Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i03.007
Year: 2015, Volume: 1, Issue: 3, Pages: 24-26
Case Report
Santosh Nagaraju1, Sakshi Vaishnav2, Aravinda K Nirmala3
1Fellow Transplant, Department of Surgery, Transplant division, 550 N, University Boulevard, Suite 4603, Indianapolis, IN 46202- USA,
2Fellow Nephrology, Department of Medicine, Nephrology division, 550 N, University Boulevard, Suite 4603, Indianapolis, IN 46202- USA,
3Resident, Department of General Surgery, Grant Medical College, Byculla, Mumbai, Maharashtra, India
Address for correspondence:
Santosh Nagaraju, Transplant division, 550 N, University Boulevard, Suite 4603, Indianapolis, IN 46202- USA. Tel.: 269-568-8868. Email: [email protected]
Primary sarcomas of the breast are rare tumors of mesenchymal origin. Owing to the rarity, clear consensus regarding diagnosis and management are lacking. Early and accurate diagnosis may help improve the outcome in patients with these tumors. Fine-needle aspiration cytology may not be able to diagnose sarcomas accurately, and tru-cut biopsy may be better at making the correct diagnosis of sarcoma. Surgical resection is the best available treatment option for breast sarcomas. Adjuvant and neoadjuvant therapy with radiation and chemotherapeutic agents are emerging options and are being evaluated. Certain aggressive subtypes like undifferentiated tumors progress rapidly and have poorer outcomes despite treatment. We report a case of a highly aggressive primary sarcoma of the breast in a 19-year-old girl.
KEY WORDS:Breast malignancy, primary breast tumor, sarcoma, surgical margins.
IntroductionSarcomas of the breast are rare, malignant tumors arising from the mesenchymal tissue of the mammary gland.[1] Breast sarcomas are broadly divided into three groups, (a) malignant phyllodes tumors, (b) sarcomas arising in breast that has received irradiation, and (c) primary breast sarcomas (PBS).[2] The incidence of PBS is reported to be as low as < 1% of all breast masses.[3] Owing to the rarity of occurrence, no clear cut directives exist for early diagnosis and management of PBS. Size of the tumor at the time of diagnosis is an important factor in predicting survival. Surgical resection with clear margins is also a very important predictor of outcome.[4] Adjuvant radiotherapy and chemotherapy are also important in the management algorithm of breast sarcomas.[5]
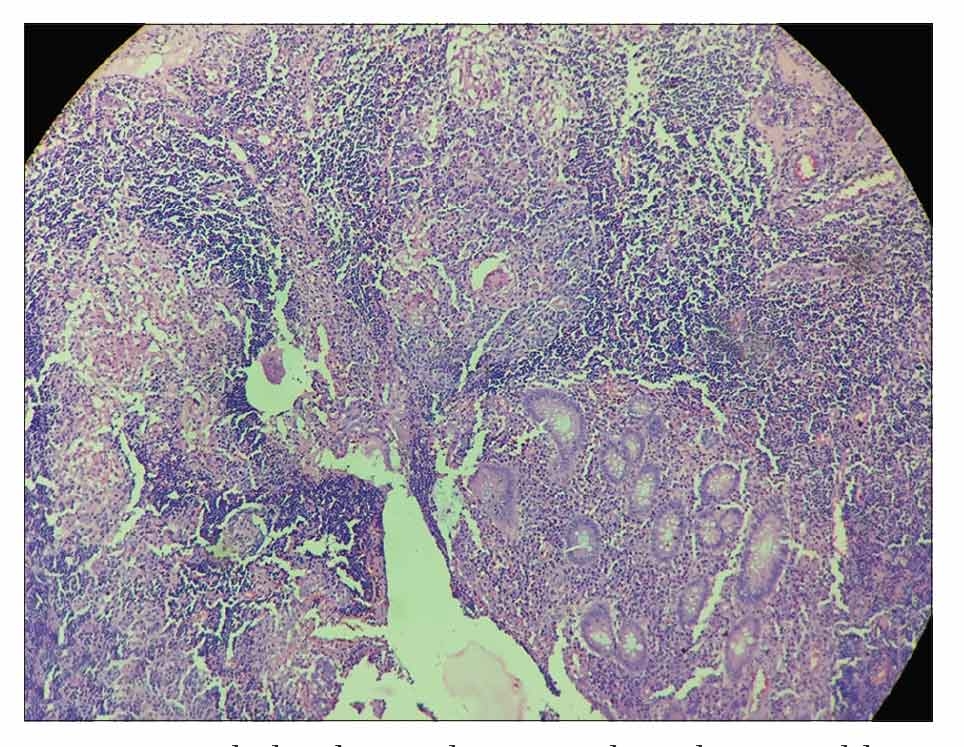
Case ReportA 19-year-old female patient presented with a fungating mass in the right breast, replacing the entire breast, since 15 days. The patient initially noticed a small lump in the right breast 2 months ago, for which she consulted a local physician, underwent fine-needle aspiration cytology (FNAC) and was diagnosed as fibroadenoma. The lump progressively increased in size and formed a fungating mass in 2 months. On examination a 25 cm × 22 cm × 14 cm fungating mass was noted (Figure 1). No axillary lymph nodes were palpable. Thorough investigations including tru-cut biopsy of the lesion, chest X-ray, computerized tomography of chest and ultrasonography of abdomen were done. No evidence of metastatic disease was noted in the chest or abdomen. A diagnosis of primary sarcoma of the breast was made and wide local excision with axillary sampling and delayed reconstruction of breast using ipsilateral latissimus dorsi flap was done (Figure2). Histopathology showed spindle cells arranged in whorl pattern, sheets, and fascicles. Individual tumor cells had moderate amount of cytoplasm, pleomorphic hyperchromatic nuclei. Mitotic activity was high (>10/10 HPF) abnormal mitosis and necrosis were noted. It was diagnosed as undifferentiated sarcoma of breast without lymph nodal involvement (Figure 3). 