Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.211
Year: 2025, Volume: 11, Issue: 1, Pages: 68-73
Original Article
Arpita Gogoi1 , P S Kirtheka2
1Associate Professor, Department of Pediatrics, Assam Medical College, Dibrugarh, Assam, India, 2Post graduate resident, Department of Pediatrics, Assam Medical College, Dibrugarh, Assam, India
Address for correspondence:
P S Kirtheka, Post graduate resident, Department of Pediatrics, Assam Medical College, Dibrugarh, Assam, India.
E-mail: [email protected]
Received Date:05 July 2024, Accepted Date:23 November 2024, Published Date:23 February 2025
Objective: The Pediatric Intensive Care Unit plays an important role in delivering demanding and required care to seriously ill children. The aim of the study is to determine the application of pSOFA scores as a predictor of outcome in children admitted to the pediatric intensive care unit. Methods: This was a hospital based cross sectional study conducted at the Pediatric Intensive Care Unit (PICU) of the Assam medical college and hospital from july 2023 to december 2023. Forty critically ill children from age one month to twelve years of either gender, admitted in PICU for more than 24 hours were included. The p-SOFA score was calculated for all eligible children at the time of admission. Data was analyzed using Statistical Package for the Social Sciences (SPSS) version 23. Results: The mean pSOFA score was found to be more in those participants who expired (10.86±1.35) compared to those who were discharged (3.79±2.64). This difference was found to be statistically significant. The pSOFA score was found to be more in non survivors compared to survivors which was statistically significant. Conclusion: The pSOFA score at the time of admission is a simple tool which is useful for predicting the mortality and outcome of the critically ill patients requiring PICU admission.
Keywords: Pediatric sequential organ failure assessment (p-SOFA), Pediatric intensive care unit, Mortality, Children, Organ dysfunction, Mortality prediction
Both in affluent and developing nations, there is a significant risk of morbidity and death for critically sick children admitted to the pediatric intensive care unit (PICU) 1 . To objectively measure the severity of the disease and estimate the probability of death at the time of PICU admission , a number of prognostic scores have been created. These scores can be very helpful in treatment planning. Furthermore, since a large portion of the variation in death rates between PICUs is determined by factors other than medical management, such as the primary diagnosis and illness severity at admission, such scores are crucial for evaluating the quality of medical care 2, 3 .
Organ malfunction is a stand-in for death in other scores. An excellent candidate marker of disease severity is multiple organ dysfunction syndrome (MODS), which is linked to a significantly higher risk of death. One study found that the mortality rate for MODS was 1% when one organ system was dysfunctional and could rise to 75% when four organ systems were dysfunctional. Mortality is frequently predicted using the Pediatric Risk of Mortality (PRISM), the Pediatric Index of Mortality (PIM), and their revised versions 4, 5 .
An accurate prognostic score should be simple, affordable, easy to use, and minimally invasive 6 . Nonetheless, there is presently no such ideal pediatric mortality prediction score, thus researchers are still working to increase the accuracy of the ratings that are now available and create new ones. The pediatric organ dysfunction scores include the Pediatric Logistic Organ Dysfunction Score(PELOD) 7 , PELOD-2, and Pediatric Multiple Organ Dysfunction Score (P-MODS) 8, 9 . The Sequential Organ Failure Assessment (SOFA) score, formerly known as the Sepsis-Related Organ Failure Assessment, is the score most frequently used to measure organ dysfunction in critically ill adults 10 .
According to the third International Consensus Definitions for Sepsis and Septic Shock [Sepsis-3]: sepsis diagnosis in adults is now thought to be closely related to the SOFA score 11 . Researchers are now keen to modify the SOFA for the pediatric population as a result of this. A pediatric variant of the SOFA score (pSOFA) was created recently and was verified in severely unwell children in the past 12 . The pediatric population, on the other hand, has little data available, and the pSOFA score has not yet been verified in low-income nations or through prospective cohort studies. This study's motive was to evaluate the prognostic value of pSOFA score in a diverse cohort of critically ill children in a nation with inadequate resources and ascertain whether the score can forecast the outcome.
