Introduction
Androgenetic alopecia (AGA), is characterized by gradual thinning and loss of scalp hair. 1 30% of men experience AGA by age of 30, and 50% by age of 50. 2 A study conducted in India reported 58% prevalence of AGA. 3
Genetic predisposition to AGA has intrinsic link with testosterone and 5α dihydrotestosterone (DHT) – produced by action of enzyme 5α-reductase. 4, 5, 6
Emerging evidence suggests that early onset AGA may be associated with cardiovascular risk. Androgens have been recognized for their role in the development of cardiovascular disease (CVD). 7 Hair loss may serve as an indicator of androgenic activity, potentially influencing coronary atherosclerosis. Multiple studies have explored the connection between male pattern baldness and cardiovascular risk factors. Recent research suggests that male baldness could be a marker for the presence of cardiovascular risk factors. 8 The likelihood of coronary heart disease and cardiovascular events increases with certain patterns of hair loss, 9 increasing rate of hair loss, 10 and the extent of baldness in both younger 8 and older men. 11 Severe baldness in older men has also been linked to a higher risk of cardiovascular mortality. 11 Nevertheless, existing literature fails to discern such a direct association. 12 Hence this study was undertaken to ascertain prevalence of MetS and cardiovascular risk factors in early onset male AGA. The objectives of this study are to assess the prevalence of metabolic syndrome (MetS) and cardiovascular risk factors in individuals with early onset male androgenetic alopecia (AGA). Additionally, the study aims to explore the relationship between the severity of AGA and the presence of MetS and cardiovascular risk factors, while also considering the demographic profile of the participants. By examining these associations, the research seeks to provide insights into how early onset AGA might correlate with broader health risks, specifically in terms of metabolic and cardiovascular conditions, and how these relationships may vary across different demographic groups.
Materials and Methods
The cross-sectional study was conducted in the dermatology department from March 2021 to March 2022, with ethical clearance obtained from the Institutional Ethics Committee. Male patients aged 18 to 35 years, diagnosed with androgenetic alopecia (AGA) and visiting the dermatology department during the study period, were included. Patients on immunosuppressive treatment for the past month, undergoing treatment for AGA, or using lipid-lowering or hypoglycemic medications were excluded from the study. A total of 99 participants who met the eligibility criteria and gave informed consent were recruited. A detailed medical history was obtained, followed by a comprehensive systemic and cutaneous examination. AGA was diagnosed based on clinical findings, and its severity, along with the status of metabolic syndrome and carotid intima-media thickness (CIMT), was assessed. Clinical photographs were taken with the patients' informed consent. Permission was also obtained to use their photographs, with assurance of concealing their identities. AGA was classified using the Hamilton Norwood scale, with types I-III representing normal to mild AGA and types IV-VII representing moderate to severe AGA. 13 Metabolic syndrome was defined according to the National Cholesterol Education Program Adult Treatment Panel III criteria, requiring the presence of three or more of the following: triglyceride levels ≥150 mg/dl, high-density lipoprotein (HDL) <40 mg/dl, fasting blood sugar ≥100 mg/dl, waist circumference >102 cm, or blood pressure ≥130/85 mmHg. Waist circumference was measured 2 cm above the navel using a flexible tape, with the patient standing. Laboratory investigations included lipid profile (LDL, HDL, total cholesterol, triglycerides), fasting blood sugar, and B-mode ultrasound of the common carotid artery to assess CIMT and detect atheromatous plaques. CIMT was measured 1.5 cm below the bifurcation of the common carotid artery on both the left and right sides, and an average of the two values was used as the final CIMT measurement. The ultrasound image displayed the anterior and posterior walls of the carotid artery as two bright white lines, with the distance between the leading edges of the far wall (lumen-intima interface) and the second bright line (media-adventitia interface) representing the CIMT.
Study Design: An observational clinical single group study.
Statistical Methods: Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5 % level of significance. The following assumptions on data is made.
Assumptions:
-
Dependent variables should be normally distributed.
-
Samples drawn from the population should be random, cases of the samples should be independent.
Student t test (two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters. Leven`s test for homogeneity of variance has been performed to assess the homogeneity of variance. A t-test is a statistical test that is used to compare the means of two groups. It is often used in hypothesis testing to determine whether a process or treatment actually has an effect on the population of interest, or whether two groups are different from one another with the null hypothesis (H0) is that the true difference between these group means is zero and the alternate hypothesis (Ha) is that the true difference is different from zero.
Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups, Non-parametric setting for Qualitative data analysis. Fisher Exact test used when cell samples are very small.
