Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i01.005
Year: 2020, Volume: 6, Issue: 1, Pages: 21-26
Case Report
N Thulasivasudevaiah1, S Sudhir2, P Deepak Naik3, D K Dilip4, Ankit Raj5, Sujitkumar Sah5
1Associate Professor, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India,
2Professor, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India,
3Assistant Professor, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India,
4Senior resident, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India,
5Junior residents, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India
Address for correspondence:
N Thulasivasudevaiah, Associate Professor, Department of Surgery, JSS Medical College and Hospital, JSS Academy of Higher Education and Research, Mysore, Karnataka, India. Phone: +91-9741939850. E-mail: [email protected]
Background: The midline sacrococcygeal pilonidal sinus is the common surgical condition among younger population. They present to surgical outpatient department with pain and history of pus discharge from natal cleft. These patients approach for permanent cure following repeated attacks of pain and abscess drainage. We present a new surgical technique of primary closure by applying deep tension sutures (DTS) to close the defect following excision of midline sacrococcygeal pilonidal sinus. The rationale behind this technique is to avoid prolonged hospital stay and early return to work.
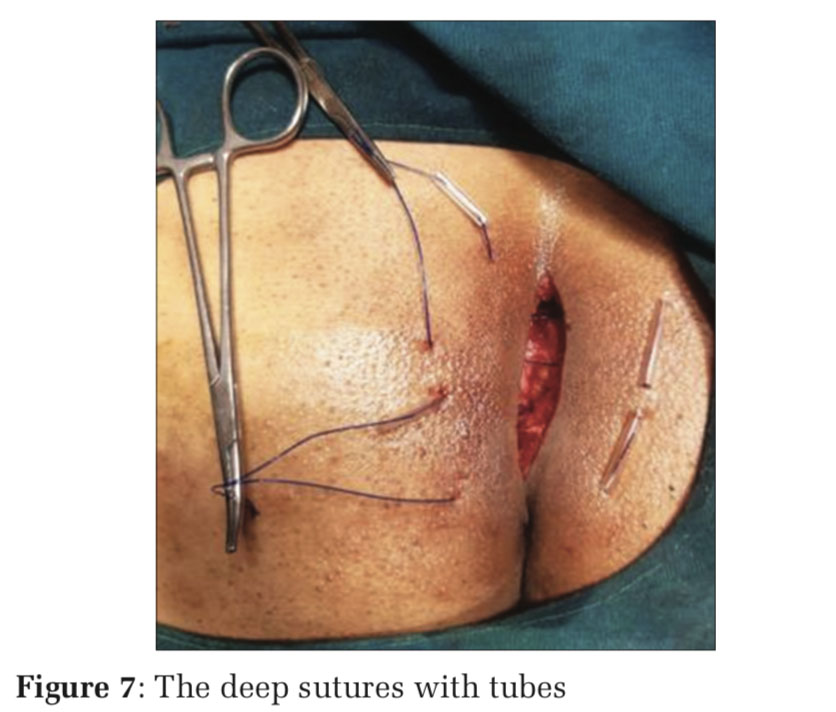
Materials and Methods: In this study, a group of five patients (one female and four male patients) with the age group between 18 and 35 years was studied for the effectiveness, duration of hospital stay post-operative complications, and recurrence following the new surgical technique of DTS. Following excision of midline sacral pilonidal sinus, the resulting elliptical wound varying from 6 cm to 10 cm was approximated using two or three DTS with No-1 Prolene. In this suturing technique, the sutures were held in place using small pieces of plastic tubing from intravenous drip set to avoid suture cutting through the skin. This technique was similar to abdominal wound closure in cases of complete wound dehiscence. The superficial part of the wound was approximated using No-3 zero Ethilon. In this procedure, author has not used any type of drain in the wound. No suture materials were used inside the wound to approximate the raw area (e.g., Vicryl suture). Patients were covered with IV antibiotics and analgesics for a period of 5 days. All sutures were removed on the 10th day.
