Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.015
Year: 2021, Volume: 7, Issue: 2, Pages: 90-95
Original Article
N. Hemavathi1 , H. Sridhar2
1 Assistant Professor, Department of Pathology, MVJ Medical College and Research Hospital, Hoskote, Bengaluru, Karnataka, India,
2 Associate Professor, Department of Pathology, M S Ramaiah Medical College, Bengaluru, Karnataka, India
Address for correspondence:
Dr. N. Hemavathi, No. 2, 7th Cross, Kubersingh Lane, Dodda Mavalli, Lalbagh Road, Bengaluru, Karnataka, India. E-mail: [email protected]
Background: Neoadjuvant chemotherapy (NACT) administered preoperatively is currently the standard treatment modality being used for locally advanced breast cancers, primarily meant for clinical downstaging. Histopathological assessment of the tumor response is a gold standard and is essential for the identification of a group of patients with pathological complete response (pCR) or pathological non-complete response (pNR).
Aim: The aim of the study was as follows: (1) To study the histopathological changes induced with NACT in breast carcinoma and (2) to evaluate the pathological response to treatment.
Materials and Methods: Thirty cases of modified radical mastectomy have been studied in locally advanced breast carcinomas with NACT. Statistical Analysis: Frequency tables and Pearson Chi-square were utilized for this study.
Results: The cytomorphological changes of the tumor cellularity and stromal changes were documented. The most common findings were cytoplasmic eosinophilia (70%) and stromal dense fibrosis (83%). Out of 30 cases, 27 cases (90%) achieved pathological partial response with 1 case (3.3%) of Stage 0 achieved pCR and the remaining 2 cases (6.7%) of Stage II showed pathological no response as per the Miller Payne and Pinder et al. tumor regression grading system. Lymphatic metastasis was seen in 73% of cases, of which 50% showed chemotherapeutic response as noted in Pinder et al. Conclusion: Pathological evaluation of the response to NACT is the most essential component, providing important prognostic information that also helps to predict distant relapse-free survival.
KEY WORDS: Breast carcinoma, neoadjuvant chemotherapy, post-chemotherapy changes, tumor regression grading, pathological response
The cancer that spreads locally to large portions of the breast tissue along with or without involvement of the adjacent locoregional lymph nodes, without metastasizing to the distant sites refers to the term locally advanced breast cancer (LABC).[1] In the United States, it accounts to 5–15% only. However, in developing nations, this constitutes up to 60% of the newly diagnosed cases.[2] They may be treated with endocrine therapy or chemotherapy before the surgical excision termed neoadjuvant therapy.[1] Preoperatively, administered neoadjuvant chemotherapy (NACT) currently represents the standard treatment option for LABC.[3] It renders major benefits by allowing surgery in primarily inoperable ones, helping in downstaging the resectable tumors, thereby promoting breast conservative surgery, gives prognostic details, and enables the therapy to be modified or changed in cases of non-responsive tumors and sets an ideal research tool in the study of biomarkers.[4] Pathological evaluation of therapeutic response of the residual tumor in the breast and lymph node is critical as it helps to determine the prognosis, survival, and provide guidance for further therapy to be used after the surgery.[5] Therefore, it is still considered to be the gold standard for determining the pathologic complete response (pCR) or pathologic non-complete response (pNR) to the therapy.[2]
With the achievement of pCR, it can also serve as an important predictive marker for disease-free survival and overall survival.[6]
As the surgical pathologists are increasingly encountering post-chemotherapy treated breast carcinoma cases, it is essential for the proper assessment of histopathological response to the therapy and thereby predicting the prognosis of the patients. Hence, in this study, we try to analyze the cytomorphological changes of the tumor cellularity and stromal changes induced by the therapy and also to assess the pathological response.
The aim of the study was as follows:
