Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.23.334
Year: 2024, Volume: 10, Issue: 1, Pages: 1-7
Original Article
Swarupa Malla1 , Sailaja Suryadevara2 , Pallivilla Umarani3 , Gudeli Vahini3
1Resident, Alluri Sitaramaraju Academy of Medical Sciences, 534005, Andhra Pradesh,
2Associate Professor, Alluri Sitaramaraju Academy of Medical Sciences, 534005, Andhra Pradesh ,
3Professor, Alluri Sitaramaraju Academy of Medical Sciences, 534005, Andhra Pradesh
Address for correspondence:
Pallivilla Umarani, Professor, Alluri Sitaramaraju Academy of Medical Sciences, 534005, Andhra Pradesh .
E-mail:
[email protected]
Received Date:10 October 2023, Accepted Date:11 January 2024, Published Date:30 March 2024
Introduction: Breast carcinoma is the largest cause of mortality from cancer among women in India. Tumor budding is usually defined as isolated single cancer cells or clusters of up to four cancer cells located at the invasive tumor front. Tumor budding is associated with poor clinicopathological characteristics, such as Tumor size, tumor differentiation, lymph node invasion, lymphatic or vascular invasion etc. Aim: To study tumor budding and its association with known clinicopathological parameters and hormone receptor status in invasive breast carcinoma. Methods : A Cross-sectional study was conducted after approval from the ethics committee. The duration of study was 1.5 years (Jan 2022- June 2023). Results: A total of fifty cases of invasive breast carcinomas were included in this study. 70% (35cases) were >50yrs of age, 65% (33cases) were of T2 (tumor size) category. 82%(41cases) of Invasive duct carcinoma, No specific type, 12% (6 cases) of mixed carcinomas followed by three cases, one is invasive lobular carcinoma(6%), others are high grade papillary duct carcinoma(6%) and mucinous carcinoma (6%). 76%(38cases) showed presence of lymphovascular invasion, 74%(37cases) showed absence of necrosis, 54%(27 cases) are categorized as grade 2. High grade tumor budding was seen in 54% (27 cases). Conclusion: The following variables had a significant association with the tumor budding in present study: Tumor size, TNM staging, treatment status, lymphovascular invasion showing a p-value of <0.05. ER positive tumors are also associated with high grade tumor budding.
Keywords: Breast Carcinoma, Clinicopathological Variables, Lymphovascular Invasion, Tumor Budding
Breast carcinoma is the most common cancer among women in India. Breast cancer is a heterogeneous disease with different molecular subtypes. Tumor budding is a prognostic entity which has been identified as a prognostic factor in carcinomas associated with epithelial mesenchymal transition 1. Tumor budding is defined as small group of cells (upto 4 - 5 cells), detached from the tumor bulk 2.
Tumor budding is associated with various clinicopathological characteristics like age, laterality, tumor size, tumor grade, histological subtypes, inflammation, lymph node and, lymphatic/vascular invasion, ER, PR, Her2Neu, treatment status, pTNMstaging 3, 4, 5. Tumor buds are helpful in predicting the response to neoadjuvant chemotherapy in breast carcinoma patients 5.
TGF-β signaling pathway plays an important role in tumor budding through invasion and metastasis in breast carcinoma. MMP9 is a downstream effector of TβR1. Inhibition of MMP-9 can prevent TβR1 induced EMT and thus reduces cell invasion and metatsasis 6.
The number of tumor buds is categorized as low grade (≤ 20 tumor buds/10 HPF) and high grade (>20 Tumor buds / 10HPF) 7. Tumors with high grade budding have a significantly more aggressive clinical course. Significance of tumor budding has mainly been studied in colorectal carcinoma 8.
The association of lymphovascular invasion and tumor budding led to the postulation of their involvement in the early metastatic process owing to epithelial-mesenchymal transition (EMT) 9. In most of the studies, the assessment of tumour budding seems to identify the behavior of cancer, and facilitates treatment planning 10. In cases involving significant inflammatory cell infiltration, immunohistochemical methods increase the confidence of the assessment and the inter-observer agreement 11 .
Regarding breast cancer, multiple studies revealed that budding was correlated with larger tumour size, lymphovascular `embolisation, lymph nodal metastasis and lower five year survival 12. High grade tumor budding is an independent risk factor for metastasis 13, 14.
Assessment of the tumor budding in routine pathological slides, is relatively simple and may be readily incorporated into routine histopathology reporting. It improves risk stratification particularly in patients with node negative breast cancer 15.
Aim: To study tumour budding and its association with known clinicopathological parameters and hormone receptor status in invasive breast carcinoma.
Objectives:
To identify tumor budding in invasive duct carcinoma breast.
To grade the tumor budding into high and low grade tumor buds.
To estimate the association between tumor budding with known clinicopathological parameters and hormone receptor status.
A cross-sectional study was conducted after approval from the ethics committee (Approval no. 155/2023). The duration of study was 1.5 years (Jan 2022- June 2023).
Inclusion Criteria
All female breast carcinoma (mastectomy & lumpectomy) specimens received by department of pathology.
Exclusion Criteria
Trucut specimen
Needle core biopsies.
Inadequate specimen.
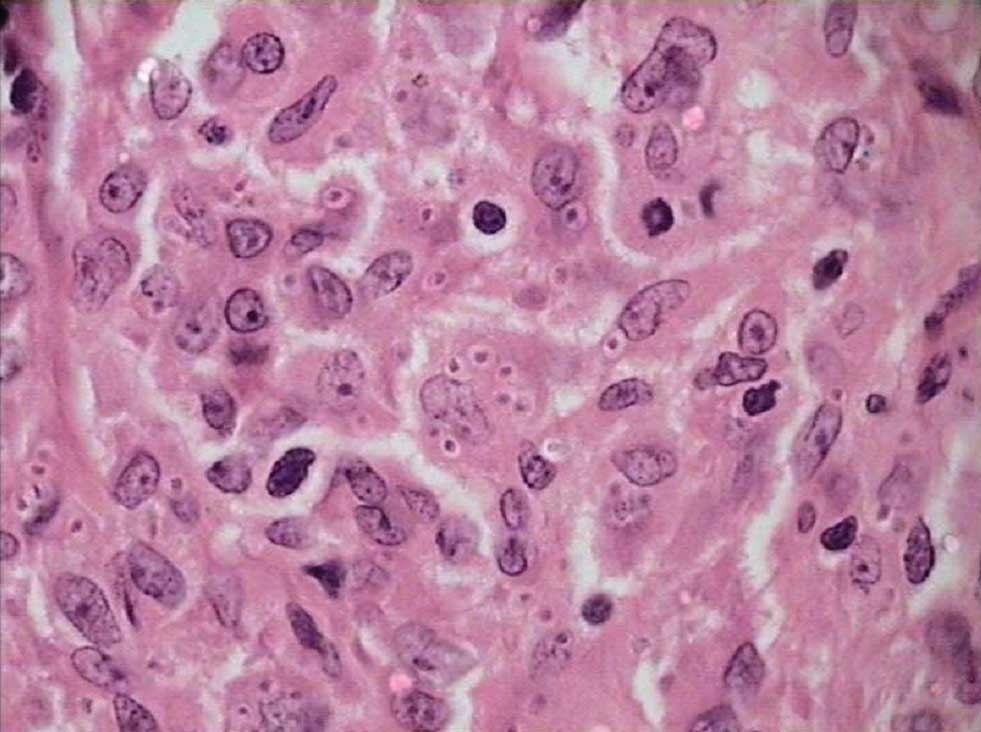
The tissues were subjected to routine paraffin embedded processing. 3-4 micrometer thick sections were cut, using a microtome and mounted on to glass slide. The sections were stained using hematoxylin & eosin and evaluated for the tumor buds followed by grading.
To grade breast tumors, we used the Nottingham modified Bloom Richardson method, followed by WHO categorization of breast cancer. Tubule development, nuclear grade, and mitosis were included in this Bloom-Richardson (BR) grading.