Results: There were no post-operative complications noted during the hospital stay and during follow-up period ranging from 2 months to 6 months. The scar was healthy with functionally, cosmetically acceptable results. There was no recurrence noted in our study group during the follow-up.
KEY WORDS: Deep tension sutures, pilonidal, sacrococcygeal.
The midline sacrococcygeal pilonidal sinus is the common surgical condition among younger population. They present to surgical OPD with pain and history of pus discharge from natal cleft. These patients approach for permanent cure following repeated attacks of pain and abscess drainage. We present a new surgical technique of primary closure by applying deep tension sutures to close the defect following excision of midline sacrococcygeal pilonidal sinus.
Case No-1
A 35-year-old male presented with a small sinus in the natal cleft for 3months duration. There was a history of a minor surgical procedure for pilonidal abscess. The patient was an auto driver by occupation. On local examination of sacrococcygeal region, there was a single midline sinus without any signs of inflammation. There were no comorbidities such as diabetes or pulmonary tuberculosis.
After baseline investigations, a preliminary diagnosis of pilonidal sinus in natal cleft was made. The patient underwent excision of pilonidal sinus under spinal anesthesia. In prone position, the opening of the sinus infiltrated with methylene blue dye to facilitate sinus track identification for complete excision.
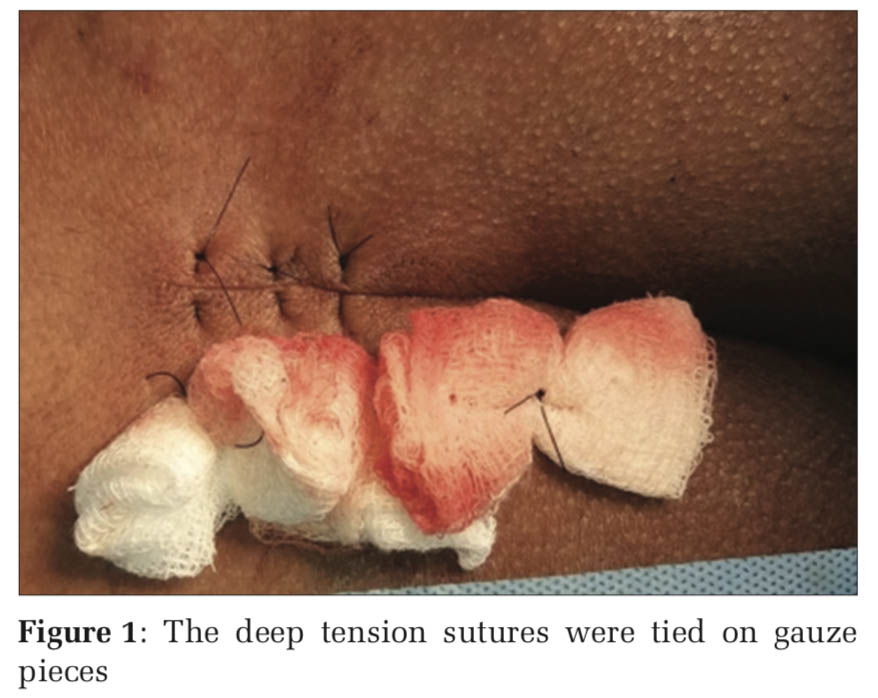
In our first case i have used polypropelene sutures to close the deeper dead space without including the skin on the opposite side, and tied over a gauze piece on one side. This method was improved in subsequent cases by including the full thickness of the wound edges on both sides (Figure 1). In the remaining four patients, the author has used small pieces of IV drip set tubing while tightening the suture by approximating both cut edges. The superficial skin edges were approximated using 3-0 non-absorbable suture (Ethilon). The excised specimen was sent for histopathological examination, which showed features of pilonidal sinus.
Postoperatively, IV antibiotics and analgesics were given for 5 days. The deep sutures were removed on the 7th day. Superficial sutures were removed on the 10th day. The patient was followed up after 3 weeks (Figure 2) and after a period of 6 months with no complaints.
