Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.422
Year: 2026, Volume: 12, Issue: 2, Pages: 150-154
Original Article
Divya Bajpai 1, Himanshu Pandey 2, Nitesh Mohan 3
1Associate Professor, Department of Pathology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh, India.
2Associate Professor, Department of Radiology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh, India.
3Professor and Head, Department of Pathology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh, India.
Address for correspondence: Divya Bajpai, Associate Professor, Department of Pathology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh, India.
E-mail: [email protected]
Received Date:29 December 2025, Accepted Date:07 April 2026, Published Date:18 May 2026
Introduction: Breast cancer is one of the most frequently diagnosed malignancies in women. Tumour-infiltrating lymphocytes are emerging as important biomarkers in breast cancer for assessing the prognosis of cases particularly in triple-negative and HER2-positive subtypes. This study aimed to quantify Tumour-infiltrating lymphocytes in breast carcinoma and evaluate their correlation with other established prognostic parameters.
Material and Methods: An observational study was conducted on 40 histologically confirmed breast carcinoma cases. Tumour-infiltrating lymphocytes were scored on H&E-stained sections following International Tumour-infiltrating lymphocytes Working Group 2014 guidelines. Correlation between Tumour-infiltrating lymphocytes and clinicopathological parameters were evaluated using chi-square tests.
Results: Statistically significant association of Tumor Infiltrating Lymphocytes was seen with tumor grade (p = 0.043) and Ki-67 proliferation index (p = 0.037). Age, tumor size, lymph node status or molecular subtype did not yield significant association.
Conclusion: Tumour-infiltrating lymphocytes demonstrated significant correlations with tumor grade and Ki-67 proliferation index values. The findings support integrating Tumour-infiltrating lymphocytes scoring into routine breast cancer reporting for improved prognostic evaluation.
Breast cancer is one of the most frequently diagnosed malignancies in women accounting for 24% of all female cancers and leading cause of female cancer related mortality worldwide[1]. Incidence of cancer breast is increasing in recent decade in low and middle income countries[2] Better screening methods attributed to increasing incidence and the triple assessment for breast malignancy including clinical examination, Imaging and Needle Biopsy. However, it is still amongst the major causes of death.
Invasive Breast Carcinoma refers to large and hetero- genous group of malignant neoplasms of glandular
elements of the breast[1]. Breast cancer is traditionally classified according to the expression of hormonal receptors (HR) and human epidermal growth factor receptor 2 (HER2) in three subtypes: HR-positive/ HER2 negative BC, HER2+ BC and HR-/HER2- (i.e. triple negative) breast cancer which form 70%, 15-20% and 10-15% breast cancers respectively.
Moreover, patients having the same stage at diagnosis may have different clinical outcome stressing on the hypothesis that there is a complex and dynamic interaction between tumour cells and the immune cells of the body[3, 4].
Tumour Infiltrating Lymphocytes are lymphoid cells infiltrating the tumour and its stroma and they represent the host immune response against the tumour cells. It may represent a prognostic marker[5-7].
In the present study various prognostic markers of carcinoma breast are assessed, the relation of these prognostic markers with tumour infiltrating lymphocytes is studied thus attempting to standardize the characterization of breast malignancy by subtype and
immune environment.
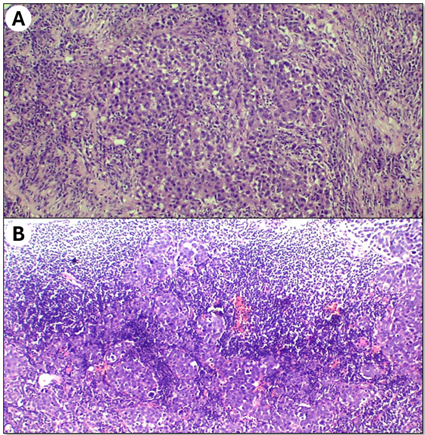
Scoring of Tumour-infiltrating lymphocytes is done as per the standardized methodology developed by the International Tumour-infiltrating lymphocytes working group 2014[8, 9] on formalin fixed paraffin embedded breast tumour tissue obtained by core needle biopsy or excision. Tumour-infiltrating lymphocytes are scored on HE sections in the stromal compartment within the tumour border. Tumour-infiltrating lymphocytes are quantified as a ratio between the stromal area occupied by the lymphocytes and plasma cells and total intratumoral stromal area and assessed as a percentage. Tumour-infiltrating lymphocytes present in the areas of artifacts, necrosis or hyalinization are excluded.
