Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i2.24.285
Year: 2025, Volume: 11, Issue: 2, Pages: 182-187
Original Article
Ranjan Agrawal1 , Naureen Ikram2 , Mudassir Aftab2 , Shashwat Verma3
1Professor & Head, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India,
2Resident, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India,
3Senior Resident, Pathology
Address for correspondence: Ranjan Agrawal, Professor & Head, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
E-mail: [email protected]
Received Date:28 April 2024, Accepted Date:23 November 2024, Published Date:18 June 2025
Background: Pancytopenia is a common hematological condition characterized by the simultaneous reduction in all three blood cell lines: erythrocytes, leukocytes and, thrombocytes. The present study investigates the etiology, clinical presentations, and outcomes of pancytopenia in patients admitted to the Rajshree Medical Research Institute in Bareilly, Uttar Pradesh, from June 2022 to May 2024. Material & Methods: All cases presenting with pancytopenia on peripheral blood were included in the study after IEC clearance. (IEC/IRB No: 035/2022) dated 10 September 2022. Patients refusing to give valid consent were left out from the study. Simultaneously, bone marrow examination and serum values were carried out to reach to a proper diagnosis. Results: A total of 88 cases of pancytopenia were analyzed, with important causes identified as megaloblastic anemia, aplastic anemia, malaria and hypersplenism. The study found a higher prevalence of pancytopenia in females as compared to the males, with the most affected age group being 10-20 years. Clinical presentations varied, with fatigue, pallor, and fever being the most frequent symptoms. Conclusion: The study highlights the importance of thorough clinical and laboratory evaluation to determine the underlying cause of pancytopenia and guide appropriate management and treatment strategies.
Keywords: Pancytopenia, Bone marrow, Megaloblastic Anaemia, Aplasia
Pancytopaenia is an important clinico-hematological feature encountered in routine medical practice. It is defined as simultaneous decrease in all three cell lines. It is characterized by the presence of anemia (Hb< 13.5 g/dLin males or 12 g/dLin females), reduced white blood cells (less than 4000/µL) and reduced platelets count below 140000/µL) resulting in decrease of all the three formed elements of blood below the normal reference range. 1, 2 It is thus, not a disease entity in itself but a triad of findings resulting from various underlying diseases that primarily or secondarily affect the bone marrow. 3, 4
Various hematological and non-hematological disorders may in any way affect the bone marrow either primarily or secondarily manifesting as pancytopaenia represented in the peripheral blood findings.5 The incidence of various hematological disorders resulting in pancytopaenia vary as per the geographical distribution and genetic predisposition of an individual. The disease pattern is also variable in different population groups owing to variations in their nutritional status and the infective disorders prevalent in that region. 6, 7
In view of the wide spectrum of aetiologies, the exact cause of pancytopaenia poses a great diagnostic challenge for the hematologists as well as the treating physician. Diagnostic clues obtained from haemogram and bone marrow examinations are useful in the early and timely diagnosis of diseases. Bone marrow examination and other specific biochemical
In India, especially in this region, the causes leading to pancytopaenia are not well delineated, so the present study was undertaken with the aim of observing the spectrum of Pancytopaenia in Rohilkhand region based on the clinico-hematological parameters of the patients.
The study was conducted in the Department of Pathology at Rajshree Medical Research Institute, Bareilly located in Western Uttar Pradesh. It was a hospital based prospective observational study of one and half year duration (October 2022 to March 2024) after obtaining IEC clearance (IEC/IRB No: 035/2022) dated 10 September 2022. It was a convenient sampling wherein all the cases befitting the inclusion and exclusion criteria were included in the study. Informed written consent was obtained in all the cases. Predesigned proforma for data collection was used. All patients clinically suspected and later hematologically proven to have pancytopaenia and who fulfilled the standard criteria such as – Hb levels in males <13.5 mg/dl and in females 12mg/dl, TLC<4000/µL and Platelet count of < 140,000/µL were taken into consideration. The total number of cases enrolled were 88. Patients of all age groups ranging from 10 years and above of either sex were included in the present study. Detailed relevant clinical history and physical examination was done in all the cases. Patients who were not willing to give consent, patients on chemotherapeutic, drugs and those who did not fulfill the above hematological criteria were excluded out from the study.
