most women had not read the card, they were unable to answer questions based on the information provided by the MCP card. Most women stated doctor as being the primary source of information, yet their mean knowledge score was significantly lower as compared than those whose primary source was village level workers (ASHA/AWW/ANM), media, and self- reading the MCP card. This has definite public health implications, as it indicates that women are not being advised to read the MCP card for health information, doctors are not using the MCP card as a health education tool, and more importantly, reading the MCP card is an easy way for women to gain knowledge regarding pregnancy and child care. This has been shown in a study in rural Gujarat, where 65% of pregnant and post-natal mothers had read the MCP card and were able to adequately state danger signs in pregnancy.[12]
|
ConclusionAwareness regarding pregnancy and child care was poor among the study population in possession of MCP card, in spite of MCP card having being developed as a tool for health education. More emphasis should be made in training the healthcare workers (ANMs, AWWs and ASHAs) to use the MCP card as a tool for teaching mothers and also encouraging mothers to repeatedly read the information regarding care and services recorded in the MCP card. |
LimitationSince this was a hospital-based study, the study subjects are not a representative sample of the general population. |
Subscribe now for latest articles and news.