The term lymphocyte predominant breast cancer is used to describe breast cancer with more than 50% of stromal lymphocytes.
Molecular classification was done by standard immunohistochemistry measurements by ER, PR, ERBB2 and Ki-67 proliferation index.
The present study aims to quantify the Tumour Infiltrating Lymphocytes in cases of carcinoma breast and to correlate the scoring with other prognostic markers, thus attempting to use Tumour-infiltrating lymphocytes as a prognostic marker and a guide to therapy.
The observational study was conducted in the Department of Pathology, at our hospital for a duration of 4 months from May to August 2024 after taking approval from the Institutional ethics committee.
All newly diagnosed cases as carcinoma breast on Histopathology in the department of Pathology during study period were studied. Due diligence was done to prevent any repetition of cases during the study period. Clinical details were taken from the case sheet, and a proforma was filled which included CR number, name, age, Histopathology number, IHC number, tumor size, modified Nottingham score, grade, LVI, PNI, lymph node status, molecular classification. ER, PR, HER2Neu. Radiological help was taken where necessary. IHC for ER, PR, HER2Neu and Ki-67 proliferation index was done as per the standard protocol. Tumour-infiltrating lymphocytes score was evaluated as per the International Tumour-infiltrating lymphocytes Working Group 2014 which suggests only Tumour-infiltrating lymphocytes within the borders of the invasive tumors in the stroma are evaluated. Immune infiltrates outside the tumour border, in adjacent normal tissue is not included. Large areas of necrosis or fibrosis is not included. The tumour is scanned at low magnification. Only the mononuclear infiltrate, lymphocytes and plasma cells are included. Granulocytic infiltrate in the area of tumour necrosis is not included. Tumour is then included in three groups: Group A – tumour with no/ minimal immune cells (0-10% stromal tumour-infiltrating lymphocytes); Group B – tumour with intermediate/ heterogenous infiltrate (10-40% stromal tumour-infiltrating lymphocytes) and group C – tumour with high immune infiltrate (40-90% stromal tumour-infiltrating lymphocytes). For the intermediate group different areas are evaluated at high magnification. The calculated Tumour-infiltrating lymphocytes score was correlated with other prognostic markers.
Inclusion criteria: The study included all newly diagnosed cases of carcinoma breast received in the Department of Pathology during the study period.
Exclusion criteria: Cases where IHC could not be done, cases which received any other therapy prior to biopsy. Lumpectomy/MRM of a case where biopsy was already included in the study.
Statistical analysis was performed to evaluate the association between tumor-infiltrating lymphocytes (TILs) and various clinicopathological parameters in breast carcinoma. All data were entered into Microsoft Excel and analyzed using SPSS Statistics software (version 26.0).
Categorical variables such as age group, tumor grade, molecular subtype, Ki-67 proliferation index, nodal status, and tumor size were expressed as frequencies and percentages. The association between TIL levels and these clinicopathological parameters was assessed using the Chi-square test.
To evaluate whether TIL levels could predict clinicopathological characteristics, binary logistic regression analysis was performed. Regression coefficients (β), standard errors, Z values, and odds ratios with 95% confidence intervals were calculated. A p value <0.05 was considered statistically significant.
A total of 40 histologically confirmed breast carcinoma cases were included in the study. The age of the patients ranged from 21 to 85 years, with the majority of the cases (67.5%) belonging to the ≤50-year age group, while 32.5% were older than 50 years. The association observed between the age category and tumour-infiltrating lymphocyte levels (p = 0.389) did not reach statistical significance. Left-sided breast involvement was more common (67.5%) compared to right-sided lesions. The specimens comprised core biopsies (55%), modified radical mastectomies (40%), and lumpectomies (5%).
