Introduction
Thyroid diseases are major health problems, that manifested by alteration inhormone secretion, enlargement of the thyroid gland. The mostprevalent thyroid diseases are goiter, hypo or hyperthyroidism, thyroiditis andneoplasms 1, 2. The incidence and prevalence of thyroid diseases in a community are variables which depends on various factors 3.
The presence of thyroid peroxidase (TPO) antibody is a feature of autoimmune thyroiditis and hyperthyroid variant is closely related to Graves’ disease on gross examination and microscopic appearance 4. Thyroid‑stimulating hormone (TSH) receptor antibodies confirm the diagnosis of GD in such cases 5. The autoimmune process involves an underlying genetic predisposition and a trigger (s) that initiate the cascade of events. The identified triggers are infections, life stress, iodine intake, smoking, medications such as amiodarone, interferon, radiation and environmental toxicants 6, 7.
GD is most common in women, the spectrum of clinical presentation ranges from asymptomatic, large goiter to an atrophic gland, euthyroidism, hypothyroidism and rarely hyperthyroidism.8, 9. The pathologic changes include marked lymphocytic infiltration of the thyroid with germinal center formation, atrophy of the thyroid follicles accompanied by oxyphil metaplasia, absence of colloid, and mild moderate fibrosis 10.
Fine needle aspiration cytology (FNAC) is a widely accepted screening procedure in diagnosis of diffuse and solitary thyroid nodules and it is a simple, cost effective, minimally invasive and quick to perform procedure 11. Widespread use of FNAC has reduced number of patients requiring surgery by more than 50%. FNAC not only prevents unnecessary thyroid surgery for benign nodules, but also has increased malignancy rate in resected nodules from 14% to 50% 12. However, the procedure has its own limitations since accuracy is lower in suspicious cytology and in follicular neoplasms 13. FNAC is considered superior as well as more cost-effective in diagnosing than antibody screening 14.
The thyroid is an endocrine organ composed histologically of 20-40 thyroid follicles. They produce hormones triiodothyronine (T3) and thyroxin (T4) which are in turn regulated by thyroid stimulating hormone produced by anterior pituitary gland 15. The lesions of thyroid can be categorized in hypothyroid, euthyroid or hyperthyroid condition based on the assessment of the level of T3, T4 and TSH 16. Thyroid cancers are divided into papillary carcinomas, follicular carcinomas and medullary thyroid carcinomas (MTCs), anaplastic carcinomas, primary thyroid lymphomas and primary thyroid sarcomas 17. The present study aims to assess the complete clinical examination and cytomorphological features of GD and its co relation with anti TPO antibody and its association with clinical and thyroid hormone status of patients.
Methodology
It contained fifty patients with GD (11 male and 39 female), patients were selected Kumaon region hill area and nearby industrial area belt of endemic goiter, iodine deficiency and so many environmental issues. Patients diagnosed from by specialist doctor team in tertiary care referral hospital, otorhinolaryngology (ENT) Outpatient Department (OPD) in Dr. Susheela Tiwari Government Hospital, Haldwani, Nainital, Uttarakhand. The GD was diagnosed by documented clinical and biochemical hyperthyroidism with presence of diffuse goiter. For all subjects, phenotype was determined with the clinician blinded to the individual’s genotype.
Physical examination of graves patients
The physical examination can be grouped under three main categories, examination of the goiter and the surrounding structures, and identifying clinical signs and symptoms of hyperthyroidism specific to GD.
Data collection procedure
All the caregivers of the patients were explained about the purpose of the study and were assured strict confidentiality. Written informed consents were taken from each of them prior to the study. We examined all cases by detailed clinical history, family history, residence, food habits and drug intake with special emphasis on onset, duration and rate of thyroid swelling and particularly any irradiation in the head and neck region in the recent or distant past. In female patients, an enquiry was made about reproductive health too. FNAC was done in all the cases as an OPD procedure with other non-invasive procedures, viz. X-Ray chest PA and Ultrasound, when required. GD sample of FNAC were sent to the Department of Pathology with correct labeling for cytopathological study.
