Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i03.002
Year: 2017, Volume: 3, Issue: 3, Pages: 13-21
Original Article
Mustapha Kabir Musa1, Faisal Muhammad2, Kabir Musa Lawal3, A B M Alauddin Chowdhury2, Ahmed Hossain1
1Department of Public Health, North South University Dhaka 1229, Bangladesh,
2Department of Public Health, Daffodil International University, Dhaka 1207, Bangladesh,
3Department of Public Health, Northern University Bangladesh, Dhaka 1205, Bangladesh
Address for correspondence:
Faisal Muhammad, Department of Public Health, Daffodil International University, Dhaka 1207, Bangladesh. Phone: +8801723406483. E-mail: [email protected]
Background: Malnutrition is a major public health problem of developmental concern with both health and socioeconomic consequences. The study was aimed to determine the risk factors of severe acute malnutrition among under-five children.
Material and Methods: This hospital-based case control study was conducted from December 2015 to April 2016 whereby a total of 196 children under 5 years (98 cases and 98 controls) whose age ranged from 6 to 60 months were included in the study, data were collected retrospectively using a questionnaire, and mid-upper arm circumference (MUAC) was taken using standard procedures. SPSS statistical software version 19 was used to analyze the dataset.
Results: The mean ± standard deviation (SD) age of the cases and controls was 18.34 ± 14.6 and 16.93 ± 14.1 months, respectively, and the mean ± SD MUAC of the cases and controls was 9.36 ± 1.1 and 14.59 ± 2.2 cm, respectively. Risk factors associated with severe acute malnutrition were lack of taking balanced diet more than 3 times/day (adjusted odds ratio [AOR] = 5.355, 95% confidence interval [CI] = 1.162– 24.690), irregular hand washing with soap or other cleaning agents before feeding child (AOR = 0.317, 95% CI = 0.139–0.723), and father’s education level 0–8 class (AOR = 0.190, 95% CI = 0.054–0.676).
Conclusions: Severe acute malnutrition was found to be associated with father’s education level, lack of taking balanced diet, and irregular hand washing. Interventions to reduce malnutrition and address the factors contributing to malnutrition should be a policy priority.
KEY WORDS:Bangladesh, diarrhea, malnutrition, nutrition, public-health, under-five children
