Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i02.001
Year: 2015, Volume: 1, Issue: 2, Pages: 1-8
Review Article
Shameem Shariff
Professor & Head, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India
Address for Correspondence:
Shameem Shariff, Professor & Head, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka,
India. E-mail: [email protected]
The journey of breast cancer a common malignancy the world over, is long drawn with several ups and downs finally resulting in patterns of management and therapy amounting to an attempt at breast conservation. Impressive advances have been made in the past 50 years in an effort to prevent, treat and cure breast cancer. Some of the major milestones include methods of screening modalities, newer classifications and a shift from mastectomy to breast conservation therapy. At most oncology centers the first line triple approach has come to mean tissue core biopsy instead of fine needle aspiration cytology, as the histological grade and receptor status can be easily defined and is closer to results obtained at resection. Imaging modalities like mammography have unmasked lesions whose biological behavior and association with cancer is not well defined - columnar cell hyperplasia, columnar cell change, flat atypia as well as complex sclerosing lesions. Reporting these on core biopsy pose a dilemma to, not only the pathologist, but also the treating physicians. Newer concepts like the molecular classification of breast carcinoma have overshadowed the conventional specific and not specific type. This encompasses the estrogen receptor (ER) positive and the ER-negative groups. Among the ER-positive are the luminal Types A and B with fairly good prognosis. Among the ER-negative group are the ones, which are Her2 neu positive and negative ones. The last group is the normal breast type, which is yet to be recognized as a specific entity. Such categories result in specific gene signatures of good prognostic and poor prognostic variants and response to targeted therapy.
KEY WORDS:Breast cancer, core biopsy, molecular classification
IntroductionCarcinoma breast is one of the most common malignancies affecting women in both the western world as well as in the subcontinent of India. In spite of all advanced modalities of therapy, the incidence seems to be on the rise. It becomes the responsibility of all treating physicians and reporting pathologists to keep abreast with knowledge of the changing patterns in this neoplasm. Advances in technology have resulted in the emergence of recording changes in cancer cell at a molecular level. This reflection in breast pathology has culminated in the emergence of newer techniques, terminologies and basis for a new classification, which might revolutionize not only the response to therapy, but prognosticate the behavior of the various types of breast carcinoma. This review aims at a visit into the changing trends in the pathology and diagnosis of breast neoplasia starting from screening to defining the molecular classification and prognostic parameters. Breast cancer is one of the leading causes of cancerrelated death in women worldwide. In the mideighteenth century Henri Francois Le Dran proposed that breast cancer originated as a localized disease that spread via the lymphatics to the general circulation. According to Donegran,[1] Le Dran’s recognition of the dominant course of breast cancer progression was pivotal and established the idea that surgery, if performed early, offered the potential to cure breast cancer. The journey of breast cancer since then has been long drawn with several ups and downs finally resulting in patterns of management and therapy amounting to an attempt at breast conservation. Impressive advances have been made in the past 50 years in an effort to prevent, treat and cure breast