Case No-2
A young adult male aged 31 years who is a software engineer by profession was admitted to surgical wards with a history of intermittent purulent discharge from natal cleft with pain for 6 months. He has undergone drainage of pilonidal abscess at his native place on two occasions. He has experienced the discomfort and repeated visits for the dressing following recurrent pilonidal abscess drainage at peripheral hospital.
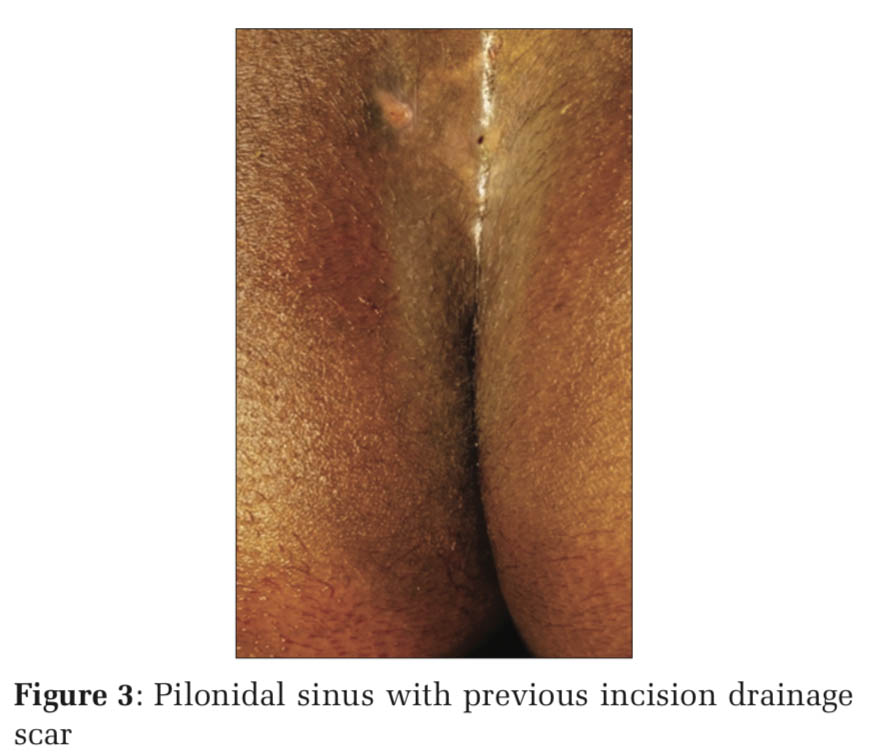
On examination of the sacrococcygeal area, there was a sinus opening amidst a scar with a lateral track extending for 2 cm to the left of midline (Figure 3).