A thorough clinical history and detailed clinical examination was carried out on all the patients who presented to the pathology department with pancytopenia. In each case bone marrow aspiration was performed by the standard aseptic precautions. Wright stain was used to stain all the bone marrow smears. When required cytochemical stains such as Periodic-Acid Schiff (PAS) and Myeloperoxidase (MPO) stains were also used. The necessary hematological and clinical parameters were noted. Besides the routine investigations other important investigations carried out included - complete blood count with special emphasis on hemoglobin, mean corpuscular volume (MCV), total and differential leukocyte counts, platelet count and, bone marrow examination with both aspiration and trephine biopsy procedures. Special stains in the bone marrow aspirate and biopsy were carried out as per the requirement of each case. Special investigations for individual disease entities including serum Vitamin B12 and folate levels for megaloblastic anemia, malaria card test, HPLC, blood culture to look for septicaemia, liver, and kidney function tests for confirming the etiology were also simultaneously carried out.
All the information collected were imported into the SPSS software version 23 for computing and standard deviations. Student’s t test was applied along with Anova test and chi – square tests. Ap value of ≤ 0.05 was considered as stastically significant. Correlation was analysed using Pearson’s correlation.
Statistical data of age group, genders, presenting complaints, different aetiologies of pancytopaenia, peripheral smear and bone marrow aspiration smears were studied, and compared with the previously published data. In the present study a total of 88 patients with 39 males and 49 females were included. There was a female preponderance with the male to female ratio of 1:1.26 (Figure 1).