1. To study the histopathological changes induced with NACT in breast carcinoma
2. To evaluate the pathological response to treatment.
This was both retrospective and prospective studies done from January 2015 to July 2017 on 30 modified radical mastectomy cases of locally advanced breast carcinomas (LABCs) who received NACT in the Department of Pathology, Ramaiah Medical College. The patients with biopsy-proven breast carcinoma and who had undergone with two or more cycles of NACT were included in the study. Other cases with a single cycle of chemotherapy or without a biopsy proven before the surgery were excluded from the study. All mastectomy specimens were received in 10% formalin. The standard protocol for surgical grossing of resected specimens was undertaken. Then, paraffin sections of 5 µm were cut and stained with hematoxylin and eosin. The stained slides were studied for therapy-induced changes which cause shrinkage of the tumor cellularity and examining the histomorphological changes where the residual tumor cells show hypereosinophilia and vacuolation of the cytoplasm, variation in nuclear size and increased chromatin pattern, and stromal associated changes in the form of necrosis, fibrosis, elastosis, calcification, and infiltration by mononuclear cells and giant cells. Similarly, therapy-induced effects in the isolated lymph nodes will be analyzed.[7] The tumor was then graded according to Elston-Ellis modification of Scarff Bloom Richardson system which is considered to be the well-established prognostic factor. Two tumor regression grading systems of Miller Payne and Pinder et al. were used for evaluating and grading the pathologic response to chemotherapy as pathologic complete response (pCR), pathological partial response (pPR), and pathological no response (pNR).[8]
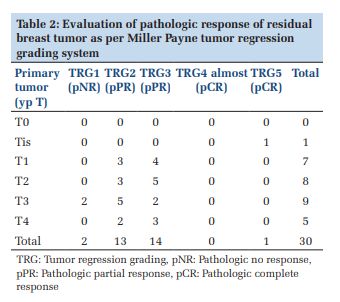
According to Miller Payne tumor regression grading system, Grade 1 indicates no complete cellular reduction (p NR), Grade 2 shows 30% loss of tumor cells (pPR), Grade 3 shows reduction in tumor cellularity by 30–90% (pPR, Grade 4 shows loss of tumor cellularity by >90% (almost pCR), and Grade 5 shows either absence of tumor cells or presence of ductal carcinoma in situ (DCIS) component.[8]
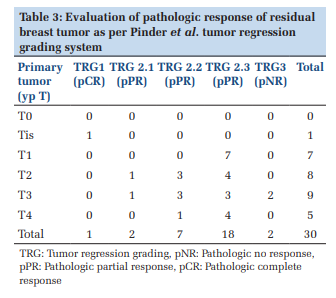
The pathologic response in both the breast and lymph nodes will be noted according to Pinder et al. tumor regression grading system. Hence, the pathologic tumor response in breast is categorized as pCR, pPR, and pNR. pCR shows no evidence of residual tumor along with or without presence of DCIS component. pPR is further subgraded into (1) showing minimal residual disease (<10% of tumor remaining), (2) evidence of response with 10–50% of tumor remaining, or (3) >50% of tumor cellularity remaining with evidence of response present. pNR indicates no response to therapy.[8]
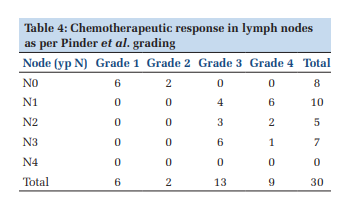
As per Pinder et al., chemotherapeutic response in the lymph nodes can be graded as Grade 1: No evidence of metastasis or response, Grade 2: Metastasis not present but evidence of response, Grade 3: Metastasis present with evidence of response, and Grade 4: Metastasis present with no evidence of response.[8]
Frequency tables and Pearson Chi-square were utilized for this study.
The age group of the patients in the present study ranges from 29 to 61 years, with a peak incidence in the 4th decade. All the cases are female breast cancers. Macroscopically, the size of the tumor bed ranges from 1.5 cm to 16 cm in maximum dimension. The most common histopathological type was found to be infiltrating ductal carcinoma, NOS seen in 90% of cases (27/30). Ductal carcinoma in situ of high-grade type without invasive carcinoma or microinvasion was seen in 1 case (3.3%). Mucinous carcinoma and medullary carcinoma were seen in the remaining cases each accounting for 3.3% of cases. DCIS was found as an additional finding in 33.3% of the cases of invasive breast carcinoma.
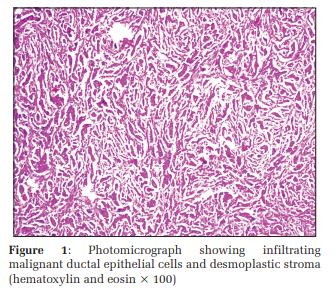
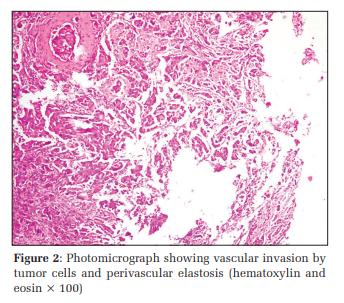
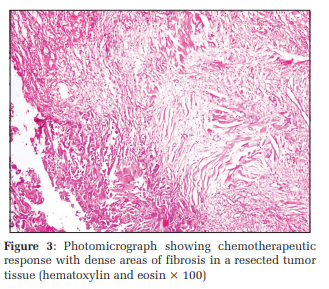
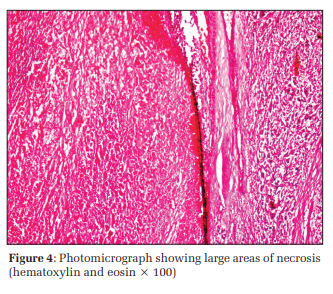
In this study, cytoplasmic eosinophilia (70%) and stromal dense fibrosis (83%) were the common findings to be noted. Other findings such as desmoplastic stroma infiltrated mainly by lymphocytes were seen in 63% of cases, followed by necrosis (60%), foci of micro calcification (20%), and perivascular elastosis as well as giant cell reaction was found in 6.6% of cases [Figures 1-4].