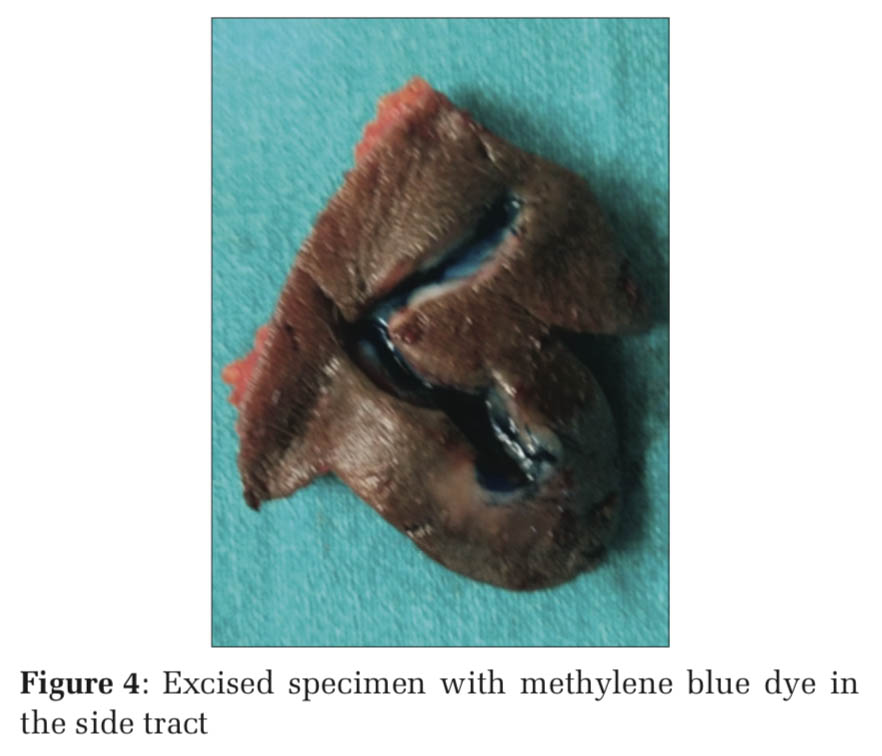
The blood investigations were normal. The patient was explained about the different surgical options and advantages of primary closure by deep tension sutures (DTS). Under spinal anesthesia in prone position, the gluteal folds were separated by adhesive plaster. The midline sinus opening was infiltrated with methylene blue dye. The entire pilonidal sinus with lateral extension (branching) was excised completely (Figure 4). The resulting elliptical defect in subcutaneous plane was approximated by DTS tied over small pieces of rubber tubing. No drain was kept in the wound. The superficial skin sutures were placed using 3 zero Ethilon sutures (Figure 5). The patient was treated with IV antibiotics and analgesics for 4days. The patient was discharged on the 4th postoperative day. On the 7th day, the DTSs were removed. The remaining sutures were removed on the 10th day. The scar was healthy. The excised specimen was sent for histopathology and reported as “pilonidal sinus.” The patient was followed-up for 6 months without any complaints.
Case No-3
A middle-aged male patient (35 years) who is an agriculturist by occupation was admitted with a history of pus discharge from natal cleft for more than 1 1⁄2 years. He has not undergone any surgical procedure in the natal cleft, and his pain and pus discharge were subsiding with a course of antibiotics from health center.
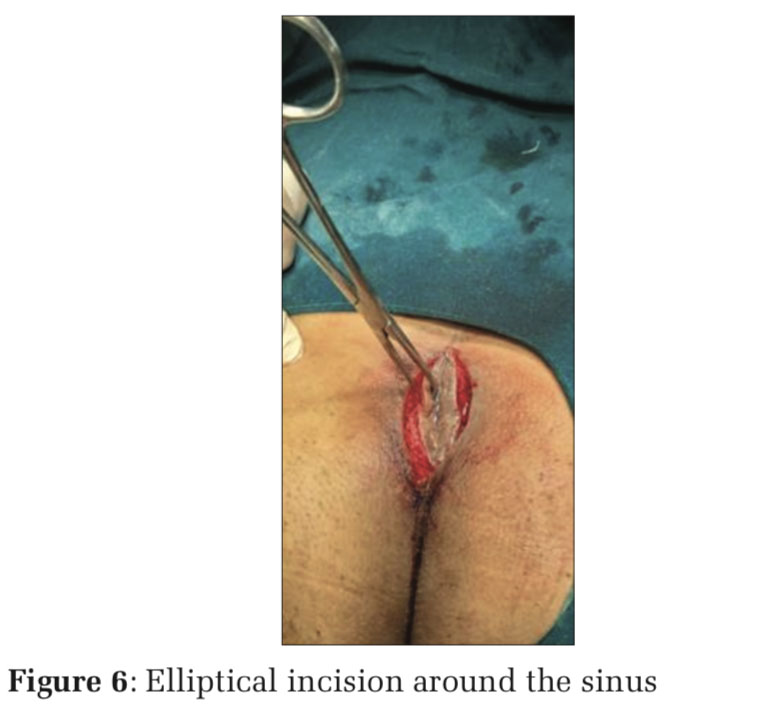
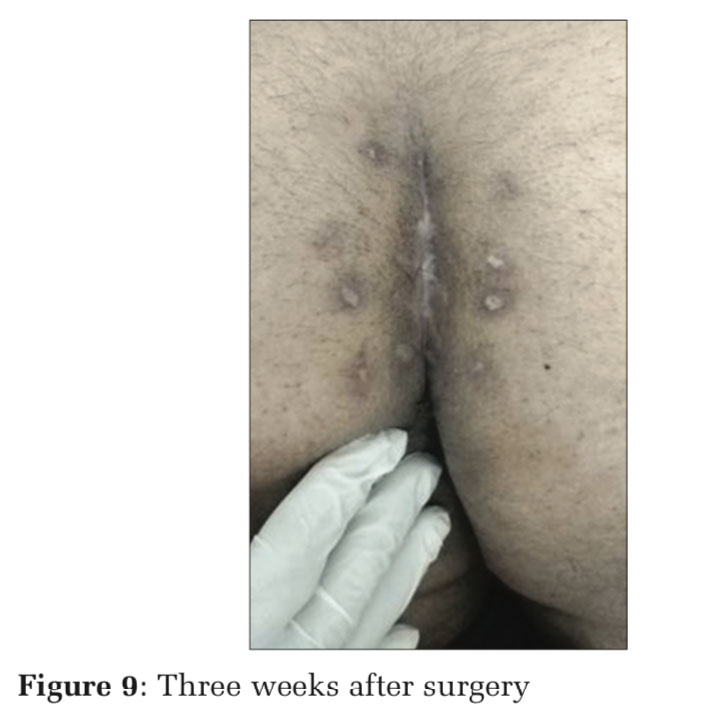
After counseling about the advantages of excision of the lesion with primary suture over lay open technique, the patient has undergone the surgical procedure under spinal anesthesia (Figures 6-8). He