Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i02.010
Year: 2015, Volume: 1, Issue: 2, Pages: 43-45
Case Report
Smitha Chandra1, Stanley John2, B Kiran3
1Assistant Professor, Department of Otorhinolaryngology, Shridevi Institute of Medical Sciences & Research Hospital, Tumkur, Karnataka, India,
2Professor, Department of Otorhinolaryngology, Shridevi Institute of Medical Sciences & Research Hospital, Tumkur, Karnataka, India,
3Associate Professor, Department of Otorhinolaryngology,
Shridevi Institute of Medical Sciences & Research Hospital, Tumkur, Karnataka, India
Address for correspondence:
Dr. Smitha Chandra, F8, Doctors Quarters, Government District Hospital, Tumkur, Karnataka, India. Phone: +91-9986700349.
E-mail: [email protected]
Myoepithelioma is rare benign tumors representing about the 1% of all the salivary gland tumors. The most common site of involvement is parotid gland, followed by palate in the oral cavity. These can arise either de novo or within a pre-existing pleomorphic adenoma. A female patient aged 46 years came to our OPD with swelling in the hard palate since 2 years. The patient had a history of similar swelling at the same location that was surgically removed 20 years ago. The patient was investigated, and the tumor was excised into to by intraoral approach. Histopathological examination of the specimen revealed a spindle cell myoepithelioma. In this report, we would stress on the clinical, radiological and histopathological features and the possible differential diagnosis of this rare tumor.
KEY WORDS: Myoepithelioma, hard palate, salivary gland, parotid
IntroductionMyoepithelial cells are seen in many secretory organs including salivary glands. They are ectodermal in origin and functions to squeeze the glandular secretion into the ductal system. They express ductal epithelium and smooth muscle phenotype.[1,2] Sheldon in 1943 was the first to identify myoepithelial tumors as a distinct salivary gland tumor entity.[3] Myoepitheliomas are rare benign neoplasm composed of myoepithelial cells. These tumors can occur in most of the glandular structures like salivary glands, breast and sweat glands of the skin.[4] Myoepithelioma of salivary glands occur mainly in parotid gland accounting to 50%, followed by sublingual and submandibular glands. Myoepitheliomas of minor salivary glands accounts to only 1.5% of all salivary gland tumors.[5] In the oral cavity, anterior part of the hard palate is devoid of salivary glands hence they occur in a posterolateral part of the hard palate and soft palate.