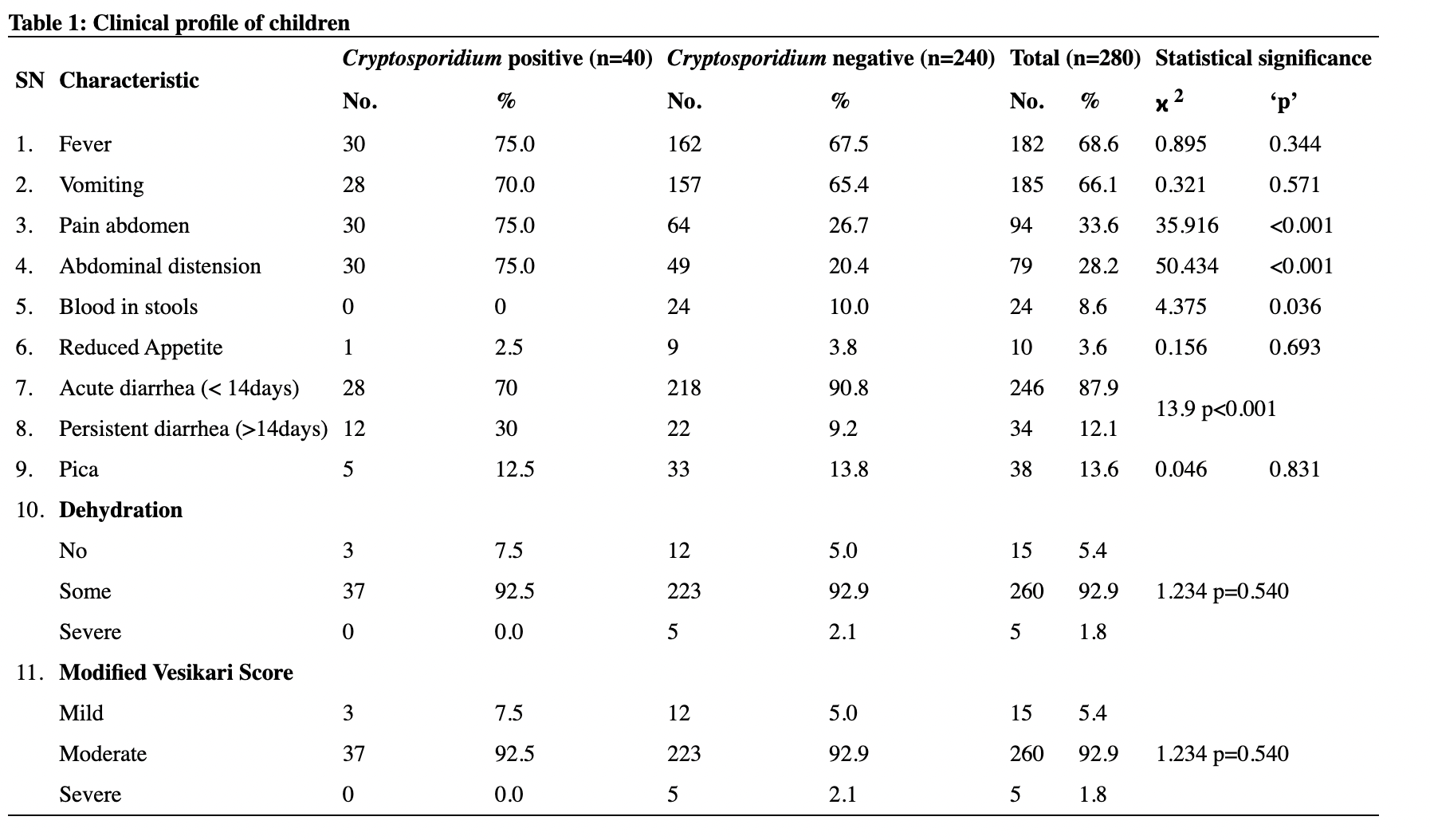
Majority of the patients belonged to the age group of 10-20 years with 25 (39.1%) cases (Table 1) in it. The most common presenting feature in majority of the patients was lethargy in 60 (68.2%) cases, followed by dyspnoea breathlessness in 48 (54.5%). (Table 1) Many of the patients had multiple complaints. Varied clinical presentations were observed in 60 of the 88 (68.2%) patients. Bleeding manifestations were reported in 32 (36.3%) of the patients. The various symptoms and clinical presentations have been mentioned in Table 1.
|
Presenting Complains |
Present (%) |
Absent (%) |
Clinical findings |
Present (%) |
Absent (%) |
|
Lethargy |
60 (68.2) |
28 (31.8) |
Pallor |
60 (68.1) |
28 (31.8) |
|
Dyspnea |
48 (54.5) |
40 (45.5) |
Bleeding manifestations |
32 (36.3) |
56 (63.6) |
|
Abdominal pain |
38 (43.2) |
50 (56.8) |
Icterus |
25 (28.4) |
63 (71.5) |
|
Fever |
35 (39.8) |
53 (60.2) |
Pedal edema |
22 (25.0) |
66 (75.0) |
|
Loss of appetite |
28 (31.8) |
60 (68.2) |
Hepato-splenome galy |
10 (11.3) |
78 (88.6) |
|
Palpitation |
23 (26.1) |
65 (73.9) |
|
|
|
|
Headache |
15 (17.0) |
73 (83.0) |
|
|
|
|
Generalized body ache |
12 (13.6) |
76 (86.4) |
|
|
|
|
Vomiting and diarrhoea |
10 (11.4) |
78 (88.6) |
|
|
|
|
Vomiting and diarrhoea |
10 (11.4) |
78 (88.6) |
|
|
|
Mild degree of anaemia was noted in 35 (39.7%) of the patients, while severe degree of anaemia was reported in 25 (28.5%). Majority of the patients presented with mild degree of leucopaenia. Mild Thrombocytopaenia was also observed in majority of the patients (Table 2). The distribution of the aetiology of pancytopaenia is tabulated in Table 3. Use of special tests helped in the diagnosis of several specific disease entities.
