Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 42-46
Original Article
N R Ramesh Masthi1, S Pruthvi2
1Professor& Head, Department of Community Medicine, Kempegowda Institute of Medical Science & Research Centre, 560018, Bangalore,
2Assistant professor, Sapthagiri Institute of Medical Science & Research Centre, 560090, Bangalore
Address for correspondence: S Pruthvi, Assistant professor, Sapthagiri Institute of Medical Science & Research Centre, 560090, Bangalore. E-mail: [email protected]
Background: The high incidence of mortality and morbidity among infants and children is attributed largely to unsafe water supply, poor hygienic practice and insanitary environment. Anganwadi are the backbone of non formal education in rural India and place for inculcating healthy habits for children at an early age. Objectives: To assess the environmental sanitation of Anganwadi Centers, to describe personal hygiene of preschool children in Anganwadi and to assess personal hygiene practices of Anganwadi staff. Materials and methods: A cross-sectional study was conducted among Anganwadis located in the rural field practice area of a medical college, Bangalore over a period of two months. Anganwadi teachers, helpers and workers were interviewed through pre tested, semi structured questionnaire regarding their awareness on personal hygiene practices. Anganwadi children were examined for personal hygiene and morbidities. The Anganwadi centers environmental sanitation was assessed by observation. Results: 50 Anganwadi centers were visited. 45(90%) anganwadi center’s vessels and kitchen were kept clean. Lighting was adequate in 43(86%). 32(64%) Anganwadis had sanitary latrines. House hold purification of water was seen in 33(66%) anganwadi’s. Out of 1113 children registered, 689(61.9%) were examined. 479(69.5%) were found to be bare foot walkers, 55(7.9%) had poor face hygeine, 24(3.4%) poor hair hygeine, 95(13.78%) poor oral hygiene, 15(2.17%) poor feet hygeine, 51(7.4%) poor nail hygiene. Conclusions: The environmental sanitation of Anganwadi centre and personal hygiene status of children was not satisfactory.
Keywords: Morbidity, Formal education, Hygiene, Anganwadi, Sanitation
Children grow and develop amazingly. Mothers with their children under five years of age, not only constitute a large proportion of the community but also a “vulnerable” or special risk group. The first five years of a child’s life are most crucial for the foundations for physical and mental development.[1] India has an Under 5 mortality rate of 56 and an aggregate child population of 158.78 million according to census 2011.[2] 32.9% of children below 5yrs were found to be underweight according to National Family health survey-5 (NFHS-5) in Karnataka.[3]
To address the growing concerns of malnourishment, childhood mortalities and morbidities, Integrated Child Development Services (ICDS) was introduced in 1975 which became functional through a vast network of ICDS centres known as Anganwadis. The word Anganwadi is derived from “angan” which means courtyard, where most of the social activities of household take place (4). These anganwadis addressed the holistic requirements of Under-5, adolescent girls, expectant and nursing mothers.[4]
The key functionary of ICDS scheme is the Anganwadi worker, an honorary worker who belongs to the community and caters to a population of ∼1000 people each.[5] The Anganwadi worker (AWW) is the community based voluntary frontline worker of the ICDS programme. Selected from the community, she assumes a pivotal role due to her close and continuous contact with the beneficiaries. Her educational level and knowledge of nutrition plays an important role related to her performance in Anganwadi centers. The output of ICDS scheme to a great extent depends on the profile of the key functionary that is Anganawadi worker, her qualification, experience, skills, attitude, training etc.[6]
In India, 14.6 lac Anganwadis are functional out of which 63,377 Anganwadi centers (AWC) belong to Karnataka.[7] Though the AWCs have been instrumental towards the inculcation of informal education, providing nutrition and nourishment of the mind, body, and soul of the children. Unsafe water supply, inadequate facilities, nonstrategic locations, poor hygiene practices, delayed incentives, lack of knowledge etc. have gradually handicapped the children with diseases and phobia towards Anganwadi centres leading to gradual loss of beneficiaries.
