Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.26.23
Year: 2026, Volume: 12, Issue: 2, Pages: 219-222
Case Report
Jyoti Rajpoot 1, Tathagata Chatterjee 2, Dipti Sidam 3, Mukta Pujani 2, Sanjay Rai 4
1Assistant Professor, Department of Pathology, ESIC Medical College, Faridabad, Haryana, India.
2Professor, Department of Pathology, ESIC Medical College, Faridabad, Haryana, India.
3Associate Professor, Department of Pathology, ESIC Medical College, Faridabad, Haryana, India.
4Associate Professor, Department of Oncology, ESIC Medical College, Faridabad, Haryana, India.
Address for correspondence: Dipti Sidam, Associate Professor, Department of Pathology, ESIC Medical College, Faridabad, Haryana, India.
E-mail: [email protected]
Received Date:22 January 2026, Accepted Date:03 May 2026, Published Date:15 June 2026
Acute lymphoblastic leukaemia is the most common childhood malignancy, followed by acute myeloid leukaemia (AML). AML with t(3;5) is a rare entity categorised under the WHO classification of AML with myelodysplasia-related changes. We present a case of an 8-year-old male child who presented with complaints of intermittent fever and generalised weakness. Complete blood count (CBC) revealed bicytopenia with 8% blasts. Flow cytometry performed on a bone marrow sample confirmed AML with monocytic differentiation. Chromosomal analysis revealed the presence of t(3;5). Remission was not achieved after the first induction chemotherapy.
In children, the most common haematological malignancy is acute lymphoblastic leukaemia (ALL), accounting for approximately 80% of cases, while the remaining 20% are acute myeloid leukaemia (AML)[1]. The reported incidence of pediatric AML is 7 cases per million children under the age of 15[2]. AML with the translocation t(3;5) has been classified as AML with myelodysplasia-related changes in the recent WHO classification[3]. This balanced translocation is rare, with an incidence of less than 0.5% among AML cases[4]. Here, we present a rare case of AML with t(3;5) in a child.
An 8-year-old male child presented with complaints of intermittent fever and generalized weakness for the past 3 months. On general examination, pallor was present. No clubbing, icterus, or cyanosis was noted, and no organomegaly was present. Basic investigations were advised, including CBC with peripheral smear, LFT, KFT, iron studies, serum vitamin B12, serum folate, serum LDH, serum electrolytes, and viral markers.
On CBC, hemoglobin was 4.10 g/dL, total leukocyte count was 9,030/μL, and platelet count was 67,000/mm³. Peripheral smear examination showed predominantly normocytic normochromic RBCs, with occasional microcytes and pencil cells. Schistocytes were present in <1%. The total leukocyte count was normal (9,000/μL), but 8% blasts were noted on the differential leukocyte count. Platelets were low at 70,000/mm³. LFT, KFT, and serum electrolytes were normal. In iron studies, serum iron (205 μg/dL) and ferritin (552 ng/mL) were raised. Serum vitamin B12 (6897 pg/mL) and LDH (477.1 U/L) levels were elevated. The serum folate level (14.7 ng/mL) was adequate. Viral markers for HBsAg, HCV, HIV, EBV, Parvo B-19, and CMV were negative. Considering the low hemoglobin, blood transfusions were administered [Table. 1].
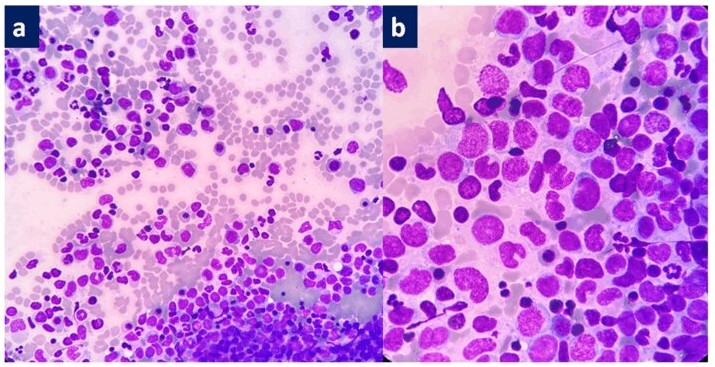
Given the bicytopenia and 8% blasts on CBC, bone marrow aspirate (BMA) and biopsy were advised. BMA smears ([Fig. 1]a, b) were cellular, showing predominantly blast cells, which were 2.5-3 times the size of small lymphocytes, with moderate amounts of cytoplasm, opened-up chromatin, and inconspicuous nucleoli. A few blast cells showed Auer rods. Myeloid lineage was seen in various stages of maturation. Singly dispersed megakaryocytes were noted, with a few showing hypolobation. The erythroid lineage showed megaloblastic maturation, with some cells showing nuclear budding and irregular nuclear outlines.
| S. No | Test | Result | Reference range |
|---|---|---|---|
| 1 | Hemoglobin (Hb) | 4.10 (Severely low) | 12–16 (female) / 13–17 (male) g/dL |
| 2 | Total Leukocyte Count (TLC) | 9,030 (Normal) | 4,000–11,000/μL |
| 3 | Platelet Count | 67,000 / 70,000 (Thrombocytopenia) | 150,000–450,000/mm³ |
| 4 | Serum Iron | 205 (Raised) | 60–170 μg/dL |
| 5 | Serum Ferritin | 552 (Elevated) | 15–150 (female) / 30–400 (male) ng/mL |
| 6 | Vitamin B12 | 6897 (Markedly elevated) | 200–900 pg/mL |
| 7 | Serum Folate | 14.7 (Adequate) | >3 ng/mL |
| 8 | LDH | 477.1 (Elevated) | 140–280 U/L |
| 9 | Liver Function Tests (LFT) | Normal | - |
| 10 | Kidney Function Tests (KFT) | Normal | - |
| 11 | Serum Electrolytes | Normal | - |
| 12 | Viral Markers (HBsAg, HCV, HIV, EBV, Parvo B-19, CMV) | Negative (No active infection) | - |
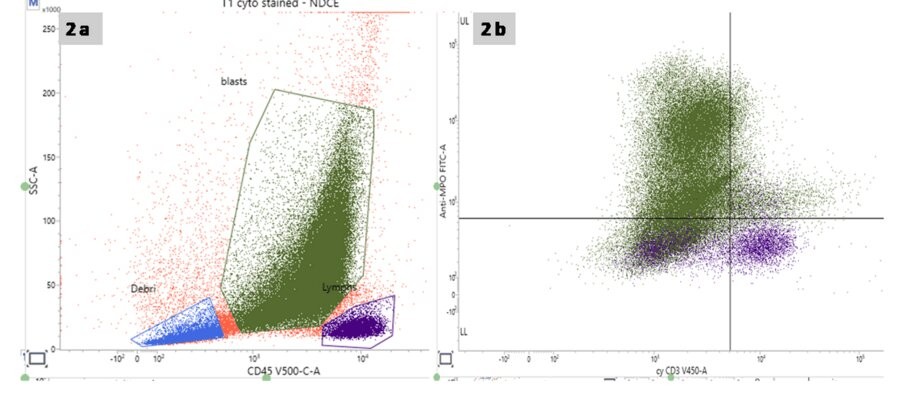
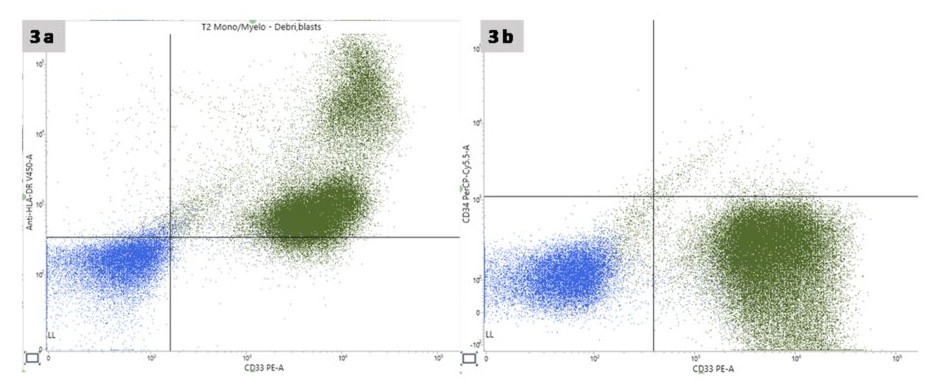
Flow cytometry performed on a bone marrow sample showed 60% blasts with moderate CD45 positivity and moderate side scatter ([Fig. 2]a). These cells were positive for cMPO (bright to moderate) ([Fig. 2]b), HLA-DR (moderate) ([Fig. 3]a), CD10 (bright to moderate), CD13 (bright 43.75% and dim to negative 35.23%), CD33 ([Fig. 3]b), CD64 (bright 11%), CD11c (bright 11%, moderate 39%, dim to negative 42%), and CD56 (bright).
Based on morphology and immunophenotyping, a diagnosis of acute myeloid leukemia with monocytic differentiation was made. Cytogenetics and molecular studies were advised for risk stratification.