was discharged after 3 days IV antibiotics and analgesics. He was advised to take rest at home in prone position. On the 10th day, all sutures were removed. The scar was healthy (Figure 9). The patient was followed-up for 2 months. There were no complications such as recurrence or wound infection.
Case No-4
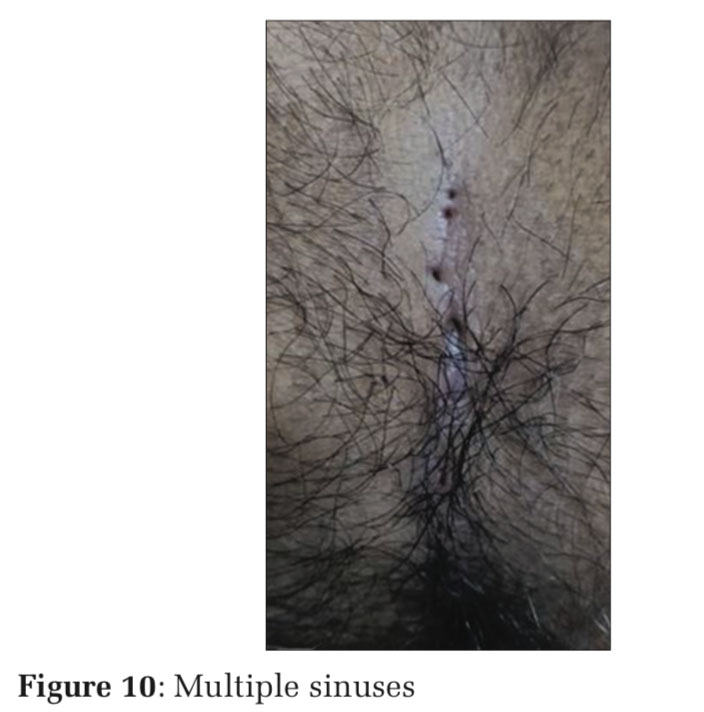
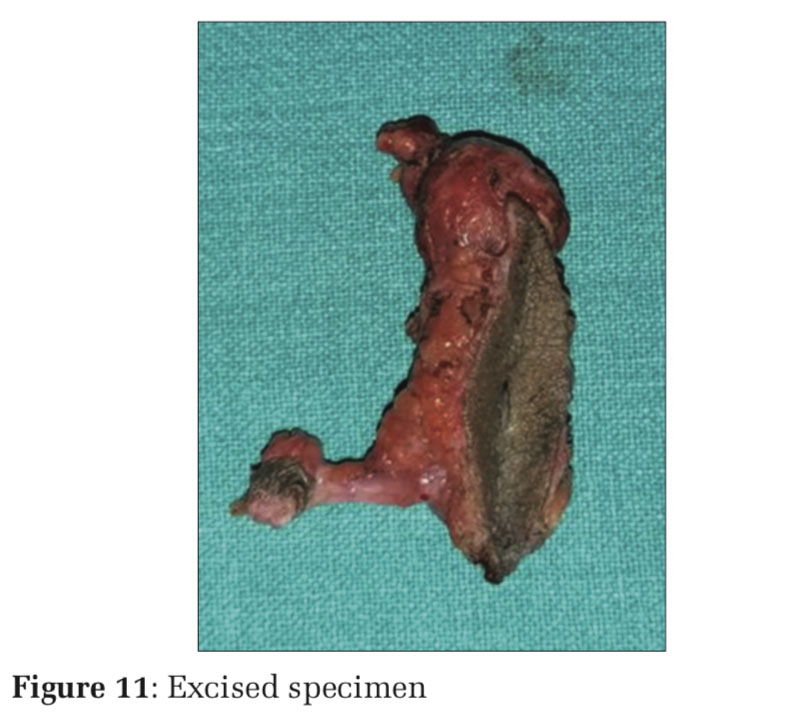
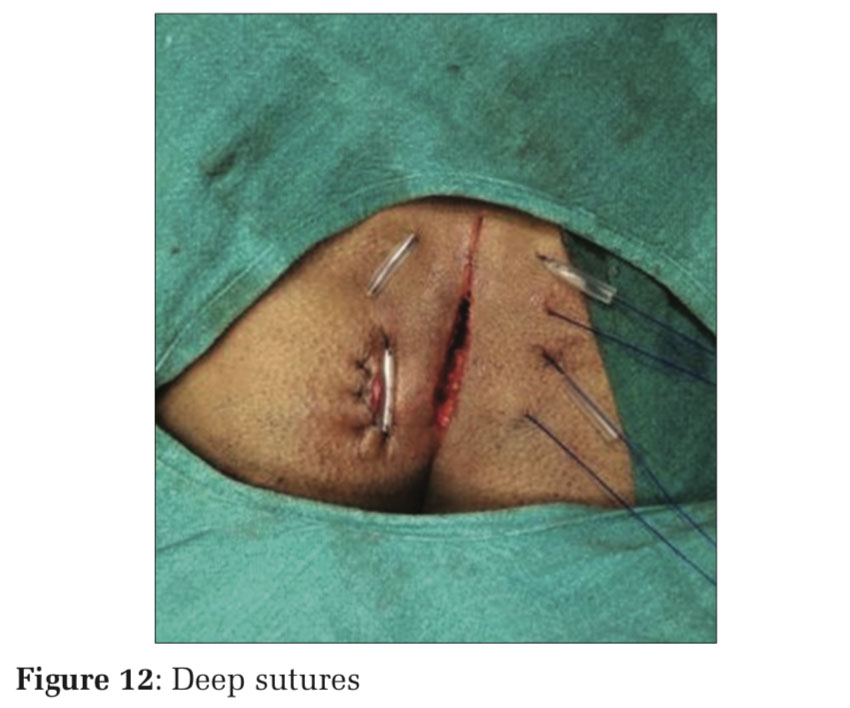
A 23-year-old adult male was admitted with a history of itching in the natal cleft for 2 months, along with recurrent attacks of pain and blood stained discharge from the natal cleft. On examination of sacrococcygeal region, there were midline multiple sinuses with surrounding hairy skin (Figure 10). The patient underwent excision of the pilonidal sinus with an abscess cavity in the upper part of the tract (Figure 11).