IntroductionChildhood undernutrition still remains one of the most serious public health problems in many countries, more especially low- and middle-income countries, and it has been reported that annually death of children in developing countries is about 1.7–3.6 million due to severe acute malnutrition (SAM) and moderate acute malnutrition, respectively.[1] Globally, it contributes to almost close to half of all child deaths, i.e.,, above 3 million children yearly.[2] SAM, which includes wasting (low weight-for-height or low mid-upper arm circumference [MUAC]) and nutritional edema, affects a small portion of numbers of children but is of particular concern as a result of high case fatality.[3,4] MethodologyTarget population and study site
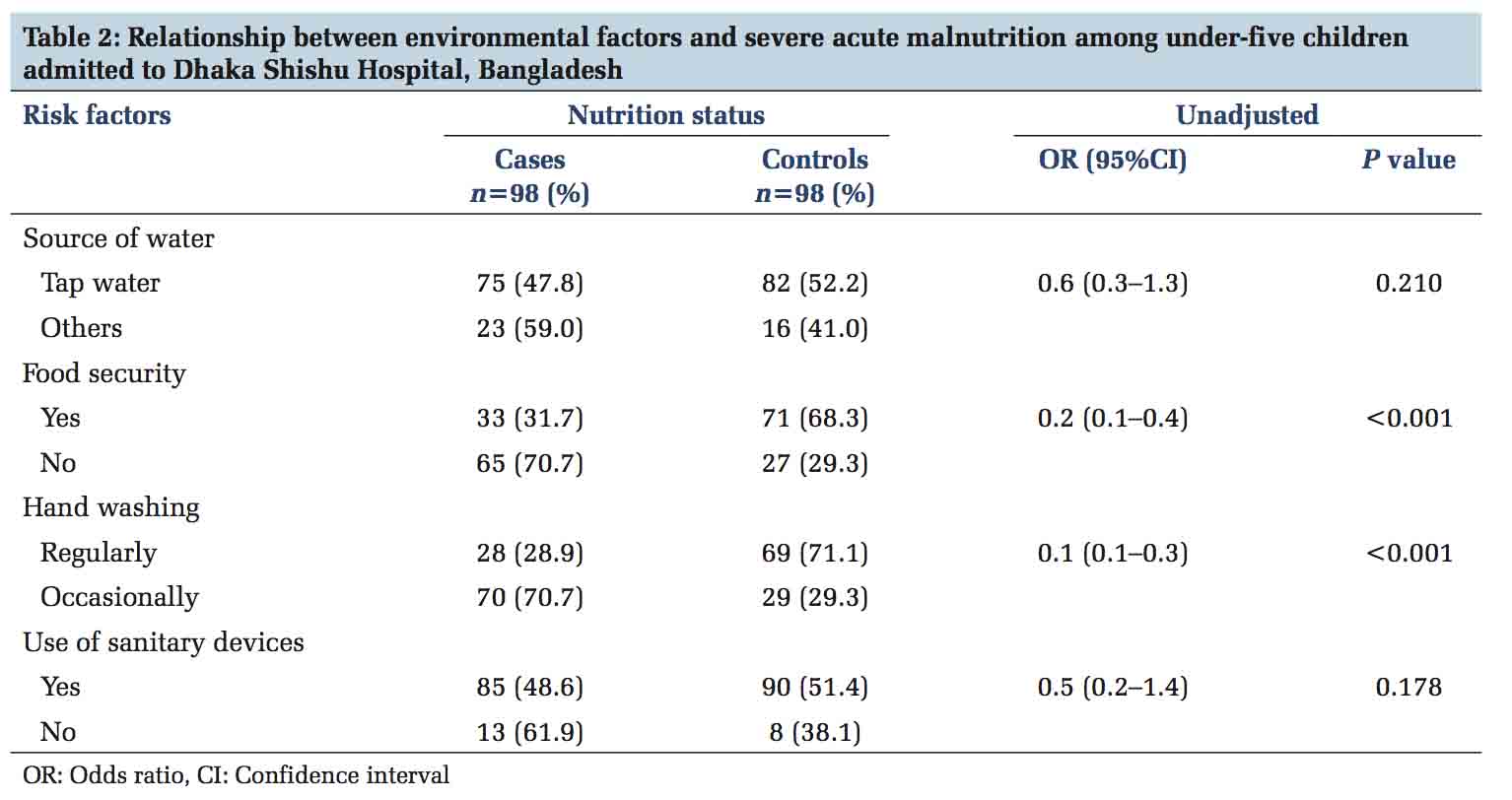
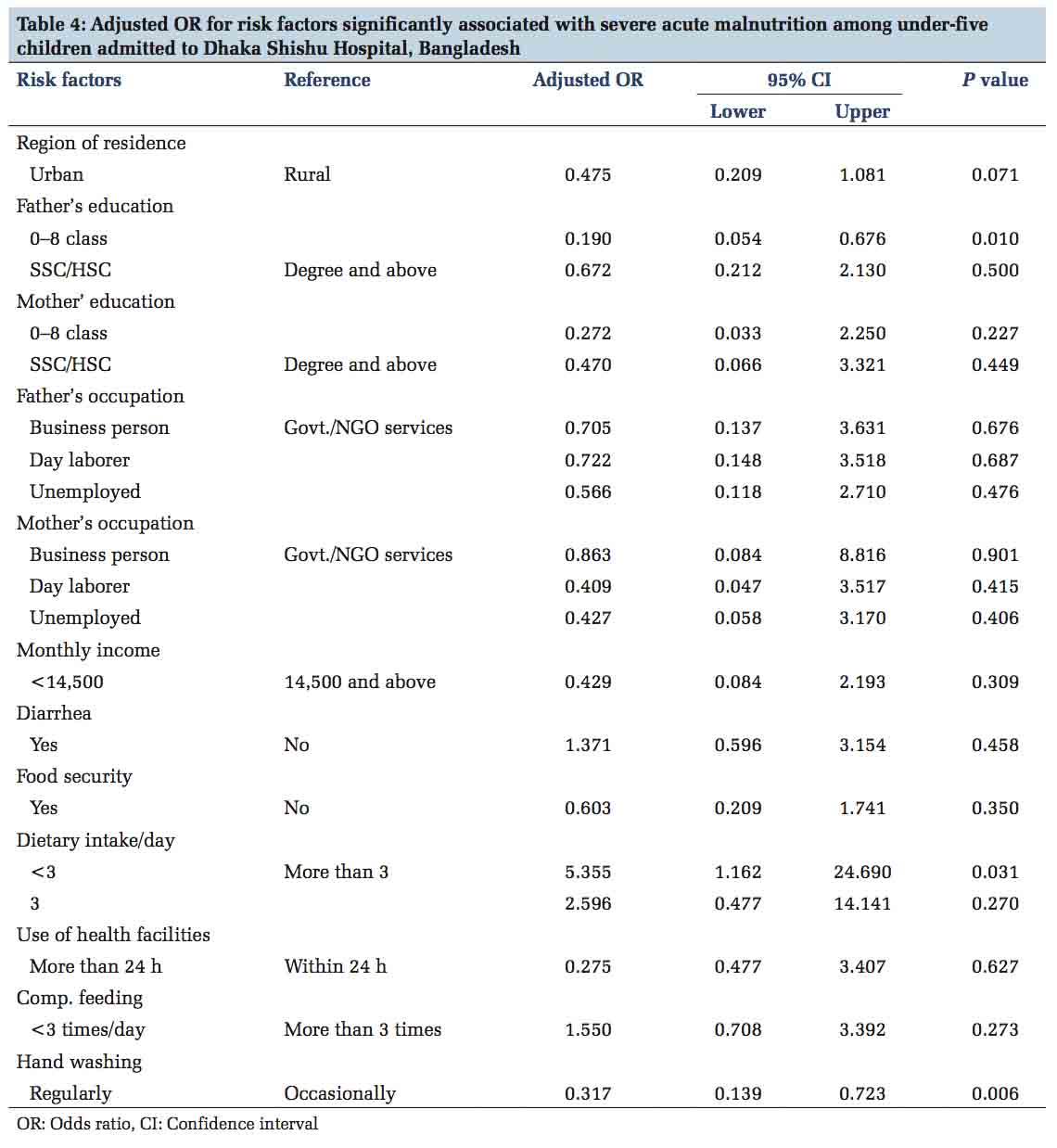
ResultsRelationship between sociodemographic factors and SAM among under-five children admitted to Dhaka Shishu Hospital, Bangladesh A total of 196 children were selected with an aim to determine the risk factors associated with SAM, among the children selected, 98 were cases and 98 were control. The mean ± SD age of the cases and controls was 18.34 ± 14.6 and 16.93 ± 14.1 months, respectively, and the mean ± SD MUAC of the cases and controls was 9.36 ± 1.1 and 14.59 ± 2.2 cm, respectively. Among the 196 children included in the study, 65.8% were males and 34.2% were females, 111 (56.6%) were in the age group 6–12 months, followed by 45 (23.0%) were 13–24 months and 40 (20.4%) were 25 months and above age group. However, there was no significant difference among thecasesandcontrolsassociatedwithagegroups 6–12, 13–24, and 25 and above months (P value 0.887 and 0.764, respectively) and sex of children (P = 0.500). Among the cases, 67.6% were living rural areas whileonly32.4%ofthecontrolswerefoundtobe livinginruralarea.Therewasasignificantdifference among case and control with regard to the region of residence (OR = 0.2, 95% CI = 0.1–0.4). Majority of the mothers, 58 (62.4%) of the cases and 35 (37.6%) of the controls, were housekeepers (day laborers). The main paternal occupation is rickshaw pullers (daylaborers)inboththecasesandcontrols(60.8% and 39.2%, respectively). There was a significant difference on the child SAM in cases and controls in relation to the mothers and fathers occupation (OR = 7.4, 95% CI = 1.5–36.5 and OR = 5.1, 95% CI = 