1 cm clear margin of resection was obtained all around. Patient recovery was uneventful and post-operative chemotherapy (vincristine and doxorubicin) and radiotherapy to the right side of the chest was initiated. The patient was discharged and advised to follow-up for therapy and assessment for breast implants subsequently. After 4 months, patient was re-admitted in emergency department with severe shortness of breath, fatigue and weight loss. Investigations revealed massive bilateral malignant pleural effusion with multiple lung metastases. The patient succumbed to her illness shortly afterward.
|
DiscussionSarcomas arising as a primary tumor are extremely rare.[3] Sarcomas arising in the breast are more common after exposure to radiation.[6] A variety of subtypes of sarcomas are seen, most common ones being -malignant phyllodes and angiosarcoma.[7] Owing to the rarity of its occurrence and fewer anecdotal reporting, the guidelines for management of sarcomas are vague. Early diagnosis, clear surgical margins of at least 1 cm and tumor size at the time of resection are the most important indicators of outcome. The commonly used approach of diagnosis of breast lumps with clinical exam and FNAC may not be enough to identify PBS. A high index of suspicion is required while evaluating breast lumps that are recurrent or atypical. PBS is easily confused with fibro adenoma on cytological analysis.[2] The consequences of such false diagnosis can be catastrophic, as exemplified in the present case. Tissue diagnosis by core biopsy supersedes FNAC in accurately identifying sarcomas.[8] Mammography or ultrasound imaging of the breast can have non- specific features and may not be conclusive.[9,10] Magnetic resonance imaging, however, is better at identifying suspicious lesions. Tumors are usually lobulated and have “washed out” appearance, - i.e., display rapid enhancement.[11] Surgical resection is still the best treatment option for PBS.[3] A tumor size < 5 cm at the time of resection has a better prognosis.[3,7] Clear surgical margin of at least 1 cm from tumor also is a favorable factor for improved outcomes.[3,7] Wide local excision is the procedure of choice, while large tumors may require a simple mastectomy to ensure adequate clearance of margin.[2] Axillary lymph node dissection is not warranted since sarcomas being mesenchymal in origin disseminate hematogenously.[2] Enlarged axillary nodes are usually reactive enlargements and rarely due to spread of the tumor. Complete axillary dissection has not been shown to be beneficial.[12,13] Adjuvant chemotherapy and radiotherapy are both a part of the treatment algorithm. Radiation to the affected site has been shown to improve survival rates in a study done at Toronto.[14] The beneficial effects of chemotherapy are advocated by some studies.[13] Despite advances in management, early and appropriate diagnosis is vital in attaining better outcomes in PBS. Delay in diagnosis coupled with aggressiveness of the tumor make a lethal combination and must be avoided. |
ConclusionPBS is rare entities and need a high index of suspicion for diagnosis. Fine-needle aspiration studies alone are insufficient to exclude sarcomas. Early diagnosis and surgical intervention may affect the outcome of the disease. Aggressive tumors rapidly progress and have a poor survival rate, despite therapy. |
Subscribe now for latest articles and news.