A poly-l-lysine coated slide with section was dewaxed, antigen retrieval was performed, and the section was incubated with sp1clone rabbit monoclonal antibody against ER (estrogen receptor), Her2 (human epidermal growth factor receptor 2), PR(progesterone receptor) antigens. TheDiaminobenzidine (DAB) chromogen counterstain was used in the last phaseof HRP polymerization. The Allred score was used for ER/PR markers, whereas the American Society of Clinical Oncology's criteria of 2016 for Her 2/neu in the reporting process.
Sections showing tumor proper with adjacent normal tissue were located in scanner view and tumor buds are identified at low power view(10x). Tumor buds were further classified into High grade tumor budding (tumor buds ≥ 10 /10 HPF) and low grade tumor budding (tumor buds < 10 / 10 HPF), at high power view(40x).
Mimickers of tumor buds like inflammatory cells, multinucleated giant cells, fibroblasts, endothelial cells, smooth muscle cells and artifacts were excluded by examining under high power (40x). IHC for Pan cytokeratin is done for mimickers of tumor buds where ever necessary.
The chi-square test, fissure exact test was used to examine tumor budding, clinicopathological characteristics, and hormone receptor status. It was determined that a p-value of <0.05 was considered statistically significant.
The presence of tumor buds is associated with various clinicopathological variables such as age group, laterality, tumor size, tumor grade, histological subtypes, lymphovascular invasion, necrosis, lymphnode status, pTNM staging, tumor grade, inflammation and ER, PR, Her2Neu status.
A total of 50 cases of invasive breast carcinomas were included in this study. 70%(35cases) were of age group >50yrs and 30%(15 cases) of <50yrs. Out of 50 cases, 65% were of T2 category followed by 14% of T1 and T3 each, along with 6% of T4 category. 82% were of invasive duct carcinoma, no specific type (41cases),12% of mixed carcinoma (6cases) followed by threecases of invasive lobular carcinoma (6%), high grade papillary duct carcinoma(6%) and mucinous carcinoma (6%).
52% (26cases) and 48% (24 cases) involved right breast and left breast respectively. 92% (46 cases) primary breast carcinoma cases and 8% (4 cases) post neo-adjuvant chemotherapy cases were observed. 76% (38cases) showed presence of lymphovascular invasion. 74% (37cases) showed absence of necrosis. Equal distribution of presence and absence of lymph node metastasis in 46% (23cases) was observed whereas in 8% (4 cases) lymph nodes were not submitted.
54% (27 cases) were of grade 2 followed by 37%(18 cases)of grade 1 and 9%(5 cases) grade 3. 61%(31 cases) were distributed in stage II of clinical TNM classification whereas 30% (15 cases) and 9%(4 cases) were distributed in grade I and grade III respectively.
|
Prognostic Factor |
Tumor Budding |
Observation |
p-Value |
|||
|
Age |
|
< 50 Years |
⩾50 Years |
|
|
0.37 |
|
Low |
21%(4) |
79%(15) |
|
|
||
|
High |
37%(10) |
63%(17) |
|
|
||
|
Absent |
50%(2) |
50%(2) |
|
|
||
|
Tumor size |
|
T1 |
T2 |
T3 |
T4 |
0.01 |
|
Low |
10.5%(2) |
58%(11) |
21%(4) |
10.5%(2) |
||
|
High |
4.4%(2) |
73.9%(21) |
13%(3) |
8.6%(1) |
||
|
Absent |
75%(3) |
25%(1) |
0 |
0 |
||
|
Tumor grade |
|
Grade 1 |
Grade 2 |
Grade 3 |
|
0.11 |
|
Low |
36.8%(7) |
42.1%(8) |
21.1%(4) |
|