Procedure followed in Fine Needle Aspiration Cytology
The study period included from Oct 2019 to Oct 2022. All the patients with thyroid swellings were referred by ENT OPD to department of pathology for FNAC as well as thyroid hormone assay. FNAC was performed in total fifty cases of thyroid swellings using non aspiration or aspiration techniques by 23 G needle with 20 mL syringe. Cytomorphologic features were reviewed and reported according to "The 2017 Bethesda System for Reporting Thyroid Cytopathology (TBSRTC)" and other parameters eg. presence of granuloma, Hurthle cells, degree of anisonucleosis and giant cells.
Thyroidectomy specimens were fixed in 10% formalin for 12-18 h after gross morphological features were documented and the submitted tissue sections were processed for paraffin embedding. Thereafter 3-5- micron thick tissue sections were obtained and stained with H&E stain. Special stains such as PAS (Periodic Acid-Schiff) and Congo red were used as and when required. The cytological and histopathological findings were correlated.
T3, T4 and TSH were analyzed by electrochemiluminescence (ECLIA) immunoassay by Cobas e411 automated analyzers (Roche Diagnostics, Mannheim, Germany). Normal reference range for T3 was taken as (0.85-2.02 ng/ml); for T4 from (5.13-14.06 ug/dl) and TSH the normal range was (0.27-4.20uIU/ml test were performed on patients’ serum.
Anti-TPO assays were evaluated on the automated analysers Roche Cobas e411. Which uses an electrochemiluminescence immunoassay (ECLIA) technology. The reagents, calibrators and controls were used in this study Elecsys Kit. Calibration for anti-TPO were performed weekly. Anti TPO Positive reference range High (>34 U/ml) Anti TPO reference range Negative Normal (< 34 U/ml). Anti-TPO assays were performed on patients’ serum.
Results
Current study included a total of 50 patients with signs and symptoms of hyperthyroidism and clinical suspicion of GD. All relevant data was collected for evaluation of clinical characteristics. Thyroid function tests (T3, T4 and TSH), Anti-thyroid peroxidase (Anti-TPO) antibody assay and cytomorphology were done for further evaluation. In the present study, patients were in the age group of 13 to 74 years of age. Youngest patient encountered was 13 years and oldest was 74 years. The median age of the study population of 37 years. Females were mostly affected by thyroid diseases than males. Female patients were 39 (78%) and male patients were 11 (22%). Most of the patients presented with diffuse enlargement of thyroid gland and unexplained weight loss with fatigue. A total of 45 patients (90 %) complained of diffuse enlargement of thyroid gland, 44 patients (88%) complained of unexplained weight loss with fatigue and 41 patients (82%) complained of sweating (Figure 1).

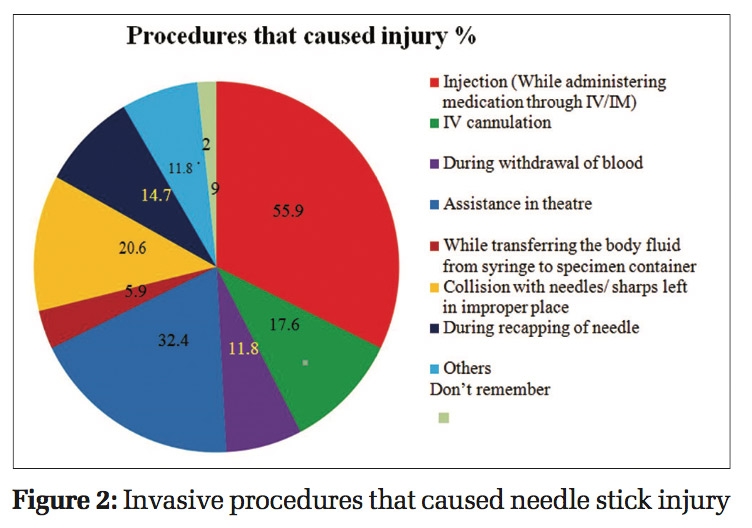
Thyroid function test was done by electrochemiluminescence immunoassay method. 40 patients (80%) presented with elevation of T3 levels and 45 patients (90%) with elevation of T4 levels. Low TSH level was found in only 32 patients (64%), normal TSH level found in 17 patients (34%) and 1 patient (2%) presented with high TSH level. Variation in thyroid function was occur due to most of the patients (38 patients, 76%) were known hyperthyroid for a long time and on therapy for more than 1year. (Figure 2).