Most of the study concentrated on the nutritional and health status of the beneficiaries of ICDS. There are fewer studies elaborating on sanitation of Anganwadi centres. Less focus on assessment of personal hygiene practices among AWW who plays a pivotal role and status of personal hygiene of children. With this background the present study was conducted to assess the environmental sanitation of Anganwadi centres, to describe the personal hygiene status of children in Anganwadi centers and to assess personal hygiene practices of Anganwadi Staff.
A descriptive cross-sectional study was conducted in 50 Anganwadi centers coming under the rural field practice area of medical college near Bangalore for a period of 3 months. 50 Anganwadi centers teachers and helpers were selected using purposive sampling technique. All Anganwadi centres were visited in a period of 3 months. Anganwadi teachers (n-50) and helpers (n-50) were interviewed through pre tested, semi-structured questionnaire regarding their socio- demographic characteristics, awareness items on personal hygiene practices. Among 1113 children registered in Anganwadi centres, (n- 689) were examined for personal hygiene status. Awareness on personal hygiene practices to be followed among Anganwadi helpers & teachers were assessed. Environmental sanitation of Anganwadi centers was evaluated.
All Anganwadi centers that were open and available were included and children who were absent on day of study were excluded. Ethical committee clearance was obtained. Informed consent was taken from the participants and cooperation was obtained from all anganwadi teachers and helpers. The confidentiality of subjects as maintained. Data was presented in the form of excel sheets and analyzed using stata 12. The results are expressed in terms of frequency percentages and proportion.
Out of 50 Anganwadi centers visited, 1113 children were registered. 689(61.9%) were available and examined.
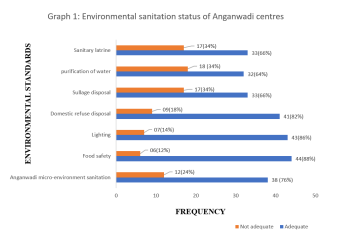
76% of Anganwadi centres had adequate micro environmental sanitation (frequency of floor, roof, windows cleaning, cleanliness of kitchen floor, stove and vessels). 88% had adequate food safety and 86% had adequate lighting. It was found that 32(64%) had a sanitary latrines which was well maintained and 33(66%) has good household purification of water as Implementation of IEC (Information, Education and counseling) materials was assessed with regard to non-formal education for children. 46(92%) Anganwadi centres had poor implementation of IEC materials with respect to non-formal education.
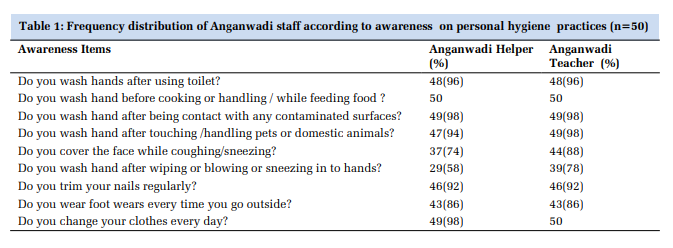
It was found that only 29(58%) Anganwadi helpers and 39(78%) Anganwadi teachers washed hands after sneezing, followed by 37(74%) Anganwadi helpers and 44(88%) teachers covered mouth while coughing and sneezing as shown in Table 1.
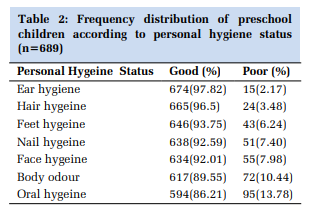
Table 2 represents the personal hygiene status of Anganwadi children. 689 children were assessed and majority 674(97.82) had good ear hygiene, 95(13.78%) of the children had poor oral hygiene. It was also found that 479(69.52%) were barefoot walkers. depicted in Graph 1.
