Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i01.006
Year: 2017, Volume: 3, Issue: 1, Pages: 30-40
Original Article
Aniruna Dey1, Riti T K Sinha2
Introduction: The axilla, a triangular area located between the upper arm and thorax, contains blood vessels, nerves, lymph nodes, and fat. The most common palpable axillary masses are usually lymph nodes. However, axillary swellings can also arise from the various mesenchymal tissues present in the axillary area. Fine needle aspiration cytology (FNAC) is a relatively safe, quick, easy and a cheap diagnostic tool to decipher the benign or the malignant nature of the swelling. Although some studies have used ultrasonographic imaging techniques, alone others have used FNAC with or without ultrasound guidance to improve the detection of axillary masses. This study was conducted to document the spectrum of lesions encountered in a tertiary care center in FNAC of axillary lesions. Awareness of the various disease entities that can cause axillary masses help in their differential diagnoses.
Materials and Methods: A total of 75 cases of axillary swelling which were referred for FNAC to the Department of Pathology, were evaluated. All of these patients presented with superficial palpable swelling in the axilla. The clinical diagnoses were confirmed by cytology. FNACs were done and both air dried and alcohol-fixed smears were prepared and stained with May Grunwald Giemsa, hematoxylin and eosin, Zeihl Neelsen, and Papanicolaou stains. The adequacy of the diagnostic material and the results of FNAC were reported the same day.
Results: Out of the total of 75 cases of axillary swellings on which FNAC were done and evaluated, there were 24 males and 51 females. The clinical diagnoses were confirmed by cytology. Reactive lymphadenitis (30.6%) was the most common cytological diagnosis followed by lipoma (21.3%). In 42 cases (56%), the clinical diagnoses did not match with the cytological diagnoses. Most of the discrepancies were seen in the cases with the clinical diagnosis of tubercular lymphadenitis. Out of the 23 cases clinically suspected as tubercular lymphadenitis, only four cases showed the cytological findings consistent with tubercular lymphadenitis. The rest 19 cases showed findings consistent with reactive lymphadenitis (14 cases) and acute suppurative lymphadenitis (five cases). There were 18 cases with clinical suspicion of metastases from carcinoma breast to the axillary lymph nodes. Out of these, only nine cases showed cytopathological features of metastasis from carcinoma breast, whereas the remaining nine showed features of reactive lymphadenitis. Lipoma was clinically suspected in 24 cases out of which 16 cases had the cytological features of lipoma. Nine cases were clinically suspected as lymphadenopathy, out of which only three cases showed features of granulomatous lymphadenitis and rest of the cases had variable findings. There were few rare findings such as Schwannoma (two cases), pilomatricoma (one case), and fibroadenoma of ectopic breast (three cases). The diagnostic accuracy was 44% and sensitivity was found to be 44%. The low sensitivity was due to the discordance between the clinical and cytological diagnoses. Conclusion: Exploration of axillary swellings could result in unmasking of sinister findings and it can be said that all axillary lesions are not just lymph nodes. FNAC being a rapid and minimally invasive procedure can help as a diagnostic tool in such cases.
KEY WORDS:Axilla, fine needle aspiration cytology, granuloma, lipomatous lesion, lymphadenitis, lymph nodes, infiltrating duct carcinoma, Schwannoma, pilomatricoma.
The axilla is a triangular space between the lateral wall of thorax and the upper part of arm. Palpable lymph nodes and lymph node metastases from breast cancer are the most commonly encountered axillary masses. However, various mesenchymal tissues present in the axilla such as fat, vessels, and nerves can also give rise to different lesions.[1] Fine needle aspiration cytology (FNAC) is a safe, quick, easy, and a cheap diagnostic tool to decipher the benign or the malignant nature of the swelling. It involves random sampling of the cells using a needle, from the potentially pathological swelling. It is also a less invasive and less traumatic procedure, and better results are obtained in the hands of an experienced pathologist.[2,3] It is of utmost importance for the clinician to examine and palpate the axillary masses carefully and come to a diagnosis accordingly. However, just doing a physical examination of axillary mass lesions, without using other diagnostic modalities may lead to false negatives (patients with nonpalpable lymph nodes found to have tumor) and false positives (patients with hard lymph nodes found to have pathologies other than the tumor). Therefore, a cumulative approach using imaging techniques and FNAC is mandatory to reach a diagnosis. Furthermore, invasive procedures like sentinel node biopsies can be avoided. Various studies have shown that imaging techniques and FNAC, both used individually or coupled, improve the accuracy of diagnosis and help in avoiding unnecessary invasive procedures.[4,5] Various studies have been undertaken in the past to demonstrate various axillary lesions, some of which used only imaging techniques while others used FNAC.[1,4,6,7]
The aims and objectives of this study were as follows:
A total of 75 cases of axillary swelling which were referred for FNAC to the Department of Pathology, were evaluated. All of these patients presented with superficial palpable swelling in the axilla. Physical examination of all the palpable swellings was done by the pathologist performing the FNAC also. The clinical diagnoses were confirmed by cytology. FNACs were done using 20 or 22 gauge needles with or without the gun. Both air dried and alcohol-fixed smears were prepared. All the air dried smears were stained with May-Grunwald Giemsa stain, and the alcohol-fixed smears were stained with hematoxylin and eosin and Papanicolaou stains. Few of the smears were heat fixed and stained with Zeihl Neelsen (ZN) stain. The adequacy of the diagnostic material and the results of FNAC were reported the same day.
