Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.134
Year: 2025, Volume: 11, Issue: 1, Pages: 98-100
Case Series
Vijayashree Raghavan1 , Ayeesha Sithika Thajudeen2 , Kundhavai Chandrasekaran3
1Professor & HOD, Department of Pathology, Chettinad Hospital and Research Institute, Kelambakkam, Chengalpattu, Tamil Nadu, India,
2Associate Professor, Department of Pathology, Chettinad Hospital and Research Institute, Kelambakkam, Chengalpattu, Tamil Nadu, India,
3Assistant Professor, Department of Pathology, Chettinad Hospital and Research Institute, Kelambakkam, Chengalpattu, Tamil Nadu, India
Address for correspondence:
Ayeesha Sithika Thajudeen, Associate Professor, Department of Pathology, Chettinad Hospital and Research Institute, Kelambakkam, Chengalpattu, Tamil Nadu, India.
E-mail: [email protected]
Received Date:18 April 2024, Accepted Date:07 January 2024, Published Date:13 March 2025
Acquired reactive perforating collagenosis (ARPC) is a rare skin disorder occurring more common in patients with chronic kidney disease or diabetes. It is caused by the perforation of dermal connective tissue through the epidermis. We report four cases of acquired reactive perforating collagenosis in patients with chronic diabetes, confirmed by histopathology.
Keywords: Perforating collagenosis, Diabetes, Kidney disease
The perforating disorders comprise a group of disorders sharing the common characteristic of trans epidermal elimination (TEE). This phenomenon is characterized by altered collagen extruding through the epidermis. 1 They are two forms, acquired and inherited. Acquired reactive perforating collagenosis (ARPC) is a rare skin disorder occurring more common in patients with chronic kidney disease or diabetes. 2 It is caused by the perforation of dermal connective tissue through the epidermis.
Case 1: A 53-year-old male came with complaints of hyperpigmented follicular papules with central crater over the arms and legs for 3 months [Figure 1 a]. Known case of Diabetes mellitus for 19 years.
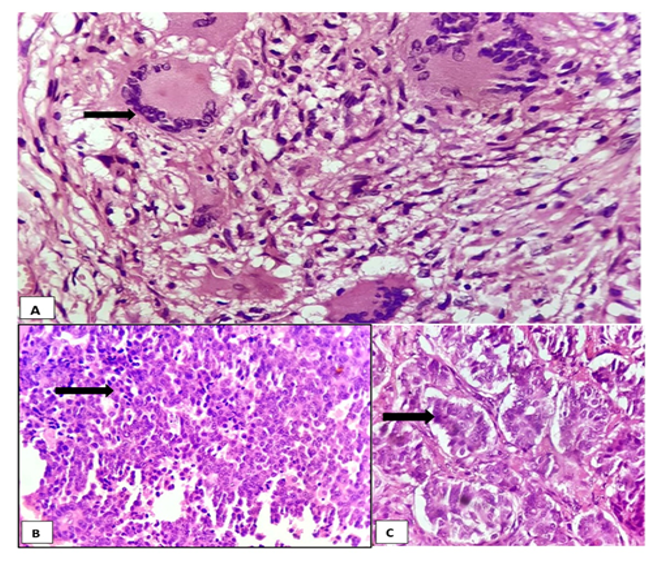
Sections from the skin showed hyperkeratosis, irregular acanthosis with crater like depression, basophilic material with altered collagen fibres in the crater exhibiting trans epidermal elimination [Figure 1 b]. The underlying papillary dermis shows moderate lymphocytic infiltrate.

Case 2: A 71-year-old male with complaints of multiple itchy hyperpigmented follicular papules with central crater over upper limbs, lower limbs and back [Figure 2 a]. He is a known diabetic.
Sections from the skin showed vertically oriented shallow invaginating epidermal channel with basophilic necrotic and degenerated collagen material. Rest of the epidermis show acanthosis, spongiosis and mild exocytosis. Moderate perivascular lymphocytic infiltrate in the papillary dermis [Figure 2 b].

Case 3: A 62-year-old female came with complaints of multiple skin lesions for 4 months [Figure 3 a].
Sections from the skin showed hyperplastic epithelium with focal ulceration and an adjacent invagination lined by stratified squamous epithelium, containing dense basophilic plug of keratin, altered collagen bundles and inflammatory debris. Underlying dermis showed moderate chronic inflammatory infiltrate. Masson’s Trichrome stain highlighted collagen fibres in the lesion [Figure 3 b].

Case 4: A 61-year-old female came with complaints of pigmented keratotic papule in the right thigh. She is a known case of diabetes for 8 years.
Sections from the skin showed a crater filled with keratin, collagen fibres and neutrophilic exudate. The stratum corneum shows entrapped plasma, the epidermis shows transient acantholysis with neutrophilic micro abscess. The superficial dermis shows proliferating capillaries with chronic inflammatory infiltrate composed of lymphocytes and plasma cells.
ARPC is a rare form of perforating dermatosis. Other forms include Kyrle disease, perforating folliculitis, and elastosis perforans serpiginosa.3 ARPC is diagnosed based on the visual or histological confirmation of trans epidermal elimination of degenerated fibres. The typical eruption has a central yellow-to-greenish crust, which represents degenerated dermal collagens. 4
Overexpression of transforming growth factor-3 has been shown around the cup shaped epidermal depression, which plays a crucial role in connective tissue metabolism and is involved in wound healing. TGF Beta, matrix metalloproteinase-1 and tissue inhibitor of metalloproteinase-1 immunoreactivity was significantly increased in the lesions which play an important role in regulation of epidermal homeostasis, delay in reepithelialisation and remodelling, and alterations in extracellular matrix protein metabolism. 5 The lesions are sometimes accompanied by severe pruritus and can impair the patient’s quality of life; therefore, clinicians should be aware of these characteristic eruptions in patients with diabetes or chronic kidney disease receiving haemodialysis for better management. 6
Subscribe now for latest articles and news.