cancer. Some of the major milestones include screening modalities, a shift from mastectomy to breast conservation therapy, advances in chemotherapy for primary disease, antiestrogenic therapy for progression of breast cancer and target therapy at the molecular level. The following review will analyse some of these aspects. Pathologists form an important part in contributing information to therapeutic decisions. The complex multifactorial description of breast pathology now considered to be standard practice has resulted in the expansion of the report from a brief descriptive statement to a catalogue of data, which runs several lines. This has resulted in an active participation by the pathologists toward diagnosis and the awareness how various components of their report are relevant to treatment decisions. Triple Assessment: Changing Picture
Minimally invasive breast biopsies as a prong in triple assessment These are sampling of breast tissue using nonsurgical techniques; i.e., using a needle and are:
To use FNAC or core biopsy in diagnosing breast lesions is a dilemma for most clinicians, surgeons and probably even pathologists. Samples obtained by any of these methods are evaluated by pathologists and classified histologically with the primary goal of determining whether the lesion is benign or malignant. Evidence-based literature discussing which of these two modalities is preferable in breast lesion diagnosis is sparse, and there is no consensus among different specialized breast cancer centers. Each method has its advantages and disadvantages.[2-4] Fine-needle aspiration cytology
(National Health Service Breast Screening Program guidelines for cytology practice)[5]
Advantages of FNAC
Limitations of FNAC
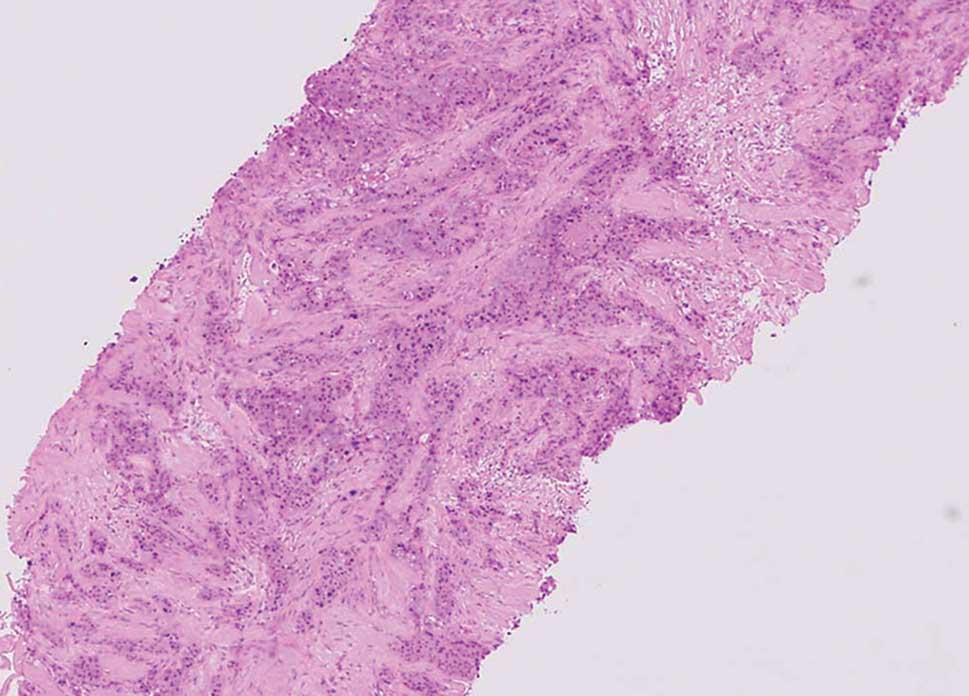
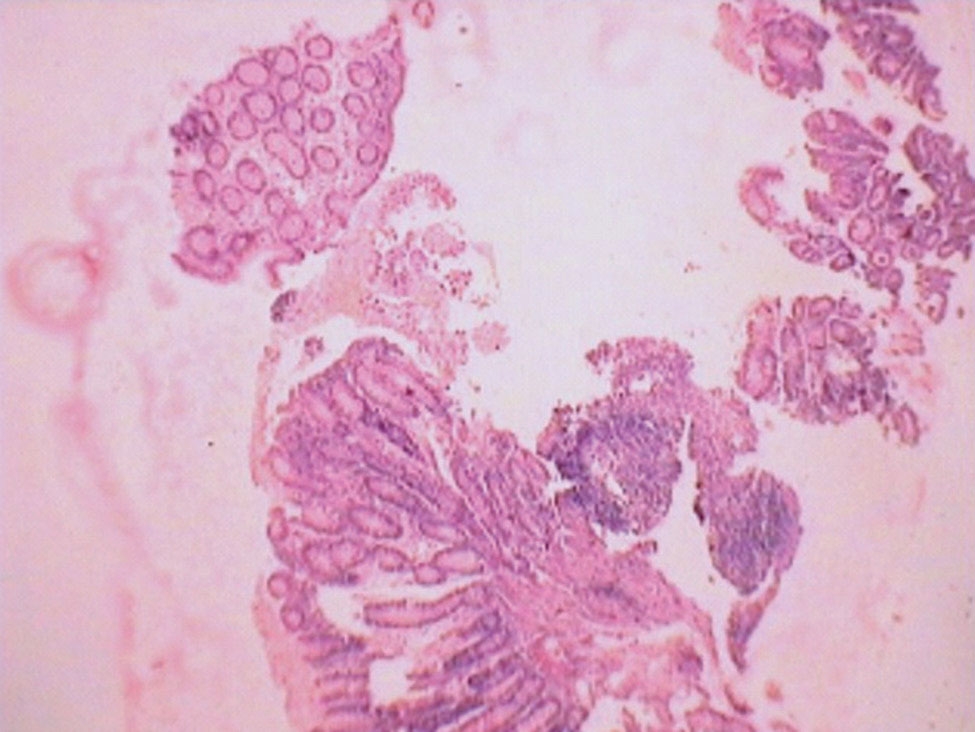
Needle Core Biopsy (NCB) This automated biopsy system obtains core needle samples. The device is pressed against the tissue at the appropriate location and angle and then the needle is fired into the tissue. After confirming that the core needle has sampled the appropriate tissue, the needle is withdrawn and the tissue sample ejected from the needle into a sample container. Some units use a co-axial needle, a canula is advanced into the tissue until it reaches the area to be sampled, the sampling needle is then fired through the canula into the lesion (Figures 1 and 2).
|
||||
|
||||
|
Classification system for the categorization of breast NCB: (UK scoring system)
Advantages of core biopsy
Limitations of core biopsy
Core biopsy over FNAC
Vacuum assisted biopsy
FNAC over core biopsy
Combined FNAC and core biopsy[9,10] There is controversy in the literature about the role of combining FNAC and NCB in the assessment of breast lesions. Some authors recommend combining the two techniques. FNAC may sample a larger or slightly different area of breast tissue than NCB, resulting in a smaller number of false negative cases when the two techniques are combined, as was evident in studies high lighting the importance of a multidisciplinary approach in the preoperative assessment of impalpable breast lesions-“quadruple approach!” Changing terminologies Atypical hyperplasia and DCIS The lack of consensus for differentiating between hyperplasia, atypical hyperplasia and carcinoma in-situ is confounded by several factors-inter observer reproducibility, definitions and criteria employed by various investigators and variability of the risk reported towards the development of cancer. One definition characterizes atypical duct hyperplasia as having “the cytologic and architectural features of the non-necrotic forms of intraductal carcinoma (IDC) and the changes may involve two or more ductules (but) the involved ducts/ductules measure < 2 mm in aggregated diameter.”