||
|
High |
29.6%(8) |
66.7%(18) |
3.70%(1) |
|
||
|
Absent |
75%(3) |
25%(1) |
0 |
|
||
|
Necrosis |
|
Present |
Absent |
|
|
0.42 |
|
Low |
31.5%(6) |
68.5%(13) |
|
|
||
|
High |
26%(7) |
74%(20) |
|
|
||
|
Absent |
0 |
100%(4) |
|
|
||
|
Lymphovascular invasion |
|
Present |
Absent |
|
|
0.03 |
|
Low |
73.6%(14) |
26.4%(5) |
|
|
||
|
High |
85.2%(23) |
14.8%(4) |
|
|
||
|
Absent |
25%(1) |
75%(3) |
|
|
||
|
Lymphnode Metastasis |
|
Present |
Absent |
Not submitted |
|
0.20 |
|
Low |
68.8%(12) |
31.2%(7) |
0 |
|
||
|
High |
34.8%(10) |
56.5%(14) |
8.7%(3) |
|
||
|
Absent |
25%(1) |
50%(2) |
25%(1) |
|
||
|
TNM Staging |
|
Stage I |
Stage II |
Stage III |
|
0.0001 |
|
Low |
0 |
62.5%(12) |
37.5%(7) |
|
||
|
High |
4.3%(1) |
65.2%(18) |
30.5%(8) |
|
||
|
Absent |
75%(3) |
25%(1) |
0 |
|
||
|
Treatment status |
|
Primary Infiltrative breast ca |
Post neo-adjuvant chemotherapy |
|
|
0.002 |
|
Low |
89.5%(17) |
10.5%(2) |
|
|
||
|
High |
100%(27) |
0%(0) |
|
|
||
|
Absent |
50%(2) |
50%(2) |
|
|
||
|
Inflammation |
|
1+ |
2+ |
3+ |
|
0.29 |
|
Low |
42%(8) |
37%(7) |
21%(4) |
|
||
|
High |
67%(18) |
26%(7) |
7%(2) |
|
||
|
Absent |
75%(3) |
(0) |
25%(1) |
|
||
|
Estrogen receptor |
|
Low |
High |
Absent |
|
0.32 |
|
ER + |
37%(13) |
57%(20) |
6%(2) |
|
||
|
ER- |
40%(6) |
47%(7) |
13%(2) |
|
||

Tumor budding was evaluated in all the 50 cases. 54%(27 cases) showing high grade tumor budding, 38%(19 cases) with low grade tumor budding and 8%(4) cases with absent tumor budding were observed.
63% cases with age ≥50 years showed high grade tumor budding compared to age <50 years (37%). Significant association with p value = 0.01 is observed between tumor size and tumor budding. 18 cases of grade 2 (66.7%) showed high grade tumor budding and 4 cases of grade 3 showed low grade tumor budding (21.1%).
74% cases showed high grade tumor budding along with absence of necrosis and low grade tumor budding is seen in 26% cases.
Significant association with p-value 0.03 was observed between tumour budding and lymphovascular invasion. Equal distribution of cases showing presence and absence of lymph node metastasis noted. No significant association is observed.
High grade tumor budding showed strong association (p-value of 0.0001) with clinical TNM staging. High grade was observed maximum in stage 2 (65.2%). High grade tumor budding showed strong association (p-value of 0.002) in patients with primary breast carcinoma (100%) compared to those who underwent post neo-adjuvant chemotherapy (0%).

67% of cases with mild inflammation (1+) showed high grade tumor budding whereas 21% with severe inflammation showed low grade tumor budding.

High grade tumor budding was seen maximum in 20 ER positive cases. No significant association is seen with PR and Her2neu receptor status.

No significant association is seen between tumor budding and laterality.
Tumor budding is one of the mechanisms of cancer invasion and metastasis.Tumor budding was first described by Imai in stomach cancer 5. It has been studied in detail in colorectal cancer and is included in the guidelines for management of colorectal cancer.
In view of very few studies, this study is done to evaluate significance of tumor budding in breast carcinoma and its association with the clinicopathological parameters and hormone receptors.