1.8–14.2, respectively). Furthermore, mother of children with lower education (0–8 class) was significantly associated with SAM compared to those of mothers with degree and above education level (OR = 0.1, 95% CI = 0.03–0.7) [Table 1].Relationship between environmental factors and SAM among under-five children admitted to Dhaka Shishu Hospital, Bangladesh Majority of households got water from the public tap. There was no difference among the cases (47.8%) and the controls (52.2%) with regard to the source of water (OR = 0.6, 95% CI = 0.3–1.3; P = 0.210). Moreover, 48.6% households of the cases and 51.4% households of controls make use of sanitary devices, and there was no significant difference among the cases and controls associated with the use of sanitary devices (OR = 0.5, 95% CI = 0.2–1.4; P = 0.178). Food insecurity was found to be associated (P < 0.001) with SAM as only 31.7% of cases and 68.3% of controls were found to be food secured (OR = 0.2, 95% CI = 0.1–0.4). There was a significant difference among the cases 28.9% and controls 71.1% associated with regular hand washing before feeding children (OR = 0.2, 95% CI = 0.1–0.4; P < 0.001). Majority of cases 70.7% wash their hands occasionally before feeding their children [Table 2]. Relationship between proximal factors and SAM among under-five children admitted to Dhaka Shishu Hospital, Bangladesh Concerning the morbidity status of the children, 66.0% of the cases and 34.0% of the controls had diarrhea 2 weeks before the study. There was a significant association (P < 0.001) between severe wasting and the morbidity status by diarrhea (OR = 4.1, 95% CI = 2.2– 7.4). With regard to daily dietary intake, 72.7% of the cases had < 3 dietary intakes/day compared to 27.3% of controls group. There was a significant association (P = 0.001) between severe wasting and dietary intake < 3 times/day (OR = 3.6, 95% CI = 1.6–8.0). However, most of the mothers had mentioned that they took their child to the health facilities for treatment, only 33.3% of the mothers of cases and 66.7% of mothers of the controls were used to visit health facilities within 24 h of the onset of symptom. Children whose mothers do not take their children to the health facilities within 24 h of the onset of the symptom were associated (P < 0.001) with severe wasting of the child (OR = 3.7, 95% CI = 2.0–6.7). However, 