Anti-thyroid peroxidase (Anti-TPO) antibody assay was done in all patients. Anti-thyroid peroxidase antibody assay was done by electrochemiluminescence immuno assay method. Normal range of anti-thyroid peroxidase antibody was < 34U/ml. Out of 50 patients, 34 patients (68%) found high anti-thyroid peroxidase antibody titre >34 U/ml (Figure 3). Our results are similar with previous study (Table 1).

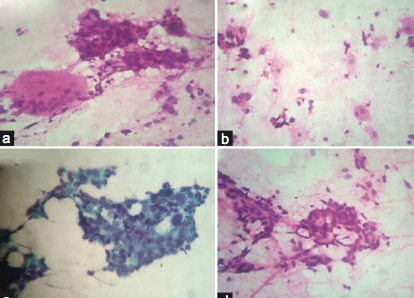
FNAC was done in all patients and cases reported according to "The 2017 Bethesda System for Reporting Thyroid Cytopathology (TBSRTC)". All cases were categorised in Bethesda category 2. Thyroid smears with good cellularity, presence of 6 cell groups with atleast s10 thyroid follicular cells in each group, were defined as adequate smears. This constituted to all 50 cases. Cytomorphology revealed cellular smears & showed follicular cells in groups, clusters and flat monolayered sheet against a hemorrhagic background. Follicular cells were showing finely granular cytoplasm, mild nuclear atypia, vesicular chromatin and inconspicuous to conspicuous nucleoli. Fair number of follicular cells are showing marginal cytoplasmic vacuoles with pink red frayed edges.
Cytomorphology revealed moderate to high cellularity in 44 cases (88%) and low cellularity in 06 cases (12%). Most frequent cellular pattern was small to large flat monolayered sheet in 43 cases (86%), micro or macrofollicular pattern in 31 cases (62%) and 13 cases (26%) showed avascular papillary infoldings. Mild to moderate nuclear anisokaryosis found in 43 cases (86%) and marginal vacuoles; fire flares in 41 cases (82%). Lymphocytic infiltrate was found in 12 cases (24%), epithelioid cell granuloma in 07 cases (14%), multinucleated giant cells in 05 cases (10%) and pseudo giant cells in 04 cases (08%). Background colloid was scant or minimal in 44 cases (88%) and abundant colloid seen in only 06 cases (12%) (Figure 4, Figure 5, Figure 6).



Hemi-thyroidectomy or thyroid lobectomy was done in only 2 cases with diffuse enlargement of thyroid gland. Histopathology revealed hyperplastic thyroid follicles with focal papillary infoldings and vascular congestion. Follicles were lined by tall columnar to cuboidal follicular cells exhibiting vacuolated cytoplasm, finely granular cytoplasm, mild to moderate nuclear anisokaryosis, vesicular chromatin and inconspicuous to conspicuous nucleoli. Numerous follicles were showing colloid reabsorption droplets. At places stroma were showing patchy lymphoid infiltrate (Figure 7, Figure 8).