|
Parameter |
Index Study |
Archana et al. 1 |
Kumarguru et al. 8 |
Gujam et al. 16 |
Sriwidyani et al. 14 |
|
Age |
⩾ 50yrs |
>40 yrs |
6th decade |
>50 yrs |
5thdecade |
|
Laterality |
Right |
Left |
Left |
---- |
---- |
|
Objective lens |
40 x |
40x |
40x |
20x |
40x |
|
Count of tumour buds |
≥10 |
≥10 |
≥20 |
≥20 |
≥10 |
|
Lesion |
Invasive breast carcinoma |
Invasive breast carcinoma |
Invasive breast carcinoma |
Invasive breast carcinoma NOS |
Invasive breast carcinoma NOS |
|
Number of fields |
10 |
10 |
10 |
5 |
5 |
|
Staining |
H & E |
H & E |
H & E |
H & E |
IHC |
|
Prognostic factor |
Index Study |
Archana et al. 1 |
Kumarguru et al. 8 |
Sriwidyani et al. 14 |
Gujam et al. 16 |
Salhia et al. |
|
Size |
T2 (p=0.02) |
T2 |
--- |
(p=0.03) |
T1 |
T1 |
|
Grade |
(G2) NS (p=0.11) |
G2 |
NS (p=0.884) |
S (p=0.031 ) |
NS (p=0.09) |
(G2) S (p=0.036) |
|
LVI |
S (p = 0.03) |
NS (p <0.559) |
S (p < 0.001) |
S (p < 0.003) |
S (p=0.001) |
S (p=0.015) |
|
Lymph node Metastases |
NS (p = 0.12) |
NS (p=0.434 ) |
S (p < 0.001) |
S (p < 0.001) |
NS (p=0.081) |
S (p=0.003) |
|
Necrosis |
Absent 32(74.42%) |
Absent 52 (79%) |
Present 40(80%) |
---- |
High 248 (52%) |
---- |
|
Treatment status |
S (p=0.001 ) |
---- |
---- |
---- |
NS (p=0.096) |
---- |
|
TNM Staging |
S (p=0.001) |
---- |
S ( p =0.024) |
S(p<0.001) |
---- |
--- |
|
ER |
NS (p= 0.32) |
NS (p= 0.729) |
---- |
NS (p=0.334) |
S (p= 0.003) |
S (p= 0.02) |
|
Inflammation |
NS (p= 0.29) |
S (p= 0.016) |
---- |
--- |
S (p=0.002) |
----- |
65% of the cases were of size T2. There was significant association (p=0.02) observed between tumor size and high grade tumor budding which is in line with the studies conducted by Archana et al 5, Agrawal R et al 11, Gabal et al 13, Sriwidyani et al 14. Sahlia et al15 and Gujam et al16 in their study had tumor size of ≤ 20mm.
54% of the cases had tumor of grade 2 similar to studies conducted by Archana et al 5, Masilamani et al 9 and Gabal et al13 and in contrast to Sriwidyani et al14 and Sahlia et al 15, no significant association was observed.
76% cases showed presence of lymphovascular invasion. Significant association(p = 0.03) is observed in most of the studies. The index study results were in disagreement with Archana et al5 and Masilamani et al 9.
Similar to studies conducted by Archana et al 5, Agrawal R et al11 and Gujam et al 16, lymph node metastasis was seen to be equally present and it is absent in present study.
In the study, necrosis was absent in 74% cases. Similar results were observed by Archana et al 5, Gabal et al13 and Gujam et al16 noticed 52% of the cases with high tumor necrosis.
Very few studies were done on treatment status in tumor budding. In contrast to Gujam et al 16, strong association (p=0.001) was observed between treatment status and high grade tumor budding.
Strong association (p=0.001) was noted with TNM staging and the results are in agreement with Kumarguru et al8 and Sriwidyani et al 14.
Present study shows molecular subtyping with no significant association between the hormone receptors and tumor budding. However, significant association between tumor budding and ER positive tumors was found in Rathod et al3 and Sahlia et al 15.
Few studies showed significant association with inflammation whereas the index study showed no similar result.
The limitation of the study primarily is smaller sample size. Since the study was done in a tertiary care center, immunohistochemical markers like Ki-67, CD 34, D2 40 were unavailable.
The following variables have a significant association with the tumor budding in the index study: Tumor size, TNM staging, treatment status, lymphovascular invasion and ER positive tumors.
Tumor budding may be of great help to the clinicians to assess the prognosis of the patient, especially its association with lymphovascular invasion in the absence of lymph node metastases. Tumor budding may be incorporated as a new parameter in the reporting CAP protocols for reporting breast cancer cases.
Subscribe now for latest articles and news.