Hormone receptor testing showed estrogen receptor (ER) positivity in 47.5% of cases, progesterone receptor (PR) positivity in 35%, and HER2 positivity in 30%, with 12.5% being HER2-equivocal. Tumour grading revealed that most tumours were Grade II (77.5%), followed by Grade III (17.5%) and Grade I (5%). A statistically significant association was observed between tumour grade and tumour-infiltrating lymphocytes category (p = 0.043), with higher-grade tumors demonstrating increased tumour-infiltrating lymphocytes infiltration. In Multivariate regression analysis tumor grade demonstrated a significant regression coefficient (β = 2.23, SE = 0.94, Z = 2.37, p = 0.018), indicating a significant association between higher TIL levels and higher tumor grade.
Tumour-infiltrating lymphocytes percentages ranged from 0% to 90% and were categorized into three groups: low (0–10%) in 25% of cases, intermediate (11–40%) in 45%, and high (>40%) in 30% of cases.
Intermediate Tumour-infiltrating lymphocytes infiltra- tion was the most frequently observed category. Molecular classification identified 7.5% cases as Luminal A, 20% as Luminal B HER2-negative, 10% as Luminal B HER2-positive, 20% as HER2-enriched, and 30% as triple-negative breast cancer (TNBC); 12.5% required additional HER2 FISH testing. Although TNBC and HER2-enriched tumors exhibited higher proportions of high tumour-infiltrating lymphocytes infiltration, the association between molecular subtype and tumour-infiltrating lymphocytes was not statistically significant (p = 0.517).
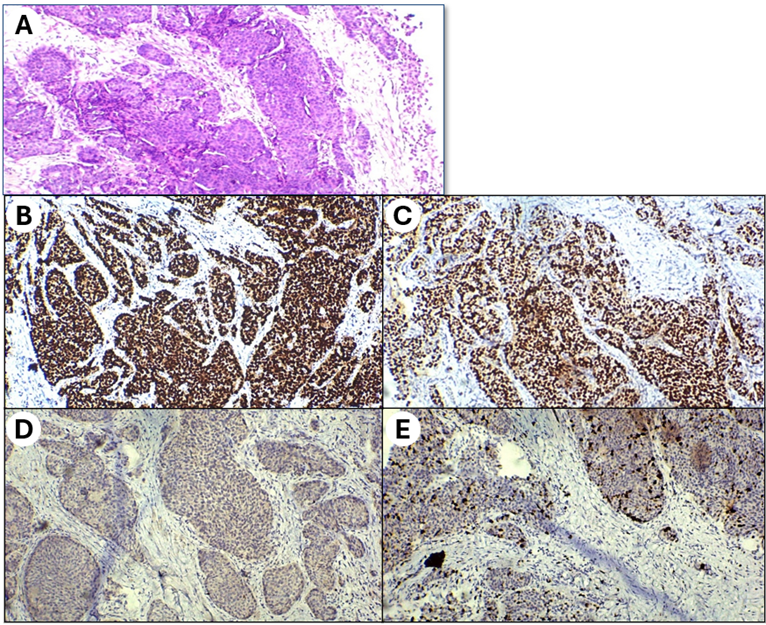
Ki-67 proliferation index ranged from 1% to 90%, with 70% of tumors showing Ki-67 proliferation index ≥30%. A statistically significant association was observed between Ki-67 proliferation index and Tumour-infiltrating lymphocytes levels (p = 0.037), with high-proliferation tumors demonstrating greater Tumour-infiltrating lymphocytes infiltration. Lymph node metastasis was present in 55% of cases. High Tumour-infiltrating lymphocytes infiltration was more commonly seen in node-negative cases, but the association did not reach statistical significance (p = 0.091). Tumor size ranged from 1.2 cm to 8.2 cm; however, tumor size did not significantly correlate with Tumour-infiltrating lymphocytes category (p = 0.462). Apart from these other prognostic parameters used were Margin status, LVI and PNI. Margins were negative in all the cases of lumpectomy and MRM. LVI was seen in 4 cases whereas PNI was seen in 2 cases. Overall, Tumour-infiltrating lymphocytes showed statistically significant associations with tumor grade and proliferation index (Note: refer supplementary file for tables).
