Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i01.007
Year: 2016, Volume: 2, Issue: 1, Pages: 34-36
Case Report
H P Sapna1, T N Harsha2
1Senior Resident, Department of OBG, JSS Medical College & Hospital, Mysuru,
2Consultant Gynaecologist, Department of OBG, District Hospital, Madikeri
Address for correspondence: Dr. Sapna H P, #268/C ‘Shivasadana’, 7th Cross Road, 3rd Stage, Gokulam, Mysuru - 570002, Karnataka, India. E-mail: [email protected]
Heterotopic pregnancy in natural conception is quite rare and most often presents as a life-threatening emergency like acute abdomen and hemorrhagic shock. In early unruptured stage, it presentation is nonspecific mimicking normal and abnormal pregnancy. A high index of suspicion and a definitive search for it even after confirming normal intrauterine gestation is needed. This little effort ensures a timely diagnosis and management thus preventing catastrophe. We hereby report a rare case of multigravida with unruptured heterotopic pregnancy following a spontaneous conception, who presented to us with nonspecific abdominal pain.
KEY WORDS:Ectopic pregnancy, heterotopic pregnancy, natural conception, transabdominal and transvaginal ultrasonography.
IntroductionHeterotopic pregnancy is quite rare following spontaneous conception. According to Peleg et al., It is defined as the presence of intrauterine and extrauterine gestation.[1] Extrauterine being commonly seen in the fallopian tube and uncommon being cervix[2] and or ovary.[3] The incidence of heterotopic pregnancy is very low. The incidence was originally estimated on a theoretical basis to be 1 in 30,000 pregnancies. However, recent data indicate that the rate is higher due to assisted reproductive techniques and it is approximately found to be 1 in 7000 overall and is as high as 33/10000 with ovulation induction.[4] Below is a unique case history of heterotopic pregnancy in a clinically stable patient without any risk factors which was picked up by ultrasonography. This case report stresses the importance of holistic approach and thorough ultrasonography in managing these types of patients.
Case ReportGravida 4 para 3 living 3 with 2½ months of amenorrhea came with severe pain abdomen of 2 days duration. Vitals were stable. Per abdomen tenderness was noted in the lower abdomen. No guarding/rigidity noted. Per speculum - cervix and vagina healthy, no active bleeding noted. Per vaginal examination-cervical motion tenderness+, uterus bulky in size, non-tender, right fornicial fullness+, tenderness+, left fornix free and non-tender. Urine pregnancy test was found to be positive.
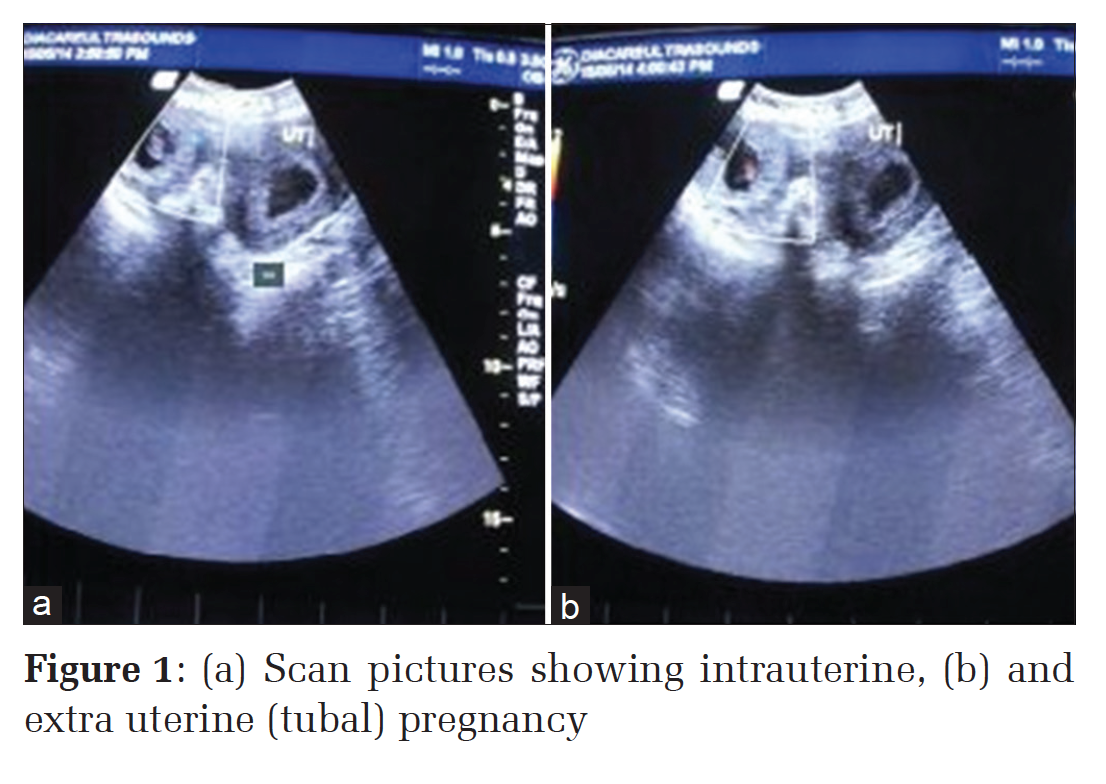
Transabdominal scan revealed single live right tubal pregnancy of 7 weeks 6 days with minimal free fluid in pouch of Douglas with a single intrauterine gestational sac of 17 mm noted without yolk sac and fetal pole (Figure 1). Transvaginal scanning (TVS) was done to confirm the same. The Doppler study of the right adnexal mass showed low resistance flow. Blood investigations done which revealed were all within normal limits with Hb 11.6 g/dl. A provisional diagnosis of heterotopic pregnancy with unruptured right ectopic pregnancy was made. The patient was taken for emergency laparotomy as laparoscopy was not available in our center and was found to have an unruptured right sided ampullary tubal pregnancy with minimal hemoperitoneum. Right sided salpingectomy (Figure 2) and left sided tubectomy were done. The intrauterine gestation was allowed to continue as the patient did not agree for termination by evacuation even after thorough counseling but later after 15 days she spontaneously aborted. |
|