Significant figures:
+ Suggestive significance (P value: 0.05<P<0.10)
* Moderately significant (P value:0.01
** Strongly significant (P value: P ≤0.01)
Statistical software: The Statistical software namely SPSS 22.0, and R environment
ver.3.2.2 were used for the analysis of the data and Microsoft word and Excel have
been used to generate graphs, tables etc.
Sample size: 99 cases of androgenetic alopecia meeting the inclusion criteria attending to the BGS GIMS department of dermatology out- patients during the study period between March 2021 to March 2022.
In an observational correlational study with Incidence of Metabolic Syndrome derived in patients with androgenetic alopecia in relation to control (10.0% in cases vs 2.0% in controls) derived from previous literature, 90% statistical power, 5% level of significance, the sample size of 99 is adequate for a single group observational clinical study.
Results
A total of 99 cases of early-onset androgenetic alopecia (AGA) were enrolled in the study, with the most common age group being 20 to 25 years and a mean age of 24.84 ± 4.85 years. The majority (44.4%) of patients were classified under Grade 2 AGA, and 94.9% were in the Mild AGA category (Norwood-Hamilton AGA I to III), while 5.1% had Severe AGA (Norwood-Hamilton AGA IV to VII). Additionally, 58.6% of patients had a hair loss duration of 3 to 12 months, and 56.6% reported a positive family history of AGA. A smoking history was present in 17.2% of patients. The mean waist circumference was 34.28 ± 3.75 cm, the mean fasting blood sugar (FBS) was 94.62 ± 12.20 mg/dL, and the mean triglycerides (TG) level was 134.25 ± 53.72 mg/dL, with an HDL level of 44.96 ± 8.70 mg/dL. Blood pressure readings showed a mean systolic blood pressure (SBP) of 125.68 ± 9.93 mmHg and a mean diastolic blood pressure (DBP) of 82.49 ± 7.35 mmHg. Only one patient had a carotid intima-media thickness (CIMT) greater than 0.8 mm, and seven patients were diagnosed with metabolic syndrome, all of whom belonged to the Mild AGA group. Among the metabolic syndrome patients, 14.3% had a smoking history. Notably, metabolic syndrome patients had significantly higher mean SBP (135.71 ± 10.48 mmHg) and DBP (90.57 ± 12.90 mmHg) compared to those without metabolic syndrome (SBP: 124.91 ± 9.52 mmHg, DBP: 81.87 ± 6.46 mmHg), with p-values of <0.005 and <0.002, respectively. Furthermore, the mean FBS in metabolic syndrome patients was 114 ± 3.96 mg/dL, significantly higher than that in patients without metabolic syndrome, who had a mean FBS of 93.15 ± 11.33 mg/dL (p < 0.001).






Discussion
The relationship between androgenetic alopecia (AGA) and metabolic syndrome has been a subject of extensive research in previous years. While some studies have established connections between these conditions, the findings have been inconsistent. The purpose of our study was to investigate whether metabolic syndrome is present in individuals with early-onset androgenetic alopecia and to explore the metabolic parameters in relation to the severity of AGA.
Early-onset androgenetic alopecia (AGA) was chosen for our study because individuals with early-onset AGA are often considered to have a more severe 14 or genetically predisposed form of the condition. 15 This early manifestation may have a stronger association with metabolic abnormalities or other systemic conditions, such as metabolic syndrome, compared to those who develop AGA later in life. 16 Investigating this subgroup could provide valuable insights into whether early-onset AGA could serve as an early indicator for other health conditions like metabolic syndrome, allowing for earlier intervention and treatment.
In our study, 99 individuals diagnosed with androgenetic alopecia were assessed and graded according to the Hamilton Norwood classification system. We examined various health conditions including hypertension, hyperlipidemia, fasting blood glucose levels, and carotid intima-media thickness (CIMT). The participants underwent blood tests to measure levels of HDL cholesterol, triglycerides, and fasting blood glucose, along with anthropometric measurements such as height, weight, and waist circumference.
The average age of the participants in our study was 24.84 ± 4.85 years, which is consistent with the study by Qi Ding, where the average age was 26.0 ± 4.6 years.17 Previous studies have suggested that the onset of AGA typically coincides with puberty. 18 Sehgal et al. found that 50% of their study population experienced the onset of AGA between the ages of 20 to 24 years. This aligns with our findings, as most of our patients were between 20 to 25 years of age, with a median age of onset being 24 years. 19 This early onset of AGA may be attributed to factors such as the pressures of a competitive social structure or lifestyle changes, although further investigation is needed.