[6] These tumors occur at a wide range of age with the average age being 44 years and more commonly seen in females. They present as asymptomatic slow growing mass over a period of few months to years.[4] Earlier these tumors were considered as a variant of pleomorphic adenoma, however now these were recognized as a histologically distinct entity by WHO in 1991.[7] Here we present this rare case of myoepithelioma arising from pleomorphic adenoma of the hard palate along with their imaging features, histological findings, management and differential diagnosis. |
||||||||||
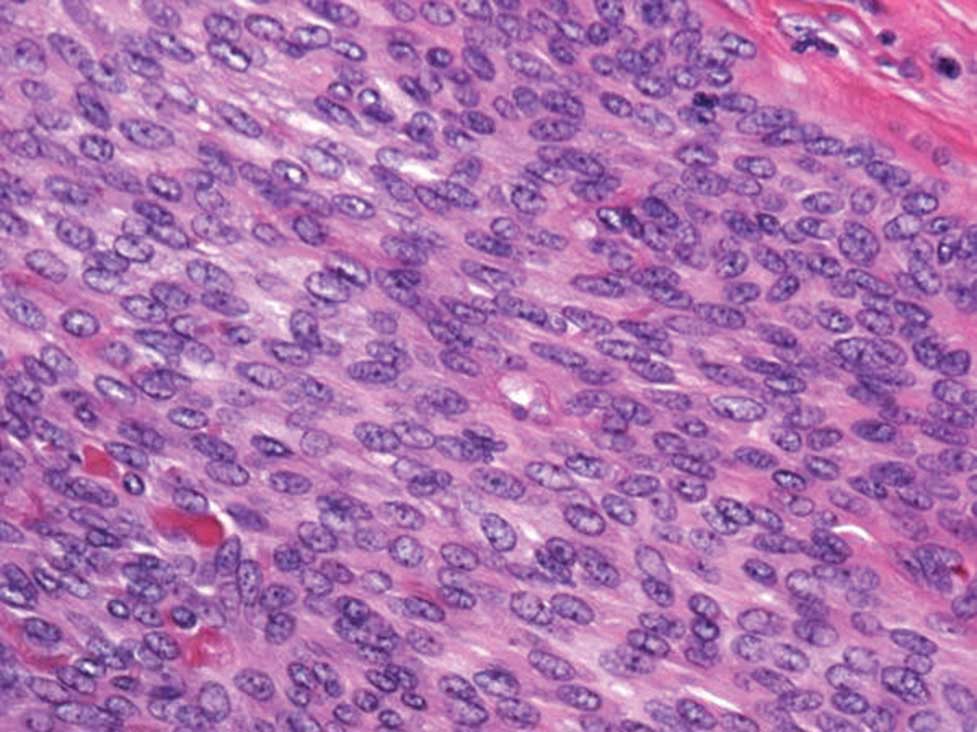
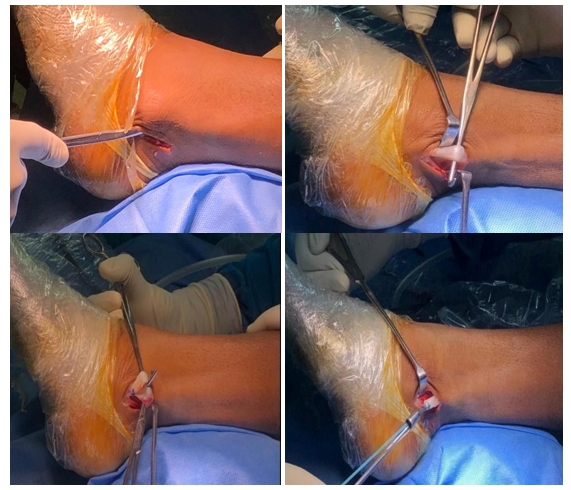
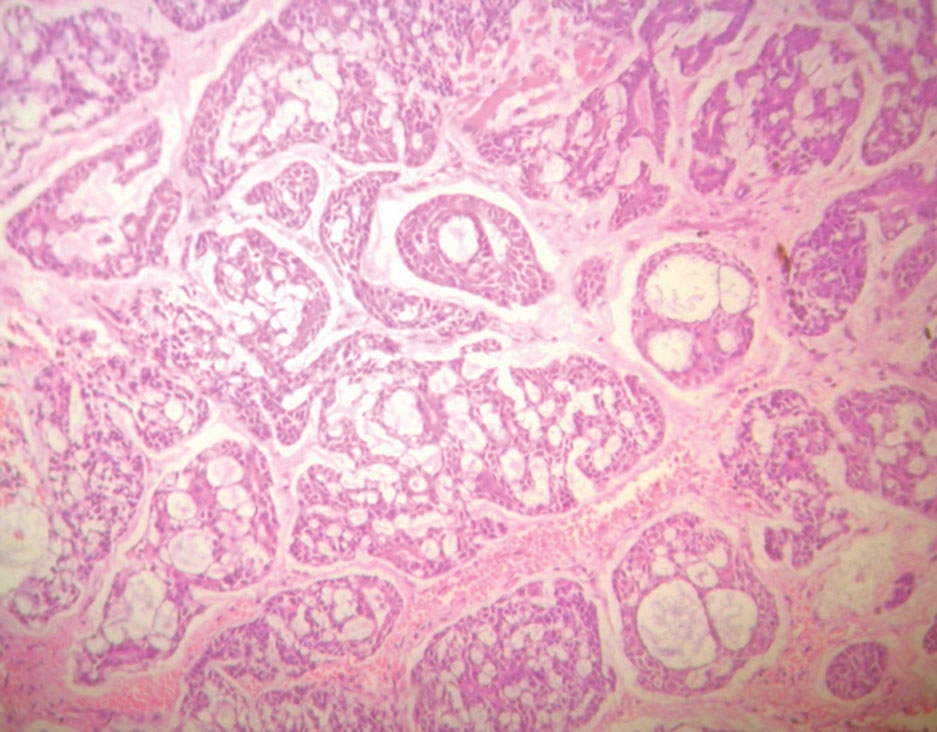
Case ReportA 46-year-old female patient presented with an asymptomatic slowly progressive palatal mass of two years duration (Figure 1). There was no history of dysphagia, odynophagia, voice change, weight loss, loss of appetite, bleeding from the lesion or fever. Patient had a history of similar mass in the palate 20 years ago which was excised and reported as pleomorphic adenoma. The clinical examination revealed a 2 cm × 2 cm, non-tender, non-pulsatile, firm, round, smooth surfaced pinkish mass in the right posterolateral part of the hard palate. There was no ulceration or erosion of overlying mucosa. There was no enlargement of regional lymph nodes. Contrast-enhanced computed tomography (CT) scan showed well-defined heterogeneous mildly enhancing soft tissue mass of 2.1 cm × 2.2 cm size in the hard palate with no evidence of erosion. There was no calcification, cystic component, or fat within the mass. With clinical and radiological features, we diagnosed it as a benign palatal tumor. After obtaining informed consent from the patient excisional biopsy of mass through intraoral approach, was done. The mucosal flap was raised; mass was excised submucosally with 0.5 cm margin around (Figure 2). The mucosa was closed with catgut sutures. Postoperative period was uneventful. The patient is being observed with regular follow-up. Gross examination revealed well circumscribed nodular, grayish solid mass with a smooth outline (Figure 3). The microscopy revealed predominant spindle cells over a nonepithelial hyaline-like basement membrane (Figure 4). The histopathological and immunohistochemical findings were suggestive of the benign myoepithelial tumor, myoepithelioma. Post operative period was uneventful with complete healing at the operative site. (Figure 5) Patient is being observed with regular follow up. |