[11] Others require “at least 2 spaces completely involved” by cells with appropriate cytologic features but do not include a measured dimension in their definition.[12] Differences also exist in regard to definitions of structural growth patterns designated micropapillary and cribriform, which are frequently seen in “nonnecrotic” variants of intrductal carcinoma and in hyperplasias. DCIS is characterized by proliferation of malignant epithelial cells, contained within the basement membrane of the mammary ductal tree. This definition only helps to define DCIS in relation to invasive carcinoma and applies to a morphologically well-defined lesion. The criteria for identifying low-grade DCIS and atypical ductal hyperplasias are still a grey zone and to differentiate these various lesions one from the other at morphology is unclear. On a routine hematoxylin and eosin stained slide, the minimum requirement for the diagnosis of DCIS is complete involvement of one or more duct cross-sections by uniform population of cells, the aggregate cross diameter of which exceeds 2 mm. Lesions displaying partial involvement of duct cross-sections of 2 mm or less in aggregate crosssectional diameter qualify as ADH. It is worth noting that the size criterion only applies for non-necrotic, low-grade variants of DCIS. DCIS is not a single entity. It is now considered as a heterogeneous group of lesions that differ in their growth pattern, histological, cytological features and biological potential. Therefore, the need arises for a classification system that takes into consideration clinical implications. The frequency of subsequent invasive carcinoma is considerably higher after IDC than after lesions usually diagnosed as hyperplasias or even atypical hyperplasias. A view was held that due to the problems in defining proliferative lesions and their diagnostic reproducibility, it was suggested by Tavassoli and workers that in a futile effort to distinguish between atypical hyperplasia and in-situ carcinoma; the lesions should be amalgamated into a term called mammary intraepithelial neoplsia or ductal intraepithelial neoplasia just as other organs like the cervix and vagina have a terminology such as CIN and VIN.[13] However, since its acceptance by WHO in 2003, this terminology has never become popular with either the reporting pathologists or the clinicians. The latter in particular seem to understand more clearly the concept of atypical ductal hyperplasia and carcinoma in-situ. Columnar cell lesions (CCLs)[14-17] CCLs of the breast are a group of lesions that have posed difficulties in interpretation to pathologists for years. They are characterized by the presence of columnar epithelial cells lining variably dilated terminal duct lobular units. The lining cells may be bland with no atypia or show changes, which may be mistaken for atypical ductal hyperplasia or DCIS. Luminal cells of these TDLUs in their simplest forms (columnar cell change) show apical snouts and luminal secretions with or without calcification. Columnar cell hyperplasia (CCH) refers to acini lined by more than two layers of columnar epithelial cells showing the abovedescribed changes along with the formation of micro papillae. CCL and CCH may display cytologic atypia termed as CCL with atypia and CCH with atypia respectively; together known as “flat epithelial atypia” formerly called as “clinging carcinoma.” These lesions generally show lowgrade atypia. High-grade cytologic atypia is not a feature of CCLs and is always diagnosed as high-grade DCIS. Recently, there has arisen a pronounced interest in these lesions because they are being encountered with increasing frequency in breast biopsies performed for the presence of mammographic microcalcifications. The clinical significance of these lesions unfortunately is not fully understood, and the lack of uniformity in diagnostic criteria has