Chromosomal analysis revealed a reciprocal translocation between the long arms of chromosomes 3 (region q25) and 5 (region q34): t(3;5)(q25;q34). Chemotherapy was initiated. After the induction therapy, which included cytarabine, daunorubicin, voriconazole, and dexamethasone, repeated bone marrow aspiration and biopsy were performed. These showed 22% blasts. Another round of chemotherapy with the same drugs was administered. Following this, a repeat bone marrow aspiration and biopsy showed morphological remission. At the time of writing this case report, the patient was undergoing the consolidation phase of chemotherapy.
Childhood acute myeloid leukemia (AML) is relatively rare and associated with significant mortality. Major host factors such as age, race, weight, and germline predisposition influence the outcome of AML in children. Important clinical characteristics associated with a poorer prognosis include a high white blood cell (WBC) count (above 100,000/μl) at the time of presentation, cerebrospinal fluid (CSF) involvement, and cutaneous manifestations[5]. Ruling out central nervous system (CNS) involvement is crucial, as its presence alters management strategies.
The cytogenetic and molecular alterations seen in pediatric AML differ from those in adults. Favourable, low risk cytogenetic alterations include Nucleophosmin 1 (NPM1), core-binding factor mutations, CEBPA gene mutations, t(8;21)(q22;q22) RUNX1-RUNX1T1, and inv(16)(p13q22) CBFB-MYH11. Alterations associated with poor prognosis include t(6;9)(p23;q34) DEK-NUP214, t(7;12)(q36;p13) MNX1-ETV6, and t(5;11)(q35;p15) NUP98-NSD1[6]. AML with t(3;5) has been reported to carry a poor prognosis in a study by Grimwade et al.[7]., while Dumézy et al. reassessed the same and found this translocation to be consistent with an intermediate prognosis[8].
In our case, the patient did not respond to the first cycle of induction chemotherapy and required a second cycle to achieve remission. At the time of this case report, the patient’s symptoms had not improved satisfactorily.
AML with t(3;5) is categorized as ‘AML with myelodysplasia-related changes. In our case, dysplasia was observed in both the megakaryocytic and erythroid lineages. The t(3;5) translocation is a rare clonal abnormality in acute leukemia, involving a balanced translocation between the long arms of chromosomes 3 and 5. It was first described in 1996 by Yoneda-Kato et al., who reported the NPM1/MLF1 gene rearrangement in AML/MDS patients with t(3;5)(q25.1; q34)[9].
