Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 52-58
Original Article
Puja Kumari Jha1 , Narendra Singh Ranawat2 , Rajesh Ranjan2 , Rafat Sultana Ahmed1 , Rajnish Avasthi3 , Ashok Kumar Ahirwar1
1Department of Biochemistry, University College of Medical Sciences & Guru teg Bahadur Hospital, Delhi-110095, India,
2Department of Medicine, Jaipur Golden Hospital, Delhi-110085, India,
3Department of Medicine, University College of Medical Sciences & Guru teg Bahadur Hospital, Delhi-110095, India
Address for correspondence: Rafat Sultana Ahmed, Department of Biochemistry, University College of Medical Sciences & Guru teg Bahadur Hospital, Delhi110095, India.
E-mail: [email protected]
Objective: The metabolic syndrome (MetS) may be responsible for occurrence of high frequency of cardiovascular disease in rheumatoid arthritis (RA) patients. An association between inflammatory activity of RA and MetS has also been speculated. This study was designed to see whether presence of MetS along with RA increases the severity of disease and to find the risk association of the disease severity markers of RA namely TNF-α, anti-CCP, RF, CRP and ESR with MetS. Methodology: 185 patients of RA (EULAR 2010) were recruited and assessed for MetS according to NCEP/ATP III criteria. Serum level of disease specific biomarkers of RA namely TNF-α, anti-CCP, RF, CRP and ESR were quantified in all patients and compared between RA with MetS and only RA patients. Cytokine TNF-α, anti-CCP, RF, and CRP were assayed through ELISA. Results: The prevalence of MetS among RA patients was 41.2%. The mean age of RA cases with MetS is significantly older (55.65yrs) with increased disease duration. The levels of TNF-α, anti-CCP, CRP and ESR along with EULAR & DAS score were significantly (p<0.05) high in RA with MetS. TNF-α showed maximum risk (OR=6.3; p=0.03) in development of MetS. Longer disease duration with high anti-CCP, CRP and DAS-28 were also contributing significantly in MetS development. Conclusion: A positive vicious cycle is working between the pathogenesis of RA and MetS through inflammatory cytokines and biomarkers. MetS in RA is associated with increased disease severity.
Keywords: Rheumatoid arthritis, Metabolic syndrome, Biomarkers, Cytokine TNF-α, Disease severity
Rheumatoid arthritis (RA) is a chronic inflammatory disease associated with increased disability, morbidity and mortality.[1] Cardiovascular disease (CVD) has been found as the most important cause of mortality in patients of rheumatoid arthritis (RA).[2] Therefore, the European League against Rheumatism had recommended urgent screening and management for cardiovascular risk in patients diagnosed with RA.[3] The development of accelerated atherosclerosis and increased risk of cardiovas cular disease in patients with RA may be influenced by occurrence of metabolic syndrome (MetS). [4] Metabolic syndrome describes a constellation of major risk factors for cardiovascular diseases such as atherogenic dyslipidemia, obesity, hypertension, and diabetes mellitus. It is measured in terms of waist circumference, triglyceride levels, fasting blood glucose and high-density lipoprotein (HDL) level. The underlying pathogenesis for MetS is thought to be insulin resistance.[5]
The probable accelerated pathogenic mechanism behind development of MetS in RA may be attributed to the following: (1) Increased production of proinflammatory cytokines in RA leading to insulin resistance, (2) Use of Glucocorticoids or other treatment modality and (3) Reduced physical activity due to joints involvement and resulting increase in body mass index (BMI).[6,7] Further, old age, positive serology and extra articular manifestation increases the risk of occurrence of MetS in patients of RA. [8]
Additionally, MetS itself is responsible for release of various adipokines and inflammatory cytokines that may further aggravate the severity of disease and morbidity in RA in patients.[9] Asian Indians are a metabolically disadvantaged ethnic group with high prevalence of obesity, diabetes mellitus and dyslipidemia.[10] The reported prevalence of RA in Indian population as per criteria of revised American College of Rheumatology (ACR) is 0.75%.[11]
Many studies have reported that the prevalence of the MetS is significantly higher in patients with RA, as compared with the general population. The worldwide reported prevalence for MetS in RA cases was 30.65%.[12] The prevalence of MetS in RA cases in Indian population has been reported between 16.7 to 57.4 %. Higher prevalence of MetS in RA cases was noted in south Indian population as compared to north and northeast India.[13–15] But to the best of my knowledge there are very limited studies considering the relationship of disease activity, severity, serum levels of inflammatory cytokines with disease biomarkers and disease duration aspects of RA with MetS in Indian Population.
This study was designed to evaluate the correlation between metabolic syndrome and disease severity of RA and thus clinical status and overall health of RA patients. We attempted to see whether presence of MetS along with RA increases the severity of disease in terms of serum levels of biomarkers of RA namely TNF-α, anti-CCP, RF, CRP and ESR or not along with the prevalence of MetS in RA in north Indian population.
This case control study was conducted at two places first one is University College of Medical Sciences and Guru Teg Bahadur Hospital (a tertiary care teaching hospital), Dilshad Garden, Delhi and second one is Jaipur Golden Hospital, Rohini, Delhi. The study was executed in the department of Biochemistry and Medicine during 2017-2020. Subjects were recruited from Medicine OPD of both the hospitals. The study was approved by the Institutional Ethical Committee for Human Research (IEC-HR) and written informed consent was taken from every participant. The study was conducted in accordance with the principles of Declaration of Helsinki.
Patients of RA were diagnosed as per EULAR (European League against Rheumatism), 2010 criteria. One hundred eighty-five (185) RA patients fulfilling EULAR-2010 criteria and above 18 years of age were recruited for the study[16] . The observed overall pooled prevalence of metabolic syndrome in RA patients was 30.65%,[12] considering this prevalence as reference, the minimum required sample size with 10% margin of error and 5% level of significance is 82 patients.
Formula for calculation of sample size applied: N ≥((p(1 -p))/(ME/zα ) 2 Where Zα is value of Z at two-sided alpha error of 5%, ME is margin of error and p is prevalence rate.
Presence of MetS were defined according to National Cholesterol Education Program /Adult Treatment Panel III (NCEP/ATP III) criteria (2004) that is based upon abnormality in any three among following parameters that is Waist circumference (≥102 cm in men; ≥88 cm in women), Triglycerides (≥150 mg/dl) HDL-c (< 40 mg/dl in men; < 50mg/dl in women), Blood pressure (≥130/85 mmHg) and Fasting blood glucose (≥100 mg/dl).
185 RA Cases were categorised into RA without Metabolic syndrome (108) and RA with metabolic syndrome (77) depicted in Tables as Group I, RA (n=108) and Group II, RA + MetS (n=77).Two hundred (200) age and sex matched Non RA controls were recruited in the study.
The possible confounders were attempted to nullify by excluding the subjects having history of alcoholism, smoking, hypertension, endocrinal disorders specially thyroid abnormalities, deranged renal function, cardiac disease, chronic lung disease, pregnancy, current malignancy, any other chronic inflammatory conditions and patients with other diseases or treatment that may lead to dyslipidemia.
These controls were just to compare the prevalence of metabolic syndrome in RA cases and in non RA north Indian population. The rest of the study was focused on evaluating the correlation between metabolic syndrome and disease severity of RA and thus clinical status and overall health of RA patients. Therefore the RA cases were categorised into RA with Metabolic syndrome and RA without metabolic syndrome.
A detailed history regarding disease duration and co-morbid condition, anthropometric measurements and clinical parameters along with available treatment details of the selected cases were noted as per pre-recorded Performa. Anthropometric measurements included Height in centimeter (Harpendens Stadiometer), weight in kilograms (kg) (model SECA 708), Waist circumference in centimeter and Body Mass Index (BMI).BMI was calculated by formula using weight (kilogram) divided by height in square meter. {Weight (kg) / Height (m) 2}. Blood pressure was measured with Welch Allyn Aneroid sphygmomanometer by taking average of two readings at 5 minute apart. European League against Rheumatism (EULAR) score and Disease activity score (DAS-28) were calculated also as per standard protocol.[17] DAS-28 calculation requires assessment of 28 joints for tenderness and swelling, ESR value and a visual analogue scale of well-being according to patient.
Blood sample collection was executed in fasting condition of participants. Sampling was done with proper aseptic precautions and collected into EDTA fluoride and plain vials for complete blood count (CBC), biochemical parameters, biomarkers of disease and cytokine level. In case of diabetic patients the interval between insulin administration and sampling was taken for at least 12 hours. Routine biochemical investigations such as plasma glucose (fasting and post prandial), kidney function test (urea and creatinine), uric acid, lipid profile test and liver function test were determined by standard laboratory methods using commercial kits carried on auto analyzer UnicelDxC 600, Synchron Clinical System from Beckman Coulter Pvt. Ltd., USA. CBC was determined on Mythic 18 blood cell counter. Modified Westergreen method was used for Erythrocyte Sedimentation Rate (ESR) estimation.
Assay for IgG antibodies to citrullinated protein (anti-CCP) and rheumatoid factor (RF) were done by ELISA (Enzyme Linked Immunosorbent Assay) with the use of commercial kits (Omega Diagnostics Ltd, Alva, UK). TNF-α was estimated by using ELISA kit from Diaclone diagnostics (France). CRP level was measured by standard ELISA kit (Ray Biotech, Norcross GA). Assay of each parameter was carried out in duplicate.
The collected data was analyzed statistically with the help of SPSS-16 software. The categorical measurands were presented as percentages and frequencies whereas continuous measurands were presented as mean ± Standard deviation (SD). Categorical measurands between two groups were compared using chi-square test whereas continuous measurands were compared using unpaired t test. p value <0.05 was considered statistically significant. Multivariate logistic regression analysis was done to determine the risk associated with serum level of individual disease marker of RA in development of MetS with 95% confidence interval (CI) and odds ratio calculation. The correlation between individual RA severity biomarkers and components of MetS were analyzed by application of spearman’s correlation and derivation of “r” value.
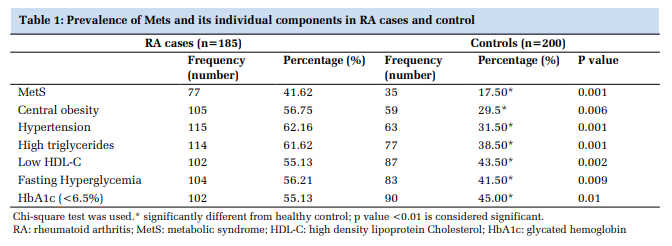
The prevalence of metabolic syndrome (MetS) and its individual components in RA cases and Controls have been presented in Table 1. MetS was prevalent in 41.6% cases of RA. All the individual components of MetS were significantly higher in cases as compared to controls. But the frequency of hypertension and high triglyceride level were most common and significant (Table 1). Though glycated hemoglobin (HbA1c) is not a component of MetS, but lower value (<6.5%) was more prevalent in RA cases.
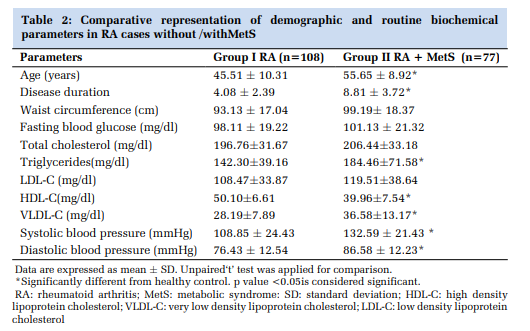
The comparative picture of demographic and routine biochemical parameters of RA cases with presence or absence of MetS were depicted in Table 2. The mean age of RA cases presenting with MetS is significantly older (55.65yrs) as compared to RA without MetS (45.51 yrs). Disease duration was also significantly longer (8.81 ± 3.72yrs) in RA cases presenting with MetS compared to RA without MetS (4.08 ± 2.39). Triglycerides along with both systolic and diastolic blood pressure were found to be significantly high in RA cases with MetS whereas HDL-C level was significantly reduced (Table 2).
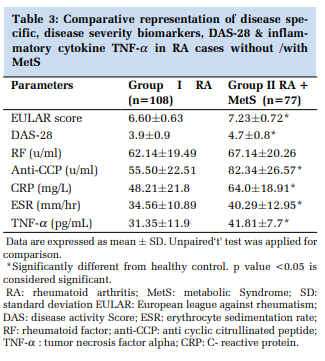
The disease specific, severity, activity markers along with inflammatory cytokine level were compared in Table 3. The mean serum level of CRP, ESR and anti-CCP was 64.0±18.91mg/L, 40.29±12.95mm/hr and 82.34±26.57 U/ml respectively and significantly elevated in presence of MetS. The higher mean of DAS-28 (4.7±0.8), elevated level of inflammatory cytokine TNF-α (41.81±7.7pg/ml) with high EULAR score (7.23±0.72) were characteristics of RA with MetS (Table 3).
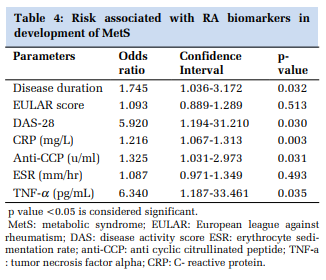
The risk associated with different parameters in development of MetS was represented in Table 4. Significant association was found with disease duration (Odds ratio: 1.745; p=0.03), DAS-28(Odds ratio: 5.920; p=0.03), CRP (Odds ratio: 1.216; p=0.003), Anti-CCP (Odds ratio: 1.325; p=0.03), TNF-α (Odds ratio: 6.340; p=0.03) in RA cases with MetS.