DiscussionThe early diagnosis of heterotopic pregnancy is quite challenging because of the lack of clinical symptoms and signs as well as diagnostic confusion with other early pregnancy issues.[5] With an increase in trend of assisted reproductive techniques, there is an increase in assisted conception, the likelihood of detecting heterotopic pregnancy following assisted conception will increase, but spontaneous heterotopic pregnancy remains a diagnostic dilemma and a challenge for gynecologists. Laparoscopy has been found to be useful for the early diagnosis of heterotopic pregnancy and has resulted in good surgical outcomes. There are various risk factors for heterotopic pregnancy, like history of previous tubal damage (after previous tubal surgery endometriosis, endometriosis or pelvic inflammatory disease), previous ectopic pregnancy and assisted reproductive techniques (pharmacological ovulation stimulation, in-vitro fertilization, gamete intrafallopian transfer). There are also few cases which have been reported in a natural cycle.[6] In our case study except for multigravida, there were no other risk factors. Heterotopic pregnancy can has various presentations. It has to be considered more likely (a) after assisted reproduction techniques, (b) with persistent or rising human chorionic gonadotropin levels after dilatation and evacuation for an induced/ spontaneous abortion, (c) when the uterine fundal height is larger than that for her menstrual dates, (d) when there is more than one corpus luteum present in a natural conception, and (e) when a vaginal bleeding is absent with the presence of signs and symptoms of ectopic gestation.[7] The clinical presentation of an unruptured heterotopic pregnancy is highly nonspecific and is variable. The common presenting symptoms and signs are pain abdomen, adnexal mass, peritoneal irritation and an enlarged uterus.[8] Heterotopic pregnancy is likely to be missed in natural conception unless a sonologist is aware of and carefully screens the tubes and pelvis. If overlooked, it may present with rupture and acute abdominal syndrome, which can lead to maternal shock and death. Our patient just had non-specific pain abdomen and without any other manifestations. Transvaginal ultrasonography is an important aid in the diagnosis of heterotopic pregnancy but ultrasonographic findings such as extrauterine gestational sac with fetal cardiac activity, fetal node and hyperechogenic ring surrounding the gestational sac and adnexal mass points towards tubal heterotopic pregnancy.[9] Any Suspected adnexal masses have to be investigated by Doppler ultrasound to improve its sensitivity and specificity. Our case study was diagnosed by ultrasonography based on her clinical symptom of pain abdomen. The heterotopic pregnancy can be managed by various methods. First being few cases may spontaneously resolve without any intervention.[10] However, there are no clear guidelines for the same. The second one being medical treatment, i.e. potassium chloride or hyperosmolar glucose has to be injected locally to the intact heterotopic gestational sac or fetus via laparoscopy or TVS.[11] These two options are useful in very few cases. The last option being surgical removal of the ectopic gestation by salpingectomy or salpingostomy which is the most common mode of treatment. Laparotomy was widely used in the past, but laparoscopy is now being preferred due to early post-surgical recovery.[12] However, a laparotomy may be preferred in cases with serious intraabdominal bleeding or in patients with hemorrhagic shock. Our patient though was clinically stable was subjected to emergency laparotomy and was found to have a right sided unruptured tubal ectopic pregnancy with minimal hemoperitoneum so was further proceded with right sided total salpingectomy and left sided tubectomy. Her intrauterine pregnancy was allowed to continue as per patients request. The sonologists have to be very keen in screening the adnexa even after they find the intrauterine gestational sac because in the busy schedule one has the tendency to miss the adnexal pathology once intrauterine pregnancy has been diagnosed.
ConclusionHeterotopic pregnancy though extremely rare can occur even in spontaneous conception. Hence, It requires a high index of suspicion for early and timely diagnosis and management. A timely intervention can result in a successful intrauterine fetus, thus preventing a catastrophe like tubal rupture and hemorrhagic shock which can be life threatening. |
Subscribe now for latest articles and news.