Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.001
Year: 2021, Volume: 7, Issue: 2, Pages: 7-12
Original Article
P V Dinesh1 , S V Bhargav2 , A G Kulkarni3
1 Associate Professor, Department of Community Medicine, KVG Medical College, Sullia, Karnataka, India,
2 Intern, Department of Community Medicine, KVG Medical College, Sullia, Karnataka, India,
3 Professor, Department of Community Medicine, East Point Medical College, Bengaluru, Karnataka, India Address for
correspondence: Dr. P V Dinesh, Department of Community Medicine, KVG Medical College, Sullia - 574 327, Karnataka, India. Phone: +91-9148217144. E-mail: [email protected]
Background: Malnutrition is not just a problem of rural population but also seen in urban children. Urbanization has significant implications on growth and development of children. The study was conducted in urban parts of Sullia Taluk, Karnataka, among preschool children going to Anganwadi to assess their nutritional status and also look for dental caries.
Materials and Methods: Two hundred and five children selected by simple random sampling technique were assessed for their nutritional status by anthropometric measurements and dental caries by dental examination.
Results: Among the 205 children, 61.95% were boys and 38.05% were girls. The proportion of children with wasting, stunting, and underweight was 14.63%, 30.24%, and 31.21%, respectively. About 43.90% of children in the study population had varying degrees of caries. There was no association between malnutrition and dental caries.
Conclusion: The study area is classified as a high to very high prevalence area for malnutrition according to the WHO.
KEY WORDS: Malnutrition, stunting, underweight, urban children, wasting.
Good nutrition is vital for any human’s cognitive and physical development. It has an impact on the quality of life. Although it is important throughout the course of an individual’s life, its importance is slightly more during early childhood period, as the rapidly developing brain during this period is more vulnerable to nutrient insufficiency.[1,2]
Child malnutrition generally occurs as a consequence of a combined effect of insufficient feeding practice and poor health for which there can be a variety of underlying causes ranging from mother’s own malnutrition to mother’s educational level, household poverty, poor water and sanitation, and lack of access to health services.[3]
Malnutrition is not just restricted to rural areas, but can be considered as an important public health problem even in urban areas as well, which officially may not be considered as poor. Urban India has 36.6 million children (28.5%) in 0–5 year’s age group. Malnutrition in urban areas may be due to a variety of factors like inadequate access to nutritious food which may be due to ignorance of the urban population or food habits like fast food culture. It may also be due to time constraints as this population has an ever busy working schedule. It may also be because there is an easy access to unbalanced packaged food. This kind of nutrition in children not only retards their growth but also causes tooth decay and makes them more prone to diseases because of weak immunity.[3,4]
Thus, this study is conducted in urban parts of Sullia Taluk, Karnataka, among preschool children going to Anganwadi for the assessment of their nutritional status by anthropometric measurements and dental caries by dental examination.
Anthropometric measurements such as weight, height, skin fold thickness, and mid arm circumference of each child were taken to assess their nutritional status. From the above measurements, weight for age, height for age, and weight for height were calculated.
Children were made to stand on the electronic weighing scale without touching anything. Heavy clothing and footwear if any were removed before weighing the child. Readings to the nearest of 0.1 kg were taken.[5]
Children were made to stand on the platform of a stadiometer without any footwear and with their feet parallel. The heels, buttocks, shoulders, and back of the head were made to touch the upright part of the stadiometer. The arms were made to hang on the sides and the head was held comfortably erect in the same plane as external auditory meatus. Height was taken to the nearest 0.5 cm with headpiece slightly crushing the hair and making contact with the top of the head.[5]
The instruments used for measuring height and weight were validated daily with known heights and weights.
Harpendens skin fold calipers were used to measure the triceps skin fold thickness.[6]
Mid upper arm circumference was measured in the left upper arm at the midpoint between the tip of the shoulder and tip of the elbow.[6]
Standard procedures as described by the WHO were used for dental caries examination.[7] Children were made to sit in a chair in front of the examiner. Cotton pellets were used to dry the teeth and natural day light and torch light were used for proper visibility. Sherpards probe 23 was used to assess caries. Caries with primary dentition was measured by the number of decayed, extracted, and filled primary teeth (DMFT). International caries detection and assessment system codes were used. The DMFT values were interpreted according to DMF scoring scale. A DMFT value between 0 and 4 was considered low caries, 5–9 as moderate caries and values greater than 9 were high caries.[8]
The data were entered into Microsoft Excel Office 2007 and analysis was performed using IBM SPSS statistics 20. The WHO Anthro software V 3.2.2 was used for anthropometric calculations.