The study was conducted after obtaining clearance from the Institutional Ethics Committee (Human), IEC number AMC/EC/PG/5465, dated 21/2/2023.This was a hospital based prospective study, conducted at the Pediatric Intensive Care Unit (PICU) in Assam Medical College and Hospital, Dibrugarh, India. This is a tertiary care referral government hospital. The study was conducted from 1st July 2023 to 31st December 2023. All patients from the age group of one month to twelve years, admitted in the PICU were included. Patients with underlying congenital deformities who required surgical correction, patients who were hospitalized for routine treatment before planned procedures such as intravenous immunoglobulin (IVIG), hemodialysis, Children who died within 24 hours of admission and those where parents refused consent, were excluded.
Considering that p-SOFA has the highest sensitivity of 80.9% in predicting mortality in critically ill children admitted in PICU and the predicted mortality rate by pSOFA score is 28.1% 13; sample size for the present study is calculated and rounded off to be 40 children with 95% confidence and margin of error of 20%.
Initially created for adult patients in the Intensive Care Unit (ICU), the Sequential Organ Failure Assessment (SOFA) score was modified to create the p-SOFA score (Table 1). A thorough assessment of the dysfunction of several organ systems is made possible by the modification of the SOFA score for pediatric patients. Through the evaluation of particular physiological markers, such as hepatic, cardiovascular, pulmonary, coagulation, renal, and neurological functioning, the p-SOFA offers a measurable way to gauge the severity of organ failure in critically ill children. As a result, it is now acknowledged as a valuable tool for estimating mortality in PICU settings.
|
pSOFA SCORE |
0 |
1 |
2 |
3 |
4 |
|
Respiration |
|
|
|
|
|
|
PaO2-FiO2 Or |
≥400 |
300-399 |
200-299 |
100-199 with respiratory support |
<100 with respiratory support |
|
SpO2-FiO2 |
≥292 |
64-291 |
21-264 |
148-220 with respiratory support |
<148 with respiratory support |
|
Coagulation |
|
|
|
|
|
|
Platelets, ×103/ microL |
≥150 |
100-149 |
50-99 |
20-49 |
<20 |
|
Liver |
|
|
|
|
|
|
Bilirubin, mg/dl |
<1.2 |
1.2-1.9 |
2-5.9 |
6-11.9 |
>12 |
|
Cardiovascular |
|
|
|
|
|
|
(MAP by age or vasoactive infusion mm Hg) |
|
|
Dopamine Hydrochloride ≤5 or Dobutamine hydrochloride (any) |
Dopamine hydrochloride or Epinephrine ≤0.1 or Norepinephrine ≤0.1 |
Dopamine hydrochloride >15 or Epinephrine >0.1 or Norepinephrine > 0.1 |
|
<1month |
≥46 |
<46 |
|||
|
1-11 month |
≥55 |
<55 |
|||
|
12-23 month |
≥60 |
<60 |
|||
|
24-59 month |
≥62 |
<62 |
|||
|
60-143 month |
≥65 |
<65 |
|||
|
144-216 month |
≥67 |
<67 |
|||
|
>216 month |
≥70 |
<70 |
|||
|
Neurologic |
|
|
|
|
|
|
Glasgow coma score |
15 |
13-14 |
10-Dec |
06-Sep |
<6 |
|
Renal |
|
|
|
|
|
|
Creatinine by age group (mg/dl) |
|
|
|
|
|
|
<1 month |
<0.8 |
0.8-0.9 |
1.0-1.1 |
1.2-1.5 |
≥1.6 |
|
1-11 month |
<0.3 |
0.3-0.4 |
0.5-0.7 |
0.8-1.1 |
≥1.2 |
|
12-23 month |
<0.4 |
0.4-0.5 |
0.6-1 |
1.1-1.4 |
≥1.5 |
|
24-59 month |
<0.6 |
0.6-0.8 |
0.9-1.5 |
1.6-2.2 |
≥2.3 |
|
60-143 month |
<0.7 |
0.7-1 |
1.1-1.7 |
1.8-2.5 |
≥2.6 |
|
144-216 month |
<1.0 |
1-1.6 |
1.7-2.8 |
2.9-4.1 |
≥4.2 |
|
>216 month |
<1.2 |
1.2-1.9 |
2.0-3.4 |
3.5-4.9 |
≥5 |
(Abbreviations: FiO2- fraction of inspired oxygen; MAP-mean arterial pressure; pSOFA-pediatric Sequential Organ Failure Assessment; SpO2- peripheral oxygen saturation)
An informed and written consent was taken from Parents/Guardians of the participants. After selecting the study participants, the predesigned proforma was filled up with the help of parents or the patient information sheet.