Resulting elliptical defect was closed with DTS and superficial skin sutures (Figure 12) The patient complained of itching at the operated site after 3 days, which was managed with antihistaminic tablets until all the sutures were removed on the 10th post-operative day. The patient was followed up for 2 months with no recurrence (Figure 13).
The histopathology of the specimen showed features suggestive of pilonidal sinus.
Case No-5
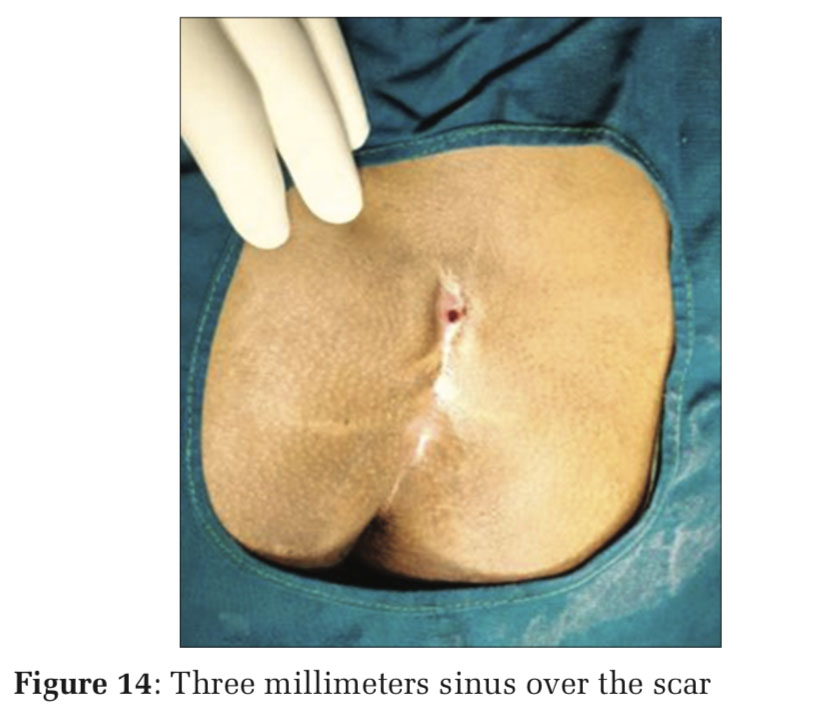
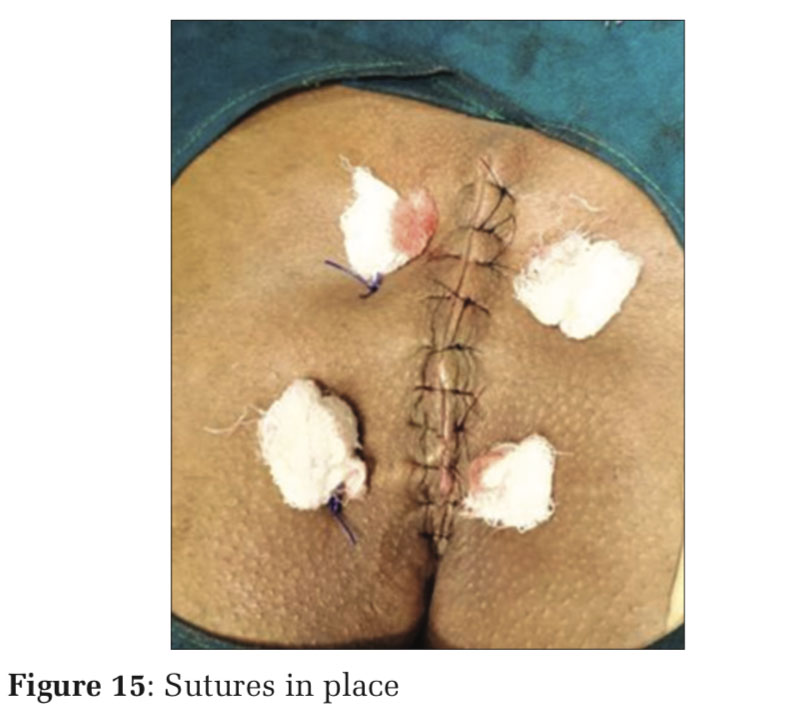
A 19-year-old adult female student by profession, presented with chronic pus discharging sinus in the sacrococcygeal area for 1 1⁄2 years. She has undergone drainage of abscess on two occasions. On examination of the sacrococcygeal area, there was a single sinus of 3 mm over a scar (Figure 14). Routine pre-operative investigations were done. The patient underwent excision of pilonidal sinus followed by DEEP sutures and superficial skin closure (Figure 15). The patient was discharged on the 1st post-operative day with oral antibiotics and analgesics. The patient was instructed to sleep with prone position, all sutures were removed on the 10th day and scar was healthy. There were no post-operative wound complications. No recurrence was observed during 3-month follow-up period.
Chronicsacrococcygealpilonidalsinusiscommon among young and middle-aged male patients.[1] It results from hair penetration beneath the skin at sacrococcygeal region. Symptomatic disease presents as a painful abscess, usually of short duration. History and physical examination are sufficient to make the diagnosis of pilonidal disease regardless of the type of presentation. Patients with pilonidal disease present in three main ways – acute abscess, chronic draining pits, or complex recurrent disease after previous surgery.[2] Any pilonidal abscess should first be drained as an urgent procedure. The various treatment modalities of pilonidal sinus disease include laying open, marsupialization, excision and primary closure, rhomboid excision with Limberg flap closure, V-Y advancement flap, Bascom procedure (follicle removal and lateral drainage), and Karydakis closure (wound closed lateral to the midline). Triangular closure technique is a new procedure invented by Mehmet Mutaf.