Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i3.22.469
Year: 2023, Volume: 9, Issue: 3, Pages: 343-346
Case Report
Md. Samim Iqbal1 , Urvashi Ghosh2 , Rina Mukherjee3 , Shyamalendu Mandal4 , Ankit Deb1 , Jayeeta Dutta5
1 Junior Resident, Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata, West Bengal, India,
2Senior Resident, Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata, West Bengal, India,
3Head of the Department, Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata West Bengal, India,
4Visiting Specialist, Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata, West Bengal, India,
5Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata, West Bengal, India
Address for correspondence:
Urvashi Ghosh, Senior Resident, Department of Pathology, B R Singh Hospital, Eastern Railway, Kolkata, West Bengal, India.
Email: [email protected]
Received Date:08 November 2022, Accepted Date:11 September 2023, Published Date:28 December 2023
Invasive carcinoma of no special type (NST) or ductal carcinoma is the most common type of invasive breast cancers. Invasive lobular carcinoma (ILC) is the most common special variant amongst breast cancers that lacks some of the common features associated with breast cancers e.g. absence of desmoplastic reaction and infrequent mitosis. Some cases of ILC produce intracellular mucin that pushes the nucleus to one side, creating the characteristic signet ring cell morphology. Extracellular mucin secretion is essentially described in association with mucinous breast carcinoma and ductal carcinoma. Very few cases of ILC showing extracellular mucin has been reported in literature. Herein, such a rare case of classic lobular carcinoma is described, in a 70-year-old female who presented to the Surgical department of our hospital.
Keywords: Breast cancer, Extracellular mucin, Invasive lobular carcinoma
Ductal and lobular carcinomas are typically considered two distinct types of mammary carcinoma. Invasive lobular carcinoma (ILC) of the breast is the second most common variant of breast carcinoma. It accounts for 5-15% of invasive mammary carcinomas 1 . Lobular neoplasia and infiltrative lobular carcinoma may produce intracellular mucin, when the secretion is prominent; the cells have a signet ring configuration. But, rarely cases have been reported of lobular carcinoma with extracellular mucin.
In this manuscript, we report a case of ILC showing presence of extracellular mucin lakes, in an elderly female in her eighth decade of life.
A 78-year-old woman presented to our hospital's surgical outpatient department complaining of pain and a lump in her right breast for approximately six months. On examination, a firm to hard lump was felt in the upper and lower outer quadrant of her right breast. Along with that, there was also ulceration of the overlying skin lateral to the nipple-areolar complex, which was mildly tender and bleeding on touch.
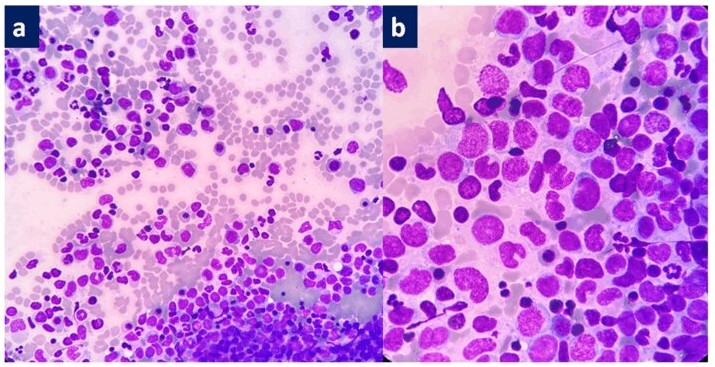
Imaging studies were performed. Mammography demonstrated a well-circumscribed oval shaped mass of mixed echogenicity in the outer half of the right breast. BI-RADS (Breast Imaging Reporting and Data System) score was given as 4b, that is suspicious of malignancy. Based on these findings, core needle biopsy of the lump was advised and performed. Core biopsy showed presence of malignant cells lying in islands amongst extracellular mucin pools. The diagnosis was given as mucinous carcinoma of breast. Modified Bloom Richardson score came out to be 7 (Grade II). Immunohistochemical (IHC) studies were also performed, where ER and PR were positive, Her2/neu negative and Ki-67 proliferative index was 28 %. Following this, modified radical mastectomyFigure 1].

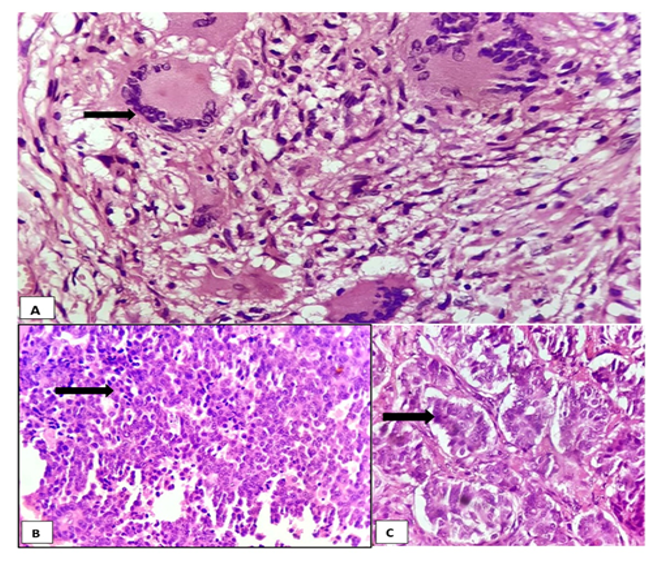
Microscopy revealed most of the areas on the tumor sections (around 70%) showing features of classical lobular carcinoma, comprising mostly solid and nested growth pattern, infiltrating cords and single files of malignant cells. The tumor cells were small to medium in size with relatively uniform, round nuclei and small nucleoli, along with scant to moderate amount of cytoplasm. Around 30% areas showed malignant cells lying in islands observed to be floating in lakes of extracellular mucin. Few signet-ring cells with intracytoplasmic vacuoles were also seen. PAS (Periodic Acid Schiff) staining of additional sections were done which confirmed the presence of mucin lying in the extracellular environment [Figure 2]. Further IHC was done on the tumor for e-cadherin which showed loss of e-cadherin expression on the tumor cells, a characteristic feature of Lobular carcinoma. Thus, the final diagnosis was given as Invasive Lobular Carcinoma with Extracellular Mucin (ILCEM).