||||||||||
|
||||||||||
DiscussionIn our case, the tumor was arising from the previously excised pleomorphic adenoma of the hard palate, which had occurred 20 years ago. The mass showed enhancement with no erosion in CT scan. Hence, we did wide excision of the tumor with 0.5 cm margin. The histopathogical and immunohistochemical findings confirmed our diagnosis of myoepithelioma. Myoepithelioma shows four different morphological patterns, which include nonmyxoid (solid), myxoid, reticular (canalicular) and mixed type.[8] The cellular patterns of myoepithelioma consists of plasmacytoid cells, spindle cells (most common), epitheloid cells, and clear cells (least common) patterns.[9] Myoepithelioma should be differentiated from its malignant counterpart, which is more aggressive and show recurrence even after adequate treatment. Ultrastructurally these tumors contain abundant cytoplasmic filaments/fibrils, the duplicity of basement membrane, perinuclear monofilament bundles, attachment plaques on the cell membrane and desmosome type intercellular junctions.[10] Myoepithelioma cells are positive for cytokeratins, vimentin and variable positivity for S100, calponin, smooth muscle actin, P63.[11] Myoepitheliomas show varying enhancement pattern on CT.[12] They are less prone for recurrence if they are removed completely. Most of these follow benign course whereas 7% eventually pursued a malignant course.[13] The rarity of myoepithelioma and the varied phenotypic expression of myoepithelioma cells may cause problems in diagnosis. Myoepithelioma needs to be differentiated from other tumors like pleomorphic adenoma, hemangiomas, neurinomas, lymphoma, solitary fibrous tumor, nerve sheath tumors, fibrous histiocytoma, paraganglioma, and leiomyoma. Differentiation from benign tumors is of academic interest, but careful differentiation has to be done from other malignant tumors like malignant myoepithelioma, mucoepidermoid carcinoma and spindle cell squamous carcinoma, leiomyosarcoma, hemangiopericytoma and metastatic tumor.[14,15] |
||||||||||
ConclusionMyoepitheliomas are rare benign tumors presenting as slow growing asymptomatic masses. With good history, clinical examination and radiological investigation it can be differentiated from the more common tumors like pleomorphic adenoma, adenoid cystic carcinoma. Histopathological and immunohistochemical examination of the tumor is mandatory for diagnosis. |
Subscribe now for latest articles and news.