This study evaluated Tumour-infiltrating lymphocytes in breast carcinoma and assessed their correlation with the already established prognostic indicators. Tumour-infiltrating lymphocytes assessment followed the standardized recommendations by Salgado et al.[8], ensuring consistency with international practice.
In this study younger patients (age≤50 years) exhibited higher proportions of intermediate and high tumour-infiltrating lymphocytes levels, however statistically significant association was not observed as shown by Takada et al.[2], who emphasized that chronological age alone does not reliably predict tumour-infiltrating lymphocytes density due to the heterogeneity of host immune responses.
A significant association was observed between tumor grade and tumour-infiltrating lymphocytes density, with high-grade tumors demonstrating increased immune infiltration. This finding is biologically plausible, as poorly differentiated tumors possess heightened genomic instability and neoantigen production, attracting more lymphocytes. This pattern is consistent with Denkert et al.[10] and Sotiriou[11], who described increased immunogenicity in high-grade tumors. The significant association in our study reinforces the relevance of tumour-infiltrating lymphocytes as markers of tumor biology which can be included as an independent tumour marker in near future.
Higher tumour-infiltrating lymphocytes infiltration was seen in TNBC and HER2-enriched subtypes of carcinoma breast but the association was not statistically significant as shown by Gao et al.[1] and Stanton et al.[3], who demonstrated that TNBC and HER2-positive tumors are more immunogenic and exhibit stronger lymphocytic infiltration. Similarly, Valenza et al.[4] highlighted that tumour-infiltrating lymphocytes serve as meaningful biomarkers across breast cancer subtypes, especially in aggressive phenotypes. Furthermore, Loi et al.[12] confirmed that high tumour-infiltrating lymphocytes predict improved prognosis and better chemotherapy response in early-stage TNBC.
A statistically significant association was found between high Ki-67 proliferation index and elevated tumour-infiltrating lymphocytes infiltration. Highly proliferative tumors generate greater numbers of neoantigens, stimulating increased immune recognition. This is supported by Savas et al.[13], who demonstrated that proliferation and immune activation are interconnected predictors of treatment response.
Lymph node negative tumours demonstrated relatively higher tumour-infiltrating lymphocytes although not statistically significant in this study, may signify robust immune infiltration reduces metastatic potential and improves outcomes as shown by Luen et al.[14] and Park et al.[15]
Statistically significant correlation was not found between tumor size and tumour-infiltrating lymphocytes, indicating that immune infiltration is influenced more by tumor biology than tumor volume. This observation is consistent with the analyses of Schmidt et al.[16], who described tumour-infiltrating lymphocytes density as an independent biological parameter.
High tumour-infiltrating lymphocytes infiltration correlates with better response to chemotherapy and improved survival, particularly in TNBC and HER2-positive subtypes, as also demonstrated by Zhang et al.[17] and Cao et al.[18].
Tumour Infiltrating Lymphocytes have strong prognostic value in improving estimates of distant recurrence free survival, disease free survival and overall survival in early-stage TNBCs treated with standard adjuvant and neo adjuvant chemotherapy. Findings are based on tumour Infiltrating Lymphocytes levels at the time of diagnosis (before any treatment). Clinical utility in treatment allocation is still under research. Therefore, tumour Infiltrating Lymphocytes should be considered as a stratification factor in clinical trials and should be included in studies evaluating prognosis. Thus, incorporating the Tumour Infiltrating Lymphocytes in routine practice will increase the availability of data on tumour Infiltrating Lymphocytes.
The present study has limitations as the sample size was relatively small and it was a single institution study. Molecular subtyping was based on immunohistochemical surrogates rather than gene expression profiling. Tumour infiltrating levels were done manually on H&E sections. The absence of longitudinal follow-up data is one additional limitation. Hence larger multi-institution studies with digital quantification of various parameters and long term follow up may substantially improve the validity of the results in the Indian population[19].
Tumour-infiltrating lymphocytes density shows statistically significant associations with tumor grade and proliferation index. These findings highlight the role of tumour-infiltrating lymphocytes as valuable prognostic indicators in breast cancer. Incorporating tumour-infiltrating lymphocytes assessment into routine pathology practice can support better prognostic stratification and may guide therapeutic selection, particularly in immune-responsive breast cancer subtypes.