From each patient a 3 ml of venous sample was collected by attending Paediatric resident trained in collecting the samples using 5 ml syringe and 24 G needle. 1 ml was taken in an Ethylene Diamine Tetra-acetic Acid (EDTA) container and properly shaken to prevent from clotting and sent for platelet. 2 ml of venous blood collected in serum separator tubes (BD vacutainer) were used for measurement of serum creatinine, serum bilirubin.
Platelet was estimated with an automated hemo-analyser (Sysmex XN-550 six-part Cell Counter) in the Haematology section of the Pathology department. Serum creatinine and serum bilirubin were estimated at Advanced Clinical Biochemistry Laboratory, Department of Biochemistry using Victros5600 auto-analyser.
After collecting data, it was entered in excel sheets (windows 10). Statistical analysis was done using SPSS 23. Categorical variables were expressed as numbers (percentages), while continuous data were expressed as Mean ± Standard deviation. The Test of Association for Categorical Variables was conducted using the Chi Square Test. The Test of Association for Continuous Variables was conducted using the Anova test or the Student t test. For both scores, the following metrics were computed: specificity, sensitivity, negative predictive value, positive predictive value, and diagnostic accuracy. A P value of less than 0.005 was regarded as statistically significant.
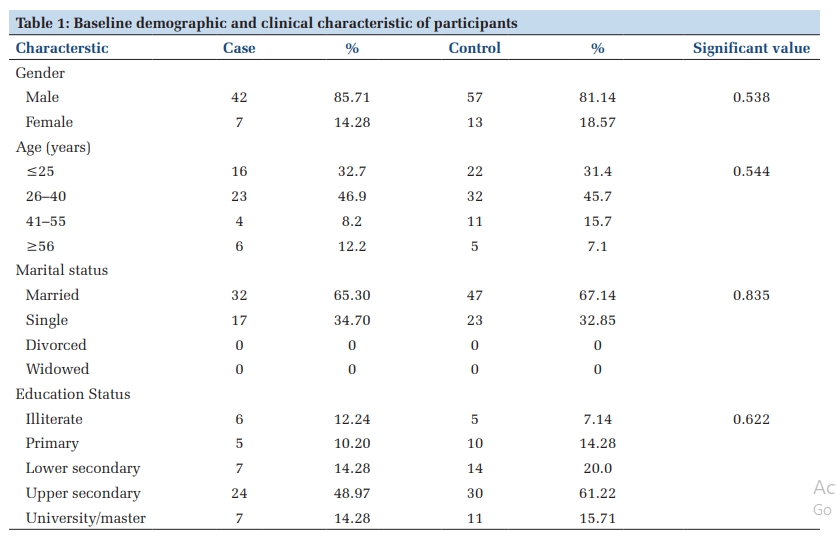
In our study, the most common age group was less than one year of age [Survivors -22(67%), Non-survivors-6(86%)]. The mean age of the study participants was 20.30±30.44 months in the Survivors group and 15.86±24.95 in Non survivors’ group. Male preponderance was observed in our study [Survivors-21(64%), Non-survivors-5(71%)]. The male female ratio was found to be 1.75:1 in Survivors and 2.5:1 in Non-Survivors. Children from the Lower Middle class were predominant in our study [Survivors-28(85%), Non-Survivors-6(86%)].