|
Haemoglobin (in gm/dl) levels |
n |
% |
WBC Count |
n |
% |
Platelet count |
n |
% |
|
< 5 |
25 |
28.5 |
1000 - 2000 / µl |
17 |
19.3 |
< 10,000 / µl |
12 |
13.7 |
|
05-Jul |
28 |
31.8 |
2001 - 3000 / µl |
32 |
36.4 |
10,000 - 50,000 / µl |
34 |
38.6 |
|
08-Oct |
35 |
39.7 |
30001 - 4000 / µl |
39 |
44.3 |
50,001 - 100,000 / µl |
36 |
40.9 |
|
Total |
88 |
100 |
Total |
88 |
100 |
> 100,000 / µl |
6 |
6.8 |
|
|
|
|
|
|
|
Total |
88 |
100 |
|
Mean ± SD: 5.84 ± 1.94 gm/dl, |
Mean ± SD: 2875.6 ± 782.5 per µl, |
Mean ± SD: 51,500 ± 30694 / µl, |
||||||
|
Minimum: 1.8 gm/dl, |
Minimum: 1000/µl, |
Minimum: 2000/µl, |
||||||
|
Maximum: 9.9 gm/dl |
Maximum: 3860/µl |
Maximum: 130,000/µl |
||||||
|
Diagnosis |
Age groups (Years) |
||||||
|
Oct-20 |
21-30 |
31-40 |
41-50 |
>50 |
Total n |
% |
|
|
Megaloblastic |
12 |
7 |
7 |
4 |
2 |
32 |
36.4 |
|
anaemia |
|||||||
|
Aplastic anaemia |
5 |
2 |
5 |
4 |
1 |
17 |
19.3 |
|
Malaria |
5 |
2 |
2 |
4 |
3 |
16 |
18.2 |
|
Dimorphic anaemia |
1 |
2 |
2 |
1 |
2 |
8 |
9.1 |
|
Acute leukaemia |
1 |
2 |
1 |
NIL |
NIL |
4 |
4.5 |
|
Dengue fever |
1 |
1 |
1 |
NIL |
1 |
4 |
4.5 |
|
Typhoid fever |
NIL |
2 |
1 |
1 |
NIL |
4 |
4.5 |
|
Chronic liver disease |
NIL |
NIL |
1 |
1 |
NIL |
2 |
2.3 |
|
Alcoholic liver |
NIL |
1 |
NIL |
NIL |
NIL |
1 |
1.2 |
|
disease + megaloblastic |
|||||||
|
Total |
25 |
19 |
20 |
15 |
9 |
88 |
100 |
Megaloblastic anaemia resulting in pancytopaenia is a frequent observation seen in 32 (36.4%) patients. It is also observed that the younger or age group is affected more frequently rather than the elderly. Multiple myeloma, however, is observed in the elderly age group (Table 3). Malaria is another important cause of pancytopaenia. Alcohol induced megaloblastic picture is also known. The second and third common causes of pancytopaenia included Aplastic anaemia followed by malaria, comprising 17 cases (19.3%) and 16 (18.2%) respectively.
Pancytopaenia is a common haematological finding observed in routine diagnostic practice and should always be suspected in patients that present with features such as unexplained anemia, prolonged fever, and tendency to bleeding. Manifestations of anaemia such as weakness, malaise, dyspnoea on exertion or even on rest along with palpitation are important features that need to be documented. Besides, other findings observed included a female preponderance in our study that could be attributed to dietary restrictions in some selected villages. Petechial rashes, bruising, bleeding gums and, increased susceptibility to infections were other observations depending on the predominant cell lines that were deficient. 8, 9
Family history, drugs or radiation, exposure can lead to pancytopaenia. Approximately half of the cases are categorised idiopathic, in which the exact etiology of pancytopaenia remains undiagnosed or undetected. 2, 3, 10, 11
Pancytopaenia is not a disease in itself but is rather a triad of haematological findings that may result from a number of underlying disease processes. 12 Early and prompt diagnosis of different etiologies of pancytopaenia is very crucial and requires prompt clinical examination and investigations such as complete blood count, peripheral smear and bone marrow examination. Bone marrow cellularity and composition in pancytopaenia differs in relationship to the underlying disease entity. The marrow is mostly hypocellular in most of the patients with pancytopaenia as a result of defect in production of cells. 5, 13, 14, 15
Megaloblastic anemia is an important and major cause of pancytopaenia as a result of under nutrition especially in the underprivileged areas of India.16, 17 In megaloblastic anemia, hypercellular bone marrow was most common which was seen in 48 patients (81.3%). Hypersplenism results in peripheral collection and destruction of blood in the engorged splenic sinusoids resulting in pancytopaenia. Hypersplenism may occur due to congestive splenomegaly following liver cirrhosis or congestive cardiac failure, chronic malaria or thalassaemia. 5, 12 Viral hepatitis results in pancytopaenia for a short duration and is associated with bone marrow.
Septicaemia hypoplasia and typhoid are associated with pancytopaenia following bone marrow inhibition. 18 Acute leukemias may indicate bone marrow failure. Drug induced pancytopaenia are usually dose dependent or immune mediated. The usual drugs leading to pancytopaenia include Chloramphenicol, Cytotoxic drugs, NSAIDS, Sulphonamide, Antihypertensives Antithyroid drugs, Anti diabetic medicines, Azithioprine. 2, 12, 19 Malaria is one of the most common causes of pancytopaenia, accounting for nearly 30% of cases especially in falciparum variety. 20, 21 Miliary tuberculosis is an important cause of pancytopaenia in India. 18, 22, 23 According to Prem Kumar et al. in developing countries, pancytopenia is mostly attributed to infectious diseases such as tuberculosis and HIV, which poorly correlates with the present study 17. Cirrhosis of liver accounted for 4.7% of the cases which was not a notable cause in the other studies.
As per the previous published reports there has been a male preponderance. 1, 3, 10 The usual presenting symptoms in the present study were lethargy, dyspnea and fever. Weakness or lethargy being the commonest presentation has also been reported by previous authors. 1, 2, 8 Khodke et al in their paper reported that the common presentation was fever (40%) followed by weakness (30%) and bleeding manifestations (20%).5 9 patients (14.1%) presented with icterus probably because of hemolysis or following hepatocellular injury after malaria. An increase in the number of cases of aplastic anemia could be due to changes in the environment such as an increased exposure to the toxic fumes. Pallor is the most common manifestation as per the previous published literature. 7, 13 In the present study the mean value of haemoglobin was 5.84 ± 1.94 g/dL. Similar findings have been observed by some other authors as well.2, 4, 21 On the contrary some authors observed a higher haemoglobin levels. 4, 6 The mean Hb, TLC and platelets according to etiology were analysed. It was found that the least mean Hb was found in hemolytic anemia. In this study, peripheral blood smear examination study was carried out in all the cases presenting with pancytopenia. The most common RBC morphology was normocytic normochromic picture.
Pancytopaenia as a result of chronic liver disease was reported in 2.3% of cases. Osama ishtiaq et al in their publication reported that liver cirrhosis leading to hypersplenism followed by pancytopaenia is observed in nearly 12% of the cases. 24 Difference in the frequency of disease that led to pancytopaenia has been attributed to variations in the methodology, advanced diagnostic modelities, geographic distribution, study period, genetic differences, and exposure to toxic or chemotherapeutic drugs. The variation in the frequency of the causes of pancytopenia has been attributed to the differences in methodology and stringency of diagnostic criteria, period of observation, varying exposure to cytotoxic drugs apart from the geographical area and genetic mutations 12, 18 . Screening programs at the community or mass levels do help in diagnosis and benefit avoiding further complications by offering adequate patient counseling, especially for anemia 4, 21. The variation in causes of pancytopenia observed among various studies could be due to differences in methodology as to which type of patients were recruited (eg. outdoor vs indoor), dietary and environmental factors as prevalence of tropical infections vary according to the geographical area.
There has been no study of this type conducted in this part of the country so far. It was a useful study since the geographical distribution as well as the pattern of pancytopenia could be understood better. However, the number of cases was a limitation and the observations obtained could have been better correlated with more number of cases.
Pancytopaenia is a common manifestation seen in routine haematological reporting. It poses diagnostic difficulty both for the reporting pathologist as well as the treating physician. The outcome depends on the presentation according to the underlying etiology and its severity, so it may vary from one patient to another.
Diagnosis of pancytopaenia requires a combination of multiple investigations. A single test usually does not help in arriving at the correct diagnosis or the pathology. The overall outcome and future management depend on the cause and presentation of the patient. Thus, an early and correct diagnosis is important in all the patients presenting with pancytopaenia.
To conclude, this study has helped us in knowing the various causes of pancytopenia in this region.
Subscribe now for latest articles and news.