Ductal carcinoma and lobular carcinoma are two distinct histological subtypes of breast carcinoma with characteristic morphology, immunohistochemical profile, and clinical behavior. ILC has several histological subtypes- classic, solid, alveolar, pleomorphic, tubulolobular, signet ring cell, and mixed type. Loss of cellular cohesion is a common feature of all with the classic variant demonstrating proliferation of dyscohesive small cells individually dispersed or arranged with a typical single-file pattern, known more commonly as the ‘Indian file’ pattern. The tumor cells are round to oval, with round nuclei and low mitotic activity, present in a concentric pattern around existing ducts and lobular units (targetoid pattern). The solid variant consists of sheets of lobular cells that have pleomorphic morphology and more mitotic activity than classic lobular carcinoma. The alveolar subtype has classic lobular carcinoma cells that are arranged in globular aggregates consisting of about twenty cells. The pleomorphic type exhibits significant cytological atypia but retains the classic lobular carcinoma pattern of single cell files. Presence of tubules in association with these features defines tubule-lobular carcinoma. The signet ring variant is extremely rare, and the term is reserved for cases where signet-ring cells comprise the exclusive or predominant cell component. The mixed type consists of a mixture of classic and one or more of these variants 2, 3 .
Mucin has been classified as membrane-bound mucin which mediate signal transduction and secretary mucin, which are directly secreted into extracellular spaces 4 . Mucinous breast lesions consist of a wide spectrum from benign fibrocystic changes to mucinous papillary lesions and mucinous carcinomas 5 . Extracellular mucin secretion is generally accepted as an indication of ductal phenotype, including solid papillary neoplasm, ductal carcinoma and mucinous carcinoma and, with the percentage of mucin determining the final histopathological subtype. In contrast, lobular carcinoma has been considered a variant of mucin-secreting carcinoma with only intracytoplasmic mucin 3, 5, 6, 7 .
Our case first underwent core biopsy of the lesion and examination of the cores showed more than 90% areas showing malignant cells lying in extracellular mucin. Thus, diagnosis was given as mucinous carcinoma of the breast. IHC was performed and it was found that the lesion was ER/PR positive, Her2/neu negative and Ki-67 proliferative index was 28%.
However, when subsequent modified radical mastectomy was performed and the tissue was examined in histopathology, it showed majority of areas having appearance of invasive lobular carcinoma, classic variant, with some areas demonstrating extracellular mucin. IHC was performed with ER, PR, HER 2/neu, Ki-67 and e-cadherin. The immmunohistochemical findings were reflective of the core biopsy findings and e-cadherin was negative, which helped to clinch the findings [Figure 3, Figure 4].


This entity was first described in 2009 by Rosa et al. 8 who reported a new variant of ILC that displayed extracellular mucin production. Since then, only about twenty-three cases have been reported in literature. It was observed that ILCEM often presents at higher stage in postmenopausal age group. Most cases presented as a definite mass that was more than twenty mm in size, with tumor cells that frequently show non-classical lobular histological features including signet ring cell change. Some cases demonstrated HER2/neu positivity 8, 9, 10, 11, 12 . Our case fit into the age group and the morphology findings. HER2/neu was performed, and was negative. However, even though a minority of ILC with extracellular mucin have been HER2-positive, 9 the rate of HER2 amplification or overexpression in ILC with extracellular mucin appears to be higher than what has been reported for classic ILC. HER2-positive pleomorphic ILC with extracellular mucin seems to be one of the least common patterns and phenotypes among ILC variants.
Based on all this evidence, extracellular mucin secretion and ILC are not mutually exclusive, as was the findings in our case. In spite of the presence of extracellular mucin, when the characteristic dyscohesive growth pattern and uniform cytology are present, a lobular carcinoma should be considered, and E-cadherin immunohistochemical stain should be performed to confirm the phenotype.
With regards to patient outcomes, published data is very limited but suggest that some ILC with extracellular mucin may have a poor prognosis. In 2 studies with 8 and 10 cases each and median follow-up periods of ≤3 years, the breast cancer-specific mortality was 20% to 40% 13, 14 .
Based on our findings and subsequent discussion, it can be concluded that extracellular mucin secretion is not an exclusive feature of ductal phenotype, and the classical morphologic definition of ductal and lobular carcinomas could sometimes be misleading. Till date, only twenty cases of ILCEM had been reported in literature. This phenotypic heterogeneity could be reflective of the molecular and genetic alterations in the evolutionary pathway.
It is important for pathologists to recognize this new entity because it mimics a NST carcinoma, as such a diagnosis may require a different approach in clinical management and surveillance. It is important to develop awareness of this unusual pattern of ILC, so as to prevent misdiagnosis in the future. However, this is just the tip of the iceberg and further studies are needed to document the biological behavior as well as molecular profiles associated with the phenotypic hybrids and their implications in clinical management.
Subscribe now for latest articles and news.