Lim et al., in their study, described the clinical and laboratory features associated with t(3;5). They observed a male predominance, with a mean age of 34.5 years[4]. Our patient is an 8-year-old male child. In their cohort of 54 patients, full karyotyping was performed on all, and t(3;5) was the most common sole chromosomal anomaly, present in 31 patients. Trisomy 8 was noted in five cases. Similarly, in our case, t(3;5)(q25;q34) was the sole chromosomal abnormality identified.
In Lim et al.’s study, 66% of patients were diagnosed with de novo AML, including AML subtypes M2, M4, and M6. Our patient also presented with de novo AML, classified as the M4 subtype.
In a separate study of seven AML patients with t(3;5) by Dumézy et al.[8], flow cytometric analysis revealed that blasts were positive for CD117, CD13, and CD33, while CD34 was negative in 86% (six) of cases. In contrast, our patient’s blasts showed positivity for HLA-DR, CD13, CD33, and CD34, but were negative for CD117. AML PCR panel testing did not detect any of the following mutations or gene rearrangements: NPM1 (Type A, B), FLT3, C-KIT, PML-RARA, AML1-ETO, CBFB-MYH11, or BCR-ABL1.
Cytogenetic and molecular alterations in pediatric acute myeloid leukemia (AML) differ substantially from those seen in adults, both in terms of frequency and prognostic implications. Among these, AML with t(3;5)(q25; q35) is an exceptionally uncommon cytogenetic anomaly in the pediatric age group, with few instances documented in the literature. In our case, the presence of this translocation, along with severe anemia, thrombocytopenia, and the presence of blasts on peripheral smear, raises concern for an underlying high-risk disease subtype. Although t(3;5) has been variably correlated with poor prognosis in adult patients, its impact in pediatric populations remains unclear. This translocation's rarity limited pediatric patients' access to approved therapy recommendations and risk stratification systems.
This case emphasizes the critical role of cytogenetic and molecular testing in pediatric AML. Owing to the scarcity of data on t(3;5) in children, larger cohort studies are essential to elucidate its clinical characteristics, response to therapy, and long-term outcomes.
1. Pediatric AML: From Biology to Clinical Management. Journal of Clinical Medicine. 2015; 4 (1). Available from: https://doi.org/10.3390/jcm4010127
2. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. 2012; 120 (16). Available from: https://doi.org/10.1182/blood-2012-03-362608
3. Diagnosis and Treatment of Patients With Acute Myeloid Leukemia With Myelodysplasia-Related Changes (AML-MRC). American Journal of Clinical Pathology. 2020; 154 (6). Available from: https://doi.org/10.1093/ajcp/aqaa107
4. Detection of t(3;5) and NPM1/MLF1 rearrangement in an elderly patient with acute myeloid leukemia: clinical and laboratory study with review of the literature. Cancer Genetics and Cytogenetics. 2010; 199 (2). Available from: https://doi.org/10.1016/j.cancergencyto.2010.02.009
5. Pediatric acute myeloid leukemia: updates on biology, risk stratification, and therapy. Current Opinion in Pediatrics. 2020; 32 (1). Available from: https://doi.org/10.1097/mop.0000000000000855
6. The molecular landscape of pediatric acute myeloid leukemia reveals recurrent structural alterations and age-specific mutational interactions. Nature Medicine. 2018; 24 (1). Available from: https://doi.org/10.1038/nm.4439
7. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010; 116 (3). Available from: https://doi.org/10.1182/blood-2009-11-254441
8. Acute myeloid leukemia with translocation t(3;5): new molecular insights. Haematologica. 2013; 98 (4). Available from: https://doi.org/10.3324/haematol.2012.082149
9. Yoneda-Kato N, Look AT, Kirstein MN, Valentine MB, Raimondi SC, Cohen KJ, et al. The t(3;5)(q25.1;q34) of myelodysplastic syndrome and acute myeloid leukemia produces a novel fusion gene, NPM-MLF1. Oncogene. 1996;12: 265-275.
Subscribe now for latest articles and news.