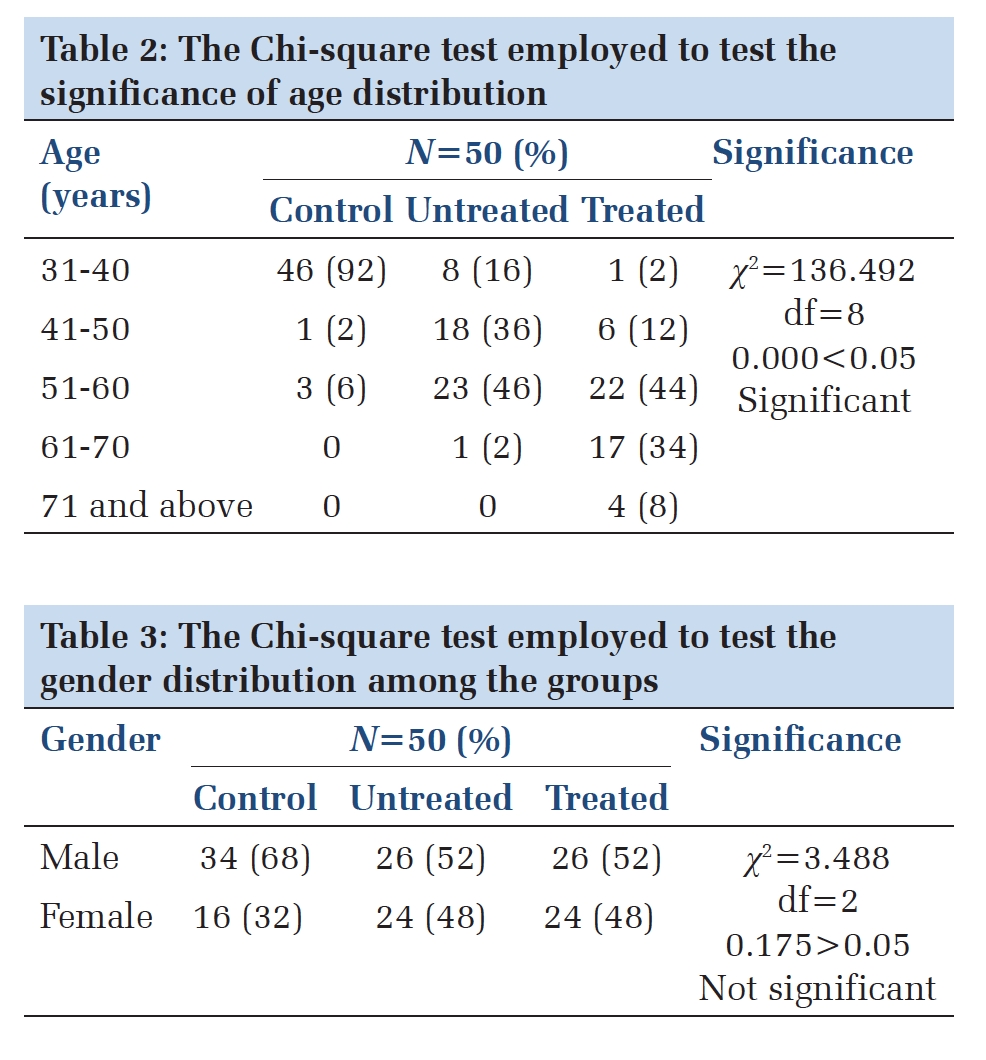
Out of the total 75 cases of axillary swellings on which FNAC were done and evaluated, there were 24 males and 51 females. The clinical diagnoses were confirmed by cytology. Reactive lymphadenitis (30.6%) was the most common cytological diagnosis followed by lipoma (21.3%) (Figure 1). In 42 cases (56%), the clinical diagnoses did not match with the cytological diagnoses (Table 1). Lipoma was clinically suspected in 24 cases out of which 16 cases had the cytological features of lipoma. Most of the discrepancies were seen in the cases with the clinical diagnosis of tubercular lymphadenitis. Out of the 23 cases clinically suspected as tubercular lymphadenitis, only four cases showed the cytological findings consistent with tubercular lymphadenitis. The rest 19 cases showed findings consistent with reactive lymphadenitis (14 cases) and acute suppurative lymphadenopathy (5 cases). There were 18 cases with clinical suspicion of metastases from carcinoma breast to the axillary lymph nodes. Out of these, only nine cases showed cytopathological features of metastasis from carcinoma breast, whereas the remaining nine showed features of reactive lymphadenitis. Nine cases were clinically suspected as lymphadenopathy, out of which only three cases showed features of granulomatous lymphadenitis and rest of the cases had variable findings such as fibroadenoma of ectopic breast, schwannoma, pilomatricoma, and metastatic squamous cell carcinoma. Among the various cytