Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.3
Year: 2025, Volume: 11, Issue: 1, Pages: 86-90
Original Article
Sabiha Tasneem Shaik1 , Chaitanya Latha Sappidi2 , Gudeli Vahini3
1Postgraduate, Department of Pathology, Alluri Sitaramaraju Academy of Medical Sciences, Eluru, Andhra Pradesh,
2Assistant Professor, Department of Pathology, Alluri Sitaramaraju Academy of Medical Sciences, Eluru, Andhra Pradesh,
3Professor & HOD, Department of Pathology, Alluri Sitaramaraju Academy of Medical Sciences, Eluru, Andhra Pradesh
Address for correspondence:
Gudeli Vahini, Professor & HOD, Department of Pathology, Alluri Sitaramaraju Academy of Medical Sciences, Eluru, Andhra Pradesh.
E-mail: [email protected]
Received Date:05 January 2024, Accepted Date:26 September 2024, Published Date:27 February 2025
Introduction: Multiple myeloma is a disorder caused by neoplastic proliferation of malignant plasma cells. It comprises about 15% of all hematologic malignancies and contributes to 1% of cancer deaths. Its incidence is higher in males with a peak age of incidence of 65-70 years. Objective: To study the incidence of multiple myeloma and to correlate with clinical, Biochemical, Radiological, hematological and Bone Marrow findings. Methods: This was a record based retrospective study conducted over a period of 1 year in Alluri sitaramar aju Academy of Medical sciences. Patients admitted in medical wards with features of anemia, bone pains, lytic bone lesions and renal failure were included. Hematological investigations such as Hemoglobin (Hb) estimation, total and differential cell counts, erythrocyte sedimentation rate (ESR), platelet count, peripheral blood smear, bone marrow examination was done. Urine examined for Bence Jones protein. Serum protein electrophoresis to detect M band, serum beta microglobulins, serum albumin was done in all cases. Radiological investigations included skeletal survey, imaging studies like PET -CT, MRI were performed where indicated. Evaluation was done based on Revised international myeloma working group 2021. Results: This study includes 30 cases which were diagnosed in the one-year study period with majority people in seventh decade, age ranging from 38-72. There is male preponderance. Fever, fatigue, and anemia are seen in 97% cases (29/30), Bone pains seen in 83% cases (25/30), Lytic bone lesions with fractures seen in 67% cases (20/30), Renal failure on dialysis seen in 27% cases (8/30). Bence jones proteins seen in 13% cases (4/30), serum electrophoresis showing decrease in albumin levels seen in 20% cases (6/30), increased beta 2 micro globulin in 23% cases, serum LDH elevated in 16% cases, serum calcium elevated in 60% cases (18/30). Conclusion: Among 30 cases, most of these cases presented with varied clinical, Hematological, and radiological presentations. So, patients in old age with such varied presentations should be worked up to rule out multiple myeloma.
Keywords: Myeloma, Plasma cell, Males, Younger age, Serum electrophoresis, Fish
Multiple myeloma is a disorder caused by neoplastic proliferation of malignant plasma cells 1, 2, 3 . It comprises about 15% of all hematologic malignancies and contributes to 1% of cancer deaths 3, 4 . Associated with diverse translocation like IGH locus, frequent dysregulation, and overexpression of cyclin D, MAF, FGFR3, and deletion of 13q14.3 3, 5 .
To study the incidence of Multiple Myeloma and to correlate with clinical, Biochemical, Radiological and Hematological findings. The present study was undertaken to evaluate the clinicopathological profile of patients diagnosed as Multiple Myeloma on bone marrow aspiration or trephine biopsy.
This is a retrospective study conducted over a period of 1 year. Patients admitted in medical wards with clinical features of anemia, bone pains, lytic bone lesions and renal failure were included. The BMA and Trephine biopsy slides of the cases under study 4.Biochemical analysis with serum protein electrophoresis is done to detect M band. Serum free light chain assay along with serum beta 2 microglobulin, serum calcium and serum LDH are also taken for supportive information. Hematological investigations such as ESR, hemoglobin, total and differential cell counts, platelet count, peripheral blood smear, bone marrow examination was done. Radiological investigations including skeletal survey with imaging studies like PET-CT, MRI were performed wherever needed.
Patients presenting with myeloma defining events, diagnosed as multiple myeloma on bone marrow aspiration, biopsy as per Revised International myeloma working group 2014.
Patients who have not given consent were excluded from the study.
Total number of cases in our study were 30. Most common complaint of presentation in our study was fever, fatigue followed by anaemia. The duration of symptoms in our study was on an average of 5.4 months. Haematological investigations showed anaemia with Hb in the range of 5-7 gm% seen in most of these cases. ESR is raised in majority of patients to value as high as 140-160 mm/hr. Radiological examination revealed multiple lytic bone lesions in 67% cases, out of which 6 patients had pathological fractures involving the skull and spine. 2% of patients presented with osteosclerotic lesions. Raised serum LDH seen in 16% of cases. 27% of cases with renal failure on dialysis, increased serum creatinine was diagnosed with Multiple myeloma. Serum electrophoresis showing decrease in albumin levels with reversal of A/G ratio seen in 20% cases. Increased beta 2 microglobulin seen in 16% cases.

|
Clinical Features |
No. of patients |
Percentage |
|
Fever, Fatigue, Anaemia |
29/30 |
97% |
|
Bone pains / hypercalcemia |
25/30 |
83% |
|
Lytic bone lesions with fractures |
20/30 |
67% |
|
Renal failure on dialysis |
08/30 |
27% |
|
Percentage of plasma cells in bone marrow examination |
Number of patients |
Percentage |
|
10 - 30% |
03/30 |
10% |
|
31- 60% |
25/30 |
83% |
|
61 - 90% |
01/30 |
3.3% |
|
> 90% |
01/30 |
17% |
Cut off percentage of clonal bone marrow plasma cells >/= 10% as per revised international myeloma working group diagnostic criteria for multiple myeloma - 2014.


Plasma cell dyscrasias are a heterogenous group of disorders in which there is expansion and infiltration by clonal plasma cells and production of monoclonal immunoglobulin by neoplastic plasma cells 4, 5 . Plasma cell Dyscrasias Include Monoclonal gammopathy of undetermined significance (MGUS), Asymptomatic/symptomatic Multiple Myeloma, solitary Plasmacytoma of bone, Waldenstrom’s Macroglobulinemia (WM), Primary Amyloidosis and Heavy chain disease 4 . In the present study we have taken 30 diagnosed cases of multiple myeloma with varied presentations. Complaints related to end organ damage - lytic bone lesions, renal impairment, hypercalcemia, and anaemia etc. were considered in the study 6, 7 . In our study Male to female ratio is 2.75:1, with majority of patients males in the age group of 5th and 6th decade. There is involvement of younger age groups with one male patient of 38 years of age and another female patient of 36 years of age in our study. Rise et al observed similar findings in their study that plasma cell myeloma is more common in men than in women and average age was 54 years and 52 years 8, 9, 10 . The most common clinical feature was fever and fatigue (97% cases). These patients also gave a history of recurrent infections. 97% cases had anaemia according to criteria satisfying myeloma related tissue or end organ impairment (Hb < 10 g/dl) 11, 12, 13 . Anaemia was the most frequent alteration correlated with study done by Kyle in the mayo clinic (95%) 14, 15 . The presence of anaemia in patients results by replacement of bone marrow by neoplastic plasma cells or because of renal damage resulting from loss of erythropoietin 15, 16. Peripheral smear examination showed predominantly normocytic normochromic blood picture with few of them displaying leukoerythroblastic picture. Most of the cases diagnosed as myeloma had total leucocyte count within normal range and thrombocytopenia seen in some cases. Peripheral smear findings of our study results are on par with Ungari et al study 17 . However, our study showed leukopenia in 6% cases.
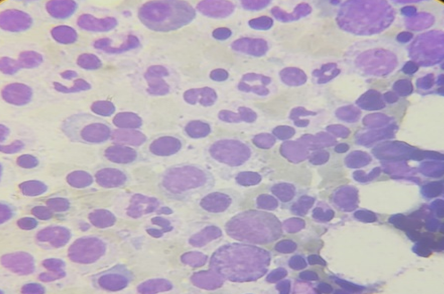
Bone marrow examination revealed an increase in plasma cells. These plasma cells are mono, bi, and multinucleate cells. Individual cells have cartwheel shaped peripherally pushed nucleus with amphophilic cytoplasm. Russell bodies, Dutcher bodies are also noted 18, 19. There is decrease in other series of cells in most of the cases. In our study 83% cases showed an increase in plasma cells in the range of 31%-60%. Bone marrow biopsy shows diffuse (80% cases), and nodular (14% cases) infiltration of neoplastic plasma cells seen. Renal failure with dialysis was seen in 27% cases, these patients are associated with increase in serum creatinine 20. This was again comparable to study done by Sindhu Sharma and my findings are on par with the study. Renal manifestations of plasma cell Dyscrasia are common, evident in approximately 25% of patients at the time of presentation and occur in 50% of patients at some point of disease. Renal involvement includes manifestations related to pathological immunoglobulin itself or to the toxic effect of the light chain 21 . As we know hypercalcemia is one of the diagnostic criteria laid down for MM, in our study also 60% cases presented with hypercalcemia which is due to either renal impairment or bone diseases (lytic bone lesions) 22, 23 . Lytic bone lesions seen in 67% of cases on X ray/CT, out of which 4 patients had vertebral bone fracture and 2 patients had femur fracture. The Pathogenesis of myeloma bone disease is due to imbalance between bone resorption and bone degeneration due to inhibition of osteoblast induced bone formation and increased activity of osteoclast 20, 21, 23 . Serum Electrophoresis in our study revealed increased IgG levels in 26 cases (90%) and increased IgM in 4 cases (9.0%) which is in contrast to the usual percentages observed in the literature wherein, IgG myeloma constitute 60% and IgM Myelomas are very rare. IgG is the most common type of Ig overproduced in multiple myeloma. IgA - second most common type of Ig overproduced in multiple myeloma. IgM - A rare type of Ig overproduced in multiple myeloma. When IgM is elevated in the blood, it could be a sign of Waldenstrom's Macroglobulinemia, a related disorder 2, 3 . Serum albumin is decreased in 20% cases with reversal of A/G ratio, Serum B2 microglobulin is increased in 23% of cases, Serum LDH is increased in 16% cases.
The increase in unbounded free light chains in the circulation is due to the secretion by the neoplastic plasma cells 24, 25. In present study 18/30 patients’ samples were sent for cytogenetic and FISH analysis to assess the prognosis in these patients. The panel was done for - Deletion 17p13, deletion 13q 14.3 t(IGH/FGFR3), t(IGH/CCND1), t (IGH /MAF). 45% of cases showed deletion of 13q 14.3, followed by t(IGH/CCND1) noted in 21% cases, 40% cases showed more than one cytogenetic abnormality26, 27. Based on the molecular findings attained on FISH can help identify high-risk patients who may need bortezomib-based therapy. FISH can also help identify standard-risk patients who can be treated with either immunomodulator- or bortezomib-based therapy 2 .
Among 30 cases in the present study, most of the cases presented with varied clinical, hematological and radiological presentations. So, patients with such varied presentations should be worked up bone marrow examination to rule out/confirm Multiple Myeloma. In possible cases the sample should be sent for molecular and cytogenetic analysis, as these are useful prognostic markers 26, 27, 28.
Subscribe now for latest articles and news.