The duration of hair loss plays a critical role in determining the appropriate treatment for patients. In our study, 78% of patients presented with 1 to 5 years of hair loss. This is in line with the findings of Nargis T et al., where 61.2% of patients reported a hair loss duration of 1 to 4 years. It appears that individuals are more likely to seek medical attention for hair loss in their younger years but tend to accept it as they age. 20
In terms of AGA severity, 44.4% of patients were diagnosed with Grade 2 AGA, while 33.3% had Grade 1 AGA. To further explore potential associations with other risk factors, we categorized the cases into two groups: Mild AGA (Hamilton Norwood types I–III) and moderate to severe AGA (Hamilton Norwood types IV–VII). Our study found that 94.9% of the patients had mild AGA, while only 5.1% had severe AGA. This differs from a study by another researcher, where 77% of patients had mild AGA, and 23% had severe AGA. 21 Furthermore, 63.9% of mild AGA patients reported hair loss duration of 3 months to 1 year, while 60% of severe AGA patients had hair loss for 2 to 5 years. These findings are in accordance with the study by Nargis T et al. 20
Androgenetic alopecia is generally considered a genetically predisposed condition, though the exact mode of inheritance is not fully understood. 22 In our study, 56.6% of patients had a family history of AGA, which is lower than the 64.1% prevalence found in an epidemiological study involving 3114 Korean patients with AGA. 23 Previous studies have shown that AGA can be inherited from either the paternal or maternal side, or both. Notably, some studies suggest that a family history of paternal AGA has a more significant impact on the expression of the condition. 23, 24 However, in our study, patients were asked only about a general family history of baldness, and the distinction between paternal or maternal inheritance was not explored.
In our study, 58.5% of mild AGA patients and 20% of severe AGA patients reported a positive family history of AGA. This indicates that patients with early-onset AGA may benefit from early intervention to prevent further progression of the condition. Additionally, 17.2% of the patients had a history of smoking, though the quantity and duration of smoking were not considered. A 2015 study on early-onset androgenetic alopecia and associated risk factors did not find a significant relationship between smoking status and the onset of AGA. The quantity of cigarettes smoked was also found to be unrelated to the onset of AGA in that study. 20
Waist circumference is a key measure in assessing the risk of metabolic syndrome and obesity. In our study, 9% of patients had a waist circumference greater than 102 cm, with an average waist circumference of 87.07 ± 9.52 cm. This finding is similar to the study conducted by Chakrabarty S, where the mean waist circumference was 84.79 cm. 25 Previous research has demonstrated that waist circumference is one of the most significant risk factors for developing metabolic syndrome, and obesity is an independent risk factor for cardiovascular disease. Our findings emphasize the importance of monitoring waist circumference in patients with AGA to assess their risk for developing metabolic conditions.
Fasting blood sugar (FBS) levels were elevated in 33.3% of patients in our study, with a mean FBS value of 94.62 ± 12.20 mg/dl. This value is lower than the cutoff point of 100 mg/dl, which contrasts with other studies where the mean FBS level was much higher (127.2 ± 67.1 mg/dl). 21 Previous studies have suggested that moderate or severe AGA is associated with a 2.01-fold higher risk of mortality from diabetes mellitus (DM) compared to mild AGA. 23 However, our study did not specifically focus on early-onset AGA patients.
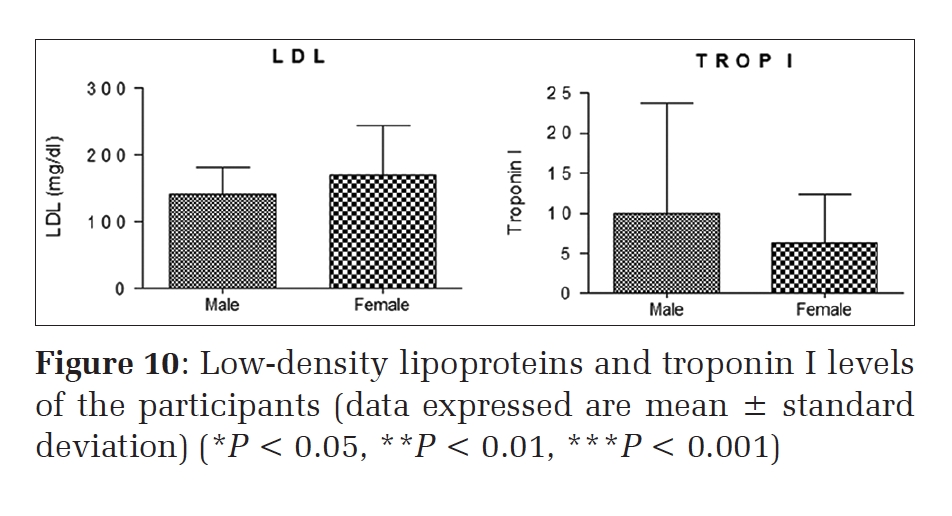
Triglyceride levels were elevated (>150 mg/dl) in 22.2% of the patients, with a mean value of 134.25 ± 5.4 mg/dl. Additionally, 28.3% of patients had HDL levels less than 40 mg/dl, with an average of 44.96 ± 0.87 mg/dl. These findings are consistent with previous studies, which also found low HDL levels and high triglycerides in patients with AGA. 26 Numerous studies have shown that androgens reduce HDL cholesterol levels, and changes in lipid profiles are associated with an increased risk of atheroma and atherothrombosis. As such, early detection and treatment of dyslipidemia in AGA patients is crucial to reduce the risk of cardiovascular events.