40% of the cases and 60% of controls had practised optimal frequency of complementary feeding (≥3 times in a day). Suboptimal frequency of complementary feeding was also seen significantly associated (P = 0.001) with severe wasting of the children (OR = 2.5, 95% CI = 1.4–4.5) [Table 3]. The results of logistic regression showed that the risk of SAM was independently associated with lack of taking balanced diet >3 times/day (adjusted OR [AOR] = 5.355, 95% CI = 1.162–24.690), lack of regular hand washing with soap or other cleaning agents before feeding child (AOR = 0.317, 95% CI = 0.139–0.723), and father’s education level 0–8 class (AOR = 0.190, 95% CI = 0.054–0.676) after the effects of other significant risk factors were controlled [Table 4].
DiscussionIn this study, the educational level of the parents had a direct impact on the nutritional status of children. In the present study, it was observed that parent education had a significant effect on nutritional status of children. Aparent who had higher education might have more knowledge of a balanced dietary intake for the family in regard to improving the nutritional status of their children. Educational levels of parents in Ghana and India with severely malnourished children were lower than that of parents with healthy children.[13] Christiaenson and Alderson in 2001 found that female education had a positive and statistically significant effect on a child’s nutritional status. Education builds this consciousness among mothers, which increases the mothers and child healthcare seeking behavior. Mothers with post-secondary schooling had fewer malnourished children than mothers with primary and secondary schooling. Mother’s that were better educated fed their children better.[14]
ConclusionSAM is found to be associated with lack of taking balanced diet >3 times/day, irregular hand washing with soap or other cleaning agents before feeding child, and father’s education level.In this study, MUAC was found to be a very good screening tool. Thus, MUAC should be routinely measured as part of the clinical assessment of all children admitted to hospitals to find references/ cutoffs for different age groups. Interventions to reduce malnutrition and address the factors contributing to malnutrition should be a policy priority. Limitations
|
Subscribe now for latest articles and news.