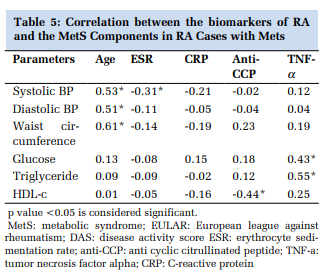
The overall correlation among biomarkers of RA cases with MetS components were depicted in Table 5. Age of the individual was positively correlated with systolic, diastolic and Waist Circumference. Inflammatory cytokine TNF-α has a significantly positive relation with fasting blood glucose and triglyceride(r= 0.432; r= 0.543 respectively), whereas anti-CCP has a negative relation with HDLc(r= -0.442)
This study was designed to evaluate the contribution of metabolic syndrome in disease severity of RA along with prevalence of metabolic syndrome in cases of RA as compared to non RA controls. The frequencies of individual components of MetS were also evaluated in RA. We also attempted to explore the risk conferred by disease biomarkers and disease severity state in development of MetS. The correlation between individual components of MetS and disease biomarkers of RA (specific & severity markers), was also assessed.
The prevalence of MetS in RA cases was found to be 41.6% in north Indian population. We had considered the modified ATPIII Criteria of MetS for adult Asian Indian where the cut-off for fasting blood glucose is accepted at 100mg/dl rather than 110mg/dl.[18]A cohort study from north India has reported the prevalence of MetS slightly less of 35.1 % with application of modified ATP-III criteria.
However, the reported prevalence from south Indian population of RA was 57.4%, higher than recorded in our cases.[13–15] Our study also confirms the finding that Indian population is more prone for metabolic syndrome as worldwide prevalence of MetS is significantly lowers approximately 30.65% only.[12] When we assessed the prevalence of individual components of MetS (WC, HDL, BP, Triglyceride and FBS) in RA cases, high blood pressure (more than 130/85) had the highest prevalence (Table 2).
This is consistent with the study conducted by Panoulas VF, Douglas KM et al.[19] Higher number of MetS in RA cases with more than 55 yrs and longer disease duration is indicating the significance of inflammatory burden leading to evolution of metabolic derangements. High Triglycerides with reduced HDL-C were more prevalent in established RA cases with MetS (Table 2).
The disease specific, severity and activity scores along with inflammatory cytokine level TNF-α were compared in Table 3. The pro-inflammatory nature of TNF-α leads insulin resistance, characteristic dyslipidemia and endothelial dysfunction and ultimately a chronic inflammatory state that leads to MetS.[20] Pro-inflammatory cytokines are major contributory factor in development of atherosclerosis and thus CVD. TNF- α also increases the production of acute phase reactants namely CRP; this hypothesis is also supported by our findings (Table 3). Further increased anti-CCP with high DAS-28 Score and EULAR score are associated with joint deformity and disease severity.[21] There are reports suggesting beneficial role of Infliximab and Methotrexate on reduction of anti-CCP level in RA patients and TNFα had been found responsible for generation of anticitrullinated peptide antibody.[22]The risk associated with different biomarkers of RA in development of MetS was represented in Table 4. The highest odd ratio of TNF- α in MetS development in RA cases is self explanatory. Though some studies have reported no association between DAS-28 and MetS development in RA cases but our study reported a significant risk with DAS-28.[23]
The correlation analysis of disease biomarkers of RA with individual components of MetS showed that inflammatory cytokine TNF-α has a significantly positive relation with fasting blood glucose and triglyceride. TNF-α induces lipolysis in adipose tissue and it also affects the glucose uptake in skeletal muscle. Increased release of free fatty acids from adipocytes aggravates the insulin resistance.[24] The anti-CCP had a negative relation with HDL-c. Citrullinated epitopes were found to be present in the atherosclerotic plaques that were targeted by antiCCP antibodies. Thus high anti-CCP with reduced HDL-c is in agreement with progressive CVD risk in RA cases with or without MetS.[25]
This study demonstrates that pro inflammatory cytokine TNF-α by augmenting the insulin resistance involved in development of MetS. A positive vicious cycle is working between the pathogenesis of RA and MetS through inflammatory cytokines and disease biomarkers. MetS in RA is associated with increased disease severity. Detailed study is require to find that how high level of TNF-α and other disease biomarkers leads to insulin resistance and thus metabolic syndrome.
The study of pro-inflammatory cytokine gene polymorphism in RA cases with MetS and to look for their possible association with individual components of MetS.
The authors declare that there is no conflict of interest.
Subscribe now for latest articles and news.