further complicated issues. CCLs are found to be associated with tubular carcinomas and lobular carcinoma in-situ and their presence in core biopsies should be viewed with caution as the full spectrum of surrounding changes cannot be viewed. CCLs are ER and PgR positive, basal cytokeratin (CK5/6 and CK14 negative), exhibit low numbers of genetic alterations, features that are similar to those of low grade in-situ and invasive carcinoma. In addition, common chromosomal alterations between CCL and more advanced atypical lesions within individual terminal duct lobular units suggest a common molecular evolution. These data further support the hypothesis that CCLs are an intermediary step in the development of some forms of low grade in-situ as well as invasive lobular and ductal carcinomas. Radial and complex sclerosing scars[18] These are complex sclerosing lesions, which are being increasingly picked up on mammographic guided biopsies because of their resemblance to microcarcinomas on imaging. They are associated with a sclerotic center with radially arranged spokes of epithelial proliferation. Smaller lesions are called radial scars and those above 1 cm as complex sclerosing lesions. About 10-20% of these are known to be associated with carcinomas. Molecular markers in breast carcinoma Molecular markers in breast carcinoma are used to identify subsets of tumors with significant prognostic and therapeutic implications. Ancillary IHC studies for hormone receptors (HRs) such as ER, PR, and HER2, act as prognostic or predictor indicators in breast cancer and are the most commonly used and are mandatory to be performed in every breast cancer report. Breast carcinoma is highly heterogeneous at both the clinical and molecular level. Therefore, separating breast cancer into various subsets based on its biological behavior for therapeutic options is helpful. Progesterone receptors serve as an indicator of an intact ER pathway, which reflects the dependence of the ER/PR axis and predicts which patients will respond to hormone therapy because adequate estrogen levels are required to transcribe PR. Accurate and quantitative assessment of HRs is critical when using IHC studies. Several factors influence results and have to be kept in mind while standardizing procedures. ER and PR receptor status is reported either by the Macarthy’s histoscore[19] or by the American Society of Clinical Oncology and College of American Pathologists (CAP). Criteria:[20] Both methods take into consideration the intensity of the nuclear stain as well as percentage of cells stained. Her2 neu is generally performed by IHC,[19] FISH or presently even by the reverse transcriptionpolymerase chain reaction (RT-PCR). IHC scores with 2+ result should always be ratified by the FISH technique. Based on the expression of various gene sets, the researchers have categorized breast cancers into 5 subsets with prognostic significance, such as the luminal A, luminal B, HER2 overexpressing, basal –like, and normal breast-like subtypes. Molecular subtypes of breast carcinoma[20] Luminal subtypes The high expression of the genes normally expressed by luminal epithelium resulted in the names of luminal subtypes. The luminal tumors express CK8/18, GATA3, and ER related genes, which is why they are designated as the ER+ group. The estrogen receptor is highly expressed in luminal Type A tumors with low levels of proliferationrelated genes resulting in a usually low histologic grade and excellent prognosis. The estrogen receptor is expressed in lower levels in luminal Type B tumors, with higher proliferation-related genes, often resulting in a higher histologic grade and a significantly worse prognosis. A significant number of HER2 overexpressed, ER+ cancers fall into the luminal B category, rather than the HER2 subtype. HER2 subtypes Tumors in this group are characterized by amplification of ERBB2 (formerly HER2) genes on band 17q12. These tumors often demonstrate 3+ HER2 IHC staining and are completely negative for ER and PR. Therefore, as mentioned previously, the HER2 overexpressed but ER+ tumors would best fit into the luminal B category. The HER2 subtype tends to have an aggressive clinical course. Basal - like subtypes These tumors express basal/myoepithelial cell genes, such as CK4, CK14, CK17, caveolins 1 and 2, nestin, P- cadherin, CD44, and EGFR. In addition, they are usually triple-negative tumors for ER, PR and HER2. A few cases harbor EGFR gene amplification or aneusomy as well as KIT gene expression. This subtype has also been noted to have an aggressive clinical behavior with high histologic grade, high proliferative index, metaplastic areas, central necrosis, pushing borders, and a prominent lymphocytic infiltrate. Basal-like tumors are more commonly found in women of Hispanic or African descent and show a high response rate to chemotherapy. The immunohistochemical and morphologic features of basal-like tumors are similar to those arising in women with BRCA1 germline mutations because of abnormalities in the BRCA1 pathway. However, most women with basal-like carcinomas do not have germline BRCA1 mutations. Breast like subtypes These tumors often express adipose tissue and other nonepithelial cell genes, including basal cell genes, and typically cluster with healthy breast and fibroadenomas. The clinical significance of this group has yet to be determined. However, some researchers have proposed that this subtype was misrepresented because of poor tissue sampling, creating a false category. Gene expression profiling Gene expression profiling is a method of providing vast amount of information about carcinoma, their behavior and prognostic factors. Patterns of gene expression and their interpretation predict the metastatic potential of these malignancies. Perou et al. proposed the first molecular classification of breast cancer using gene expression analysis on DNA microarrays. The intrinsic gene set, or the genes in which the expression patterns were analyzed, were characteristic of a specific tumor. Thus emerged by these studies the molecular subtypes of carcinomas outlined above with studies characterizing a group of genes which were related to the ER pathway, PR pathway or even metastatic potential. Predictive gene sets which are currently available are MammaPrint (Amsterdam) and Oncotype Dx (Genomic Health Insurance, California). The mammaprint was the first prognostic gene set available in clinical practice and was developed in Amsterdam. It is based on a 70 gene set profile using an oligonucleotide array. This gene set helps in deciding whether the patient should receive adjuvant chemotherapy. The oncotype DX is another commercially available RT-PCR based assay which provides a recurrence score (RS) based on a 21 gene panel associated with cancer prognosis. The test has been shown to provide predictive and prognostic information in ER+, lymph node-negative tumors by providing a RS value, which varies from 0 to 100 and predicts the risk of a 100 years recurrence. Patients who have a low score, < 18; intermediate score 18-31; and high score 31 or greater. Patients with a high score will benefit from chemotherapy. |
||||
ConclusionThe approach to diagnosis of breast carcinoma, the unmasking of grey zones due to screening by mammography and the end result of such new lesions discovered have prompted variations and newer insight into the pathology and management of this cancer. A new molecular classification has resulted in targeted therapy and the gene signatures obtained by these molecular techniques prognosticate their behavior and response to treatment. |
Subscribe now for latest articles and news.