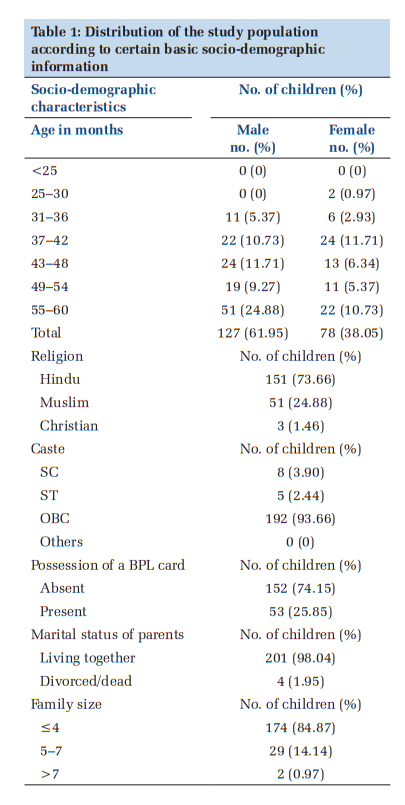
Two hundred and five children were selected from urban areas of Sullia Taluk, Karnataka by simple random sampling technique. Of them, 61.95% were boys and 38.05% were girls. Most of them (35.60%) belonged to 55–60 years of age group, belonged to Hindu religion (73.66%) and OBC caste (93.66%). Almost 84% of the children belonged to a nuclear family and in 98% of them; parents were living together with their children. A quarter of the families possessed a BPL card (Table 1).
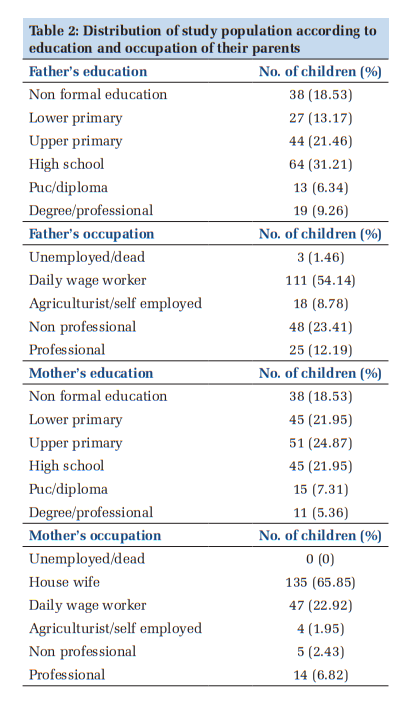
Most of the parents of the study population were educated till High school and were working as daily wage workers or were house wife as seen in Table 2. About 91% of the children in the study were either first or second born. About 3% of them were of the birth order of more than three. About 18.5% of the children involved in the study had experienced some illness in the previous 2 weeks before they were examined.
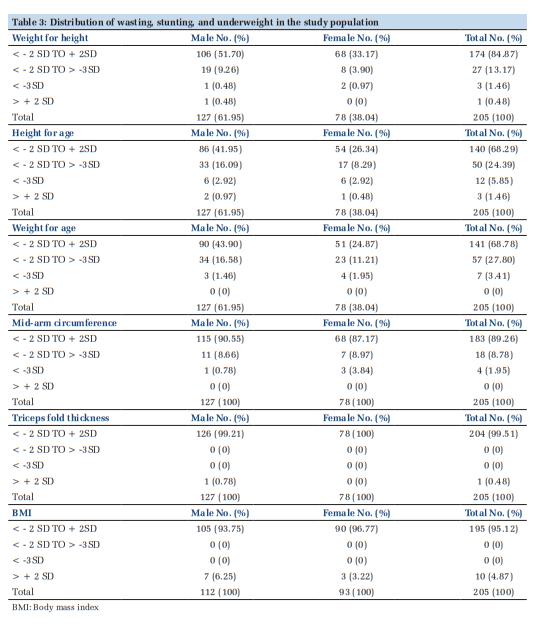
Of the total children, 9.26% of the boys and 3.90% of the girls had moderate wasting. The proportion of boys in the severe wasting category was slightly <0.5% and in girls, it was just <1%. A small proportion of boys (0.48%) and no girls were in the overweight category. Thus, 30 of the 205 children examined had decreased weight for height suggesting that 14.63% was the proportion of wasting seen in the study population (Table 3).