Blood pressure was another important parameter in our study. Systolic blood pressure (SBP) was greater than 130 mmHg in 34.3% of patients, with a mean SBP of 125.67 ± 9.93 mmHg. Diastolic blood pressure (DBP) was greater than 85 mmHg in 30.3% of patients, with a mean DBP of 82.49 ± 7.35 mmHg. These values align with the study by another researcher, where the average SBP was 125 mmHg and DBP was 85 mmHg. Furthermore, 34% of mild AGA patients and 40% of severe AGA patients had hypertension. These findings suggest that AGA may be related to subclinical vascular damage, especially in individuals with untreated hypertension, highlighting the importance of regular blood pressure monitoring in AGA patients.
Carotid intima-media thickness (CIMT) is a useful indicator of vascular health and a predictor of cardiovascular risk. The mean CIMT in our study was 0.538 ± 0.105 mm, which is consistent with the study by Harmeet Singh 26, 27, where the mean CIMT was 0.55 mm. A CIMT value of 0.8 mm is considered the threshold for increased stroke risk. Although only one patient in our study had a CIMT value of 0.8 mm, it is important to note that a 0.1 mm increase in CIMT corresponds to an 11% increase in the risk of myocardial infarction. 21
Finally, metabolic syndrome was observed in 7.1% of patients, all of whom had mild AGA. Patients with metabolic syndrome had significantly higher SBP, DBP, and FBS levels compared to those without metabolic syndrome. Specifically, the mean SBP in patients with metabolic syndrome was 135.71 ± 10.48 mmHg, while the mean DBP was 90.57 ± 12.9 mmHg, both significantly higher than those in patients without metabolic syndrome. The mean FBS was also elevated in metabolic syndrome patients (114 ± 3.96 mg/dl) compared to those without metabolic syndrome (93.15 ± 11.33 mg/dl).
Our study suggests a potential link between early-onset androgenetic alopecia and metabolic syndrome. The presence of hypertension, dyslipidemia, and elevated fasting blood glucose in AGA patients indicates the need for early intervention and management of these metabolic risk factors. Further research is necessary to explore the underlying mechanisms that connect AGA and metabolic syndrome and to determine whether early treatment of AGA can help prevent the development of serious systemic conditions.
Limitations:
Limitation of the current study was smaller sample size owing to limited time period. Individuals with other cardiovascular risk factors, such as hypertension, diabetes, hyperlipidemia, smoking, a sedentary lifestyle, and obesity were not excluded from the study These may operate as confounding factors which can potentially interfere with the true association between androgenetic alopecia (AGA) and cardiovascular disorders. Further multi-centric studies with larger sample sizes across the subcontinent, along with the elimination of confounding factors, will aid in establishing a true connection between early-onset AGA and cardiovascular risk. This will ultimately contribute to improving both the lifespan and aesthetic outcomes for patients.
Conclusion
Early onset male androgenetic alopecia, especially the more severe grades, can serve as a clinical marker for cardiovascular risks including metabolic syndrome, atheromatous plaques, hypertension, obesity and hyper-lipidemia. They should also be advised about the cessation of smoking and dietary and lifestyle modifications. Hence, patients with early onset male androgenetic alopecia should be screened for those cardiovascular risk factors and monitored for the same. This study will pave way for further studies with a larger sample size, to detect more such cardiovascular risk factors in early onset male AGA and their early recognition and treatment. As a result, the quality of life of the patients can be improved and the psychological burden can be reduced. This study encourages dermatologists to consider systemic health factors when managing AGA, potentially prompting the use of combination therapies to address both hair loss and associated metabolic concerns. This study could foster greater collaboration between dermatologists, endocrinologists, cardiologists, and other healthcare providers in managing patients with early-onset AGA and associated metabolic risks, ensuring a holistic approach to patient care.
Disclosure
Funding
None
Conflict of Interest
None