On assessing the overall hygiene of Anganwadi workers and helpers, it was found that 13( 26%) helpers and 6(12%) teachers had poor cough etiquette practices and 21(42%) helpers and 11(22%) teachers didn’t practice hand washing after coughing and sneezing. Also, when the overall personal hygiene of the children was assessed it was found that 13.78% had poor oral hygiene, 7.98% had poor face hygiene, 6.24% had poor feet hygiene, 10.3% had body odour and 7.4% had poor oral hygiene.
Among 689 children examined 69.52% were bare foot walkers. 42(6.09%) of the children had morbidities (anaemia, diarrhoea, URTI, foot infection, skin wart, pityriasis alba, SAM & ear infection). URTI was commonest i.e 27(3.91%).
It was seen that 64% anganwadi centres had good??? Sanitary latrines similar to Hemamalini G et al (2018)[8] where 57.3% had sanitary latrine. Similar study by Sabat et al.[9] showed that 54.2% AWCs (n-24) were hygienic. 91.7% AWCs had good toilet facility corresponding to another study by Debata I et al.[10] where only 57% AWCs (n-21) were hygienic. Also, Malik et al[5] in his study concluded that 80% anganwadi methods to drain water were safe and hygienic. Toilet facilities were present in 88.9%, 55.6% and 85.7% of AWCs in project A, B, C respectively. A study by Chudasama et al.[11] in Gujurat, who assessed performance of Anganwadi workers in both urban and rural areas found that out of 46 rural Anganwadi centres, toilet facilities were available only in 32 (69.6%) centres.
On examining the overall environmental sanitation of Anganwadi centers, 76% centers had adequate sanitation on par with the study by Debata I et al[10] where 13 (61.9%) centres had good micro environment sanitation. Another study by Malik A et al[5] Study concluded that only 78% AWCs in his study showed adequate water storage and 14.6% AWCs had adequate lighting in contradictory to present study. A study by Nath, K.M et al[12] showed 20% of Anganwadi workers (n-60) practiced inadequate methods of purification of water more or less similar to the present study. Dhingra R et al also said 20% AWCs were surrounded with uncovered drain and 11% AWCs with stagnant water.
Similarly, another study by Hemamalini G et al[8] on assessing the KAP of Anganwadi workers on food safety said that 95% of the Anganwadi workers washed hands with soap and water before eating, while handling food and also after using the toilet in concordance with the present study.
46(92%) had poor IEC implementation with regard to non - formal education. Similar, to study by Debata I et al (10) where prominent display of charts, posters, boards etc in form of IECs were present in only 9 (42.9%) centres. It was also found that percentage of barefoot walkers were higher than seen in the study by Meena S et al (2015)[13] where 54.9% were barefoot walkers.
Another similar study done by Patel P et al (2013)[14] in Gujarat showed that 77.22% (41.01 females and 36.21% males) had poor overall hygiene and 72.46% ( 45.54% females and 26.92% males) had poor hygiene practices which were higher than reported in present study.
Hence, through this study it was observed that the overall environmental sanitation and maintenance of Anganwadis was not up to the expected standards, therefore, contributing to poor personal hygiene among AWCs children and poor personal hygiene practices among Anganwadi staff. Anganwadi centres being the focal points of policy convergence and implementation of policies for welfare of mother and children need to step up their will towards transformation of the community. This motive can only be recognized when the Anganwadi centres are treated like your house courtyard i.e. properly maintaining infrastructure, sanitation, and other microenvironment assets of AWCs.
The environmental sanitation of Anganwadi centres was not satisfactory. Personal hygiene status of children was not good. Awareness on personal hygiene practices by Anganwadi teachers and helpers were good.
Information bias from anganwadi workers with regard to awareness on personal hygiene practices followed. Was not able to assess the environmental sanitation standards in full like ventilation, macro environment. Intervention for implementation of IEC for non-formal education, awareness on personal hygiene practices to be followed among anganwadi workers was not done.
Emphasis pre-school children to wear foot wears. Well maintained water filters and sanitary latrine should be made available in all Anganwadi centres. Larger study with greater sample size to be done for generalization of results.
Subscribe now for latest articles and news.