[3] Surgical management of pilonidal sinus should be simple with a short hospital stay, without any complications, and with low recurrence rate. The patient should have few hospital visits and should return to normal activity at the earliest. In the group of patients who undergo excision of sinus and laying open technique, frequent hospital visits for the regular dressing, until the wound granulate from periphery affects the patient financially and psychologically.
We can overcome this patient’s anxiety by the new technique of wound closure by the author.
Failure to excise the tract completely in the initial surgical procedure, wound infection can lead to recurrence in small subset of patients. Proper wound care and monthly shaving of hair will avoid recurrent sinus disease.[4] In our study group, the drain was not kept during closure of the wound, as in a group of patients, the duration of hospital stay was longer after keeping the drain in the wound.[5]




In the surgical management of the defect following excision of midline sacrococcygeal pilonidal sinus, approximation of the deeper layers of the wound using non-absorbable suture material is the better way of avoiding wound seroma/hematoma. These groups of patients can tolerate the post-operative period well and can return to their work in a short period of time (approximately 10–14 days) compared to patients undergoing lay open technique. The added advantages in this DTS technique are – no drain was kept in the wound and no suture materials were used inside the raw area of wound. There were no post-operative complications noted in all five cases in our group. There were few incidence of flap necrosis and wound dehiscence reported in Limberg Flap closure.[6-8]
Long-term follow-up (12months and 18months) revealed no recurrence among our patients. To summarize, with proper post-operative care of the wound and with simpler technique, minimum appliances to manage the wound, the DTS method is the effective new technique in the surgical management of sacrococcygeal pilonidal sinus.
The authors would like to thank all the OT staff, postgraduates, unit chiefs, colleagues, and patients who were cooperative in this study at JSS Hospital, Mysore.
Subscribe now for latest articles and news.