About 16.09% of the boys and 8.29% of the girls had moderate stunting. About 2.92% of the boys and the same proportion of girls had severe stunting. Of the 205 children, 62 of them had decreased height for age suggesting that 30.24% had stunting in total (Table 3).
About 16.58% of the boys and 11.21% of the girls belonged to moderate underweight category. About 1.46% of the boys and 1.95% of the girls were in severe underweight category. Thus, 64 children had decreased weight for age suggesting that 31.21% of the total 205 children belonged to underweight category. None of the children had increased weight for age suggesting that there are no overweight children (Table 3).
Most of the male and female children were normal when MUAC, triceps fold thickness, and body mass index (BMI) were taken into consideration for measuring malnutrition (Table 3).
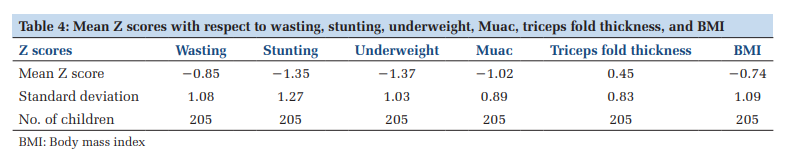
The mean z scores of almost all the parameters that were used to measure malnutrition were on the negative side except for triceps fold thickness (Table 4). The mean z scores were compared between boys and girls and it was seen that there was no statistically significant difference in wasting or stunting (Table 5).
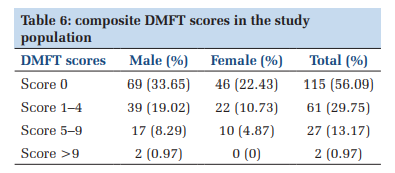
About 43.90% of children in the study population had varying degrees of caries (Table 6). To see if there was any relationship between dental caries and malnutrition, Pearson correlation was used.
It was seen that there was no correlation between malnutrition and dental caries in the present study, suggested by P = 0.40.
In the present study, nutritional assessment of 205 children going to Anganwadi in Urban Sullia Taluk of Karnataka was done using standard the WHO cut offs. Assessment of nutritional status of children is very important as this is an intervention point in the lifecycle of a person. Using different growth standards can give rise to differences in prevalence of nutritional status. It is, therefore, very important to use a single method all over the country to measure the nutritional status for comparability and uniformity.
In the present study, 64 (31.21%) children were underweight, 30 (14.63%) were wasted, and 62 (30.24%) children were stunted. When the present study is compared with NFHS 4 data of Karnataka,[9] it can be seen that 35.2% children were underweight, 26.1% children were wasted, and 36.2% were stunted. The results are almost comparable except for wasting where the present study population was found to be more wasted. A study done by Kumar et al. [10] showed that 10.6% of the children had wasting, 36.4% were underweight, and 51.6% were stunted. Kulwa et al. [11] found that among children of 6–24 months of age, 22% were underweight, and 3% were wasted. The wide variations in the prevalence of malnutrition can be attributed to variations in availability of food items, illiteracy rate, poverty, access to medical facility, and time period of data collection.
The prevalence of dental caries in the study population was 43.90% which is slightly lower when compared to a study done by Mehta[12] which showed the prevalence of dental caries among 2–5 year old children to be 48.90%. There are differences in the caries status among different populations. Probable reasons for such discrepancy could be inequality in economic conditions and resources, fluoridation policy, efficiency of health-care system, availability and consumption of refined sugars, oral health awareness among public, oral hygiene as well as motivational status of parents and children.
The present study did not show any relationship of dental caries with malnutrition. Fawaz et al. [13] showed that there was a positive relationship of dental caries with BMI for age. In contrast, a cross-sectional study of Iranian children showed no association between weight, height, and dental caries.[14] This result is similar to the finding of the present study where no association was found between BMI and dental caries. A possible explanation is that although both obesity and dental caries are often attributed to the high intake of carbohydrates and sugar, the true etiology of these diseases is much more complex and multifactorial.[15,16]

The commonly used methods for measuring nutritional status of children are weight for age, height for age, BMI for age, and weight for height. When weight for age is used as a measure, it will not be able to able to differentiate between current and past energy deficits. While stunting is an index of cumulative past energy deficit, it will not be able to reflect the current energy status, whereas BMI measures the current energy status. Thus, early detection of low BMI for age and its correction can be used for preventing stunting.
Subscribe now for latest articles and news.