Discussion
The average age of onset is between thirty and fifty years of age, the commonest age group to be the 3rd to 4th decade 18. In our study most cases fall in between 18 to 40 years, with female predominance. This increase in incidence has been linked to excess iodine intake and residence in nearby industrial area 19. The ratio of total T3 to total T4 is commonly used for differentiating the etiology of thyrotoxicosis between GD and subacute thyroiditis. The ratio of T3 to T4 was useful for distinguishing the cause of thyrotoxicosis. The low sensitivity of the cutoff value of T3/T4 ratio, we chose to use high specificity for the diagnosis of GD 20. FNAC is highly sensitive in diagnosing GD, by characteristic features of mononuclear cells infiltrate consisting of lymphocytes, plasma cells, histiocytes impinging on follicular cells, multinucleated giant cells and hurthle cell change with a diagnostic accuracy rate of 92%. Diagnosis of GD is likely to be missed in cases of nodular goiter that can be differentiated by the absence of multinucleated giant cells and epitheliod cells and lymphoid cells impinging on follicular cells 21.
Anti-TPO antibodies are the most common anti-thyroid autoantibody, present in approximately 90% of Hashimoto's thyroiditis, 75% of GD and 10–20% of nodular goiter or thyroid carcinoma 22.
|
S.No. |
Researcher Team |
Anti TPO Positive High (>34 U/ml) |
Anti TPO Negative Normal (< 34 U/ml) |
|
1. |
Carvalho et al., 2013 23 |
80% |
40% |
|
2. |
Samsudin et al., 2014 24 |
62% |
38% |
|
3. |
Almomin et al., 2019 25 |
60.4% |
39.6% |
|
4. |
Siriwardhane et al., 2019 26 |
59.8% |
40.2% |
|
5. |
Sulejmanovic et al., 2020 27 |
71% |
29% |
|
6. |
Alhubaish et al., 2023 28 |
58.9% |
41.1% |
|
7. |
Current Study 2023 |
68% |
32% |
Carvalho et al., anti-TPO Abs were present in about 80% of patients, 23 Samsudin et al., anti-TPO Abs were present in about 62% of patients, 24 Almomin et al., 2019 anti-TPO Abs were present in about 60.4% of patients, 25 Siriwardhane et al., anti-TPO Abs were present in about 59.8%. of patients, 26 Sulejmanovic et al., anti-TPO Abs were present in about 71% of patients, 27 and Alhubaish et al., anti-TPO Abs were present in about 58.9% with GD 28 .
GD is revealed by presence of hypercellular colloid free smear showing columnar type follicular cells in monolayered sheets. Cytoplasm is abundant, vacuolated with larger marginal vacuoles (fire flares). Hurthle cells, lymphocytes and multinucleated giant cells are rarely seen and have done cytological grading on FNAC smears for the first time using predefined sets of criteria, where they tried to correlate the lymphoid density withclinical, radiological and biochemical parameters 29. The importance of presence of eosinophils and high eosinophil: neutrophil ratio for making diagnosis of GD and to differentiate it from colloid goiter 30. It is important to diagnose GD because patients subsequently become hypothyroid and require lifelong thyroxine supplementation, genetic factor and environmental factors such as iodine intake, exposure to certain drugs, smoking habits, stressful life events and a number of infectious agents have all been found associated with GD 31. It could have been better if we had done US and computed tomography (CT) scan guided FNAC that have a higher probability of higher accuracy along with any wet stain (H and E, Pap stain).
Conclusion
A correct cytological diagnosis was achieved in the majority of cases and rejecting the need for a surgical intervention and provided lifelong hormonal therapy in justified cases. A careful and diligent search for various cytological features and accurate sampling can help in reducing the number of indeterminate, false-positive and false-negative diagnoses. FNAC is highly sensitive and specific technique in diagnosing GD and other types of thyroiditis. Patients with high serum anti-TPO levels seem to be at an increased risk and require frequent evaluation. Further well-designed larger community studies are required to have a clearer picture of the current situation.