|
Baseline variables |
Survivors |
Non-Survivors |
p-value |
|
N (33) |
N (7) |
||
|
Age Group (months) |
|
|
0.7204 |
|
0–12 |
22(67%) |
6(86%) |
|
|
>12–24 |
1(3%) |
0(0%) |
|
|
>24–36 |
4(12.1%) |
0(0%) |
|
|
>36–48 |
2(6%) |
0(0%) |
|
|
>48–60 |
2(6%) |
0(0%) |
|
|
>60 |
2(6%) |
1(14%) |
|
|
Mean±SD |
20.30±30.44 |
15.86±24.95 |
|
|
Gender |
|
|
|
|
Male |
21(64%) |
5(71%) |
0.6985 |
|
Female |
12(36%) |
2(29%) |
|
|
Socioeconomic class |
|
|
|
|
Upper |
0(0%) |
0(0%) |
|
|
Upper Middle |
2(6%) |
0(0%) |
|
|
Lower Middle |
28(85%) |
6(86%) |
0.7483 |
|
Upper Lower |
3(9%) |
1(14%) |
|
|
Lower |
0(0%) |
0(0%) |
|
|
Presenting Complaints |
Survivors |
Non-Survivors |
p-value |
|
N (33) |
N (7) |
||
|
Presenting complaints |
|
|
|
|
Cough |
25(76%) |
4(57%) |
0.5902 |
|
Fever |
22(66%) |
4(57%) |
0.6315 |
|
Breathing Difficulty |
24(73%) |
4(57%) |
0.4131 |
|
Abnormal Jerky Movements |
6(18%) |
6(86%) |
0.0004 |
|
Others |
10(30%) |
3(43%) |
0.522 |
|
Pulse Volume (n/%) |
32(97%) |
2(29%) |
<0.0001 |
|
Good |
1(3%) |
5(71%) |
|
|
Feeble |
|
|
|
|
Subcostal Retractions |
|
|
|
|
Positive |
30(91%) |
4(57%) |
|
|
Negative |
3(9%) |
3(43%) |
|
|
Pulse Rate/min (Mean±SD) |
137.91 ± 18.38 |
155.57 ± 19.93 |
0.0284 |
|
Respiratory Rate/min (Mean±SD) |
58.76 ± 14.83 |
41.00 ± 17.51 |
0.0081 |
SD- standard deviation, %- percentage.
Cough was the most common presentation in our study [Survivors-25(76%), Non-Survivors-4(57%)] followed by breathing difficulty [Survivors-24(73%), Non-Survivor -4(57%)]. Pulse volume was good in the Survivors [32(97%)] and feeble in Non-Survivors [5(71%)]. Subcostal retraction was positive in both groups [(Survivors- 30(91%), Non-Survivors-4(57%)]. The respiratory rate was found to be more in Survivors and less in Non-survivors and the difference was found to be statistically significant (Table 3).
In survivors, the most common provisional diagnosis was severe pneumonia [24(73%)] followed by meningitis, acute encephalitis syndrome and failure to thrive [2(6%)]. Among the Non- survivors, the commonest provisional diagnosis was Severe pneumonia [3(43%)] followed by meningitis and Acute encephalitis syndrome [2(29%)]. Severe pneumonia [23(73%)] was the most common diagnosis followed by Acute encephalitis syndrome, meningitis, and failure to thrive [2(6%)]. Among the Non-survivors, Meningitis was the most common diagnosis [3(43%)] followed by Septicemia [2(29%)].

33(82.50%) of the study participants were discharged and 7(17.5%) of the study participants died. The mean score was found to be more in those study participants who died, compared to the survivors. There was a difference between the two groups, and it was found to be statistically significant.
|
Provisional Diagnosis |
Survivors |
Non-Survivors |
|
N (33) |
N (7) |
|
|
Severe pneumonia |
24(73%) |
3(43%) |
|
Meningitis |
2(6%) |
2(29%) |
|
Acute encephalitis syndrome |
2(6%) |
2(29%) |
|
Congenital heart disease |
1(3%) |
0(0%) |
|
Failure to Thrive (inadequate calorie intake) |
2(6%) |
0(0%) |
|
Glomerular nephritis |
1(3%) |
0(0%) |
|
Diabetic ketoacidosis |
1(3%) |
0(0%) |
|
Diagnosis |
Survivors |
Non-Survivors |
|
N (33) |
N (7) |
|
|
Severe pneumonia |
23(73%) |
1(14%) |
|
Meningitis |
2(6%) |
3(43%) |
|
Acute encephalitis syn- drome |
2(6%) |
1(14%) |
|
Septicemia |
1(0%) |
2(29%) |
|
Failure to Thrive (inadequate calorie intake) |
2(6%) |
0(%) |
|
diabetic ketoacidosis |
1(3%) |
0(0%) |
|
Congenital heart disease |
1(3%) |
0(0%) |
|
Acute Glomerular Nephritis with anemia with left empyema thoracis |
1(3%) |
0(0%) |
|
Ooutcome of the patient |
Score |
p-value |
|
Discharged |
3.79±2.64 |
<0.0001 |
|
Death |
10.86±1.35 |
The most common presentation in the PICU is the sepsis which is the major cause of mortality and morbidity among the children. It is important for the clinician to predict the patient’s risk accurately within days following the admission 13. To determine a patient’s prognosis and to improve the decision-making process for the patient’s good outcome, scoring systems are used by the health care managers. The scoring system is also useful to predict the outcome and helps inprompt intervention. But developing an optimal scoring system is a challenging task. The pSOFA score helps in discriminating excellently for the PICU population for the in- hospital mortality. The overall mortality rate of our study was 17.5%. This was similar to the results of Lalitha AV et al study where the overall mortality rate was 17.5%. This was lesser than the mortality rate in other developing countries which reported at about 20% in many studies. In our study the most common age group was less than one year of age. The mean age of the study participants was 20.30±30.44 months in Survivors group and 15.86±24.95 in Non survivors group. Male preponderances were observed in our study [Survivors (64%), Non-Survivors (71%)]. Similar results were also seen in the Lalitha Av et al study where male preponderance was observed as 56.8 % in Survivors and 64.3% among Non-Survivors. The male female ratio was found to be 1.75:1 in Survivors and 2.5:1 in Non-Survivors. In El Mashad et al study, the male female ratio of the survivors was found to be 0.9:1 where female preponderance was observed. In non-survivors the ratio was 1.54:1 where male preponderance was seen 13 . Children from the Lower Middle class were predominant in our study [Survivor-28(85%), Non-Survivors - 6(86%)]. The mean score was found to be more in participants who died (10.86±1.35) compared to those discharged (3.79±2.64). There was a difference between the group and it was found to be statistically significant. Similar results were also seen by Priya Gogia et al, where the mean pSOFA score was found to be more in non-survivors compared to survivors which was statistically significant. Study done by Priya Gogia et al, stated that the pSOFA score done at 72 hours was highly statistically significant. In study done by Ferreira et al, the mean score was taken at initial, after 48 hours and delta sofa score was found to be high in non-survivors compared to survivors and was statistically significant. Early serial evaluation of the score during the first three days of the PICU admission is considered as better indicator for the prognosis than the initial assessment done at admission. Craig DG et al observed that the median SOFA score was found to be higher in patients who died. Thus, pSOFA score can be used as a prognostic indicator in ill children as it is easily available and can be measured routinely compared to other scores.
The sample size was small (n=40). We did not take pSOFA score at different points so we could not portray which point or interval is better. The pSOFA score was not compared with other scores to measure the accuracy.
The pSOFA score at the time of admission is useful for predicting the mortality and outcome the patients in the PICU population. Since the parameters of pSOFA score are less, it offers the advantage of being a relatively simple, cost effective and easy to calculate scoring system. This score focuses on organ dysfunction and provides a comprehensive assessment of the patient’s condition and may facilitate early intervention to prevent further deterioration.
None
None
Subscribe now for latest articles and news.