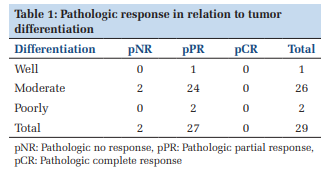
The invasive tumor component was then graded according to Elston-Ellis modification of Scarff Bloom Richardson system, where moderately differentiated ductal carcinomas were seen in maximum number of cases (90%), of which 92.3% of these cases had pathologic partial response (pPR) and the remaining 7.7% of cases showed pathologic no response (pNR) [Table 1].
According to the Miller Payne and Pinder et al. tumor regression grading system, one case of DCIS showed pCR. Among the majority of cases with a residual tumor >5 cm, 78% of cases showed pPR and 22.2% had no response (pNR) [Tables 2 and 3].
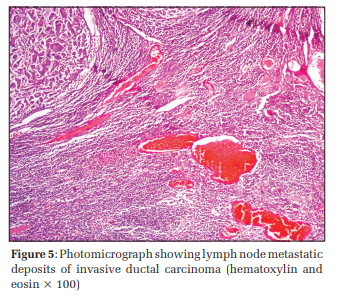
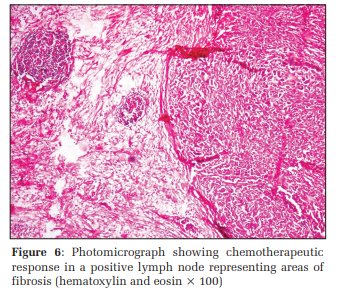
Lymphatic metastasis was seen in 73% of cases, of which 50% showed chemotherapeutic response as noted in Pinder et al [Table 4 and Figures 5 and 6]. Stromal dense fibrosis was found to be significantly correlated to pathologic response and tumor regression grade (P < 0.05).
Vascular invasion was seen in 50% of cases and perineural invasion was seen in 36.6% of cases.
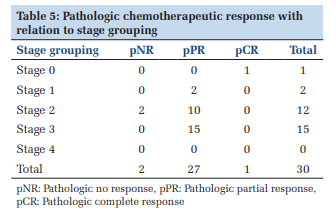
Out of 30 cases, 27 (90%) achieved pPR with majority belonged to Stage III, 1 case (3.3%) of Stage 0 achieved pCR, and the remaining 2 cases (6.7%) of Stage II showed no response (pNR) as per the Miller Payne and Pinder et al. tumor regression grading system [Table 5].
Breast cancer is the world’s most frequent malignancy among females. For medical and surgical oncologists in developing countries, LABC remains a frequent encounter and challenge.[2]
Few authors have not seen any change in the histologic tumor type following chemotherapy, nor have we observed the change of tumor type.[9-11]
Markis et al.,[12] in their study, showed drastic decrease in tumor burden that 10% of cases had no evidence of residual tumor cells while we had only 3.3% of cases showing similar response to therapy with feature of DCIS component alone being present.
In our study, the percentage of partial response was found to be highest which accounted to 90%. In a similar study conducted by Kumari et al.,[3] partial response was reported in 40% of cases, no response in 40%, and a complete response in 20% of cases.
Thus, the histopathological evaluation of therapeutic response is the gold standard with tumor regression grading system being considered to be an independent predictor of survival in post-NACT breast carcinoma because patients with partial/complete pathological tumor regression can show improved disease-free and overall survival with low risk of recurrence and better chance of being free from distant metastasis.
NACT can apparently induce significant histomorphologic changes in breast cancer and therefore, urge the need for an accurate pathological response evaluation of resected tumor and regional lymph nodes by incorporating tumor regression grading systems. Evaluation of pathologic response to therapy may provide important prognostic information to patients and help direct the extent of surgery or subsequent systemic and/or radiation therapy. Pathological assessment of residual disease is, therefore, a key component of the post-NACT breast cancer assessment. Hence, the pathological assessment of therapeutic response helps in predicting the distant relapse-free survival and also helps in modification of the treatment.
Subscribe now for latest articles and news.