Conflict of interest: None.
Funding: None.
1. Predictive and prognostic role of tumour-infiltrating lymphocytes in breast cancer patients with different molecular subtypes: a meta-analysis. BMC Cancer. 2020; 20 (1). Available from: https://doi.org/10.1186/s12885-020-07654-y
2. Differences in tumor-infiltrating lymphocyte density and prognostic factors for breast cancer by patient age. World Journal of Surgical Oncology. 2022; 20 (1). Available from: https://doi.org/10.1186/s12957-022-02513-5
3. Clinical significance of tumor-infiltrating lymphocytes in breast cancer. Journal for Immuno Therapy of Cancer. 2016; 4 (1). Available from: https://doi.org/10.1186/s40425-016-0165-6
4. Tumor Infiltrating Lymphocytes across Breast Cancer Subtypes: Current Issues for Biomarker Assessment. Cancers. 2023; 15 (3). Available from: https://doi.org/10.3390/cancers15030767
5. Evaluation of Tumor infiltrating lymphocytes in breast carcinoma and their correlation with molecular subtypes, tumor grade and stage. Breast Disease. 2020; 39 (2). Available from: https://doi.org/10.3233/bd-200442
6. Heterogeneity of tumour‐infiltrating lymphocytes in breast cancer and its prognostic significance. Histopathology. 2018; 73 (6). Available from: https://doi.org/10.1111/his.13695
7. Tumor infiltrating lymphocytes in early breast cancer. The Breast. 2018; 37 Available from: https://doi.org/10.1016/j.breast.2017.03.010
8. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Annals of Oncology. 2015; 26 (2). Available from: https://doi.org/10.1093/annonc/mdu450
9. Update on tumor-infiltrating lymphocytes (TILs) in breast cancer, including recommendations to assess TILs in residual disease after neoadjuvant therapy and in carcinoma in situ. Seminars in Cancer Biology. 2018; 52 (Pt 2). Available from: https://doi.org/10.1016/j.semcancer.2017.10.003
10. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. The Lancet Oncology. 2018; 19 (1). Available from: https://doi.org/10.1016/s1470-2045(17)30904-x
11. Gene-Expression Signatures in Breast Cancer. New England Journal of Medicine. 2009; 360 (8). Available from: https://doi.org/10.1056/nejmra0801289
12. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. Journal of Clinical Oncology. 2019; 37 (7). Available from: https://doi.org/10.1200/jco.18.01010
13. Clinical relevance of host immunity in breast cancer: from TILs to the clinic. Nature Reviews Clinical Oncology. 2016; 13 (4). Available from: https://doi.org/10.1038/nrclinonc.2015.215
14. Tumour-infiltrating lymphocytes and the emerging role of immunotherapy in breast cancer. Pathology. 2017; 49 (2). Available from: https://doi.org/10.1016/j.pathol.2016.10.010
15. Prognostic value of tumor-infiltrating lymphocytes in patients with early-stage triple-negative breast cancers (TNBC) who did not receive adjuvant chemotherapy. Annals of Oncology. 2019; 30 (12). Available from: https://doi.org/10.1093/annonc/mdz395
16. Schmidt M, Hellwig B, Hammad S. A comprehensive analysis of tumor-infiltrating lymphocytes in breast cancer using data from 12,439 patients. Breast Cancer Research and Treatment. 2018; 171:563–575.
17. Prognostic and predictive value of tumor-infiltrating lymphocytes in breast cancer: a systematic review and meta-analysis. Clinical and Translational Oncology. 2016; 18 (5). Available from: https://doi.org/10.1007/s12094-015-1391-y
18. Prognostic relevance of tumor‑infiltrating lymphocytes in residual tumor tissue from patients with triple‑negative breast cancer following neoadjuvant chemotherapy: A systematic review and meta‑analysis. Oncology Letters. 2023; 26 (4). Available from: https://doi.org/10.3892/ol.2023.14028
19. WHO classification of tumours: breast tumours. 5th ed. Lyon: International Agency for Research on Cancer. 2019; Available from: https://doi.org/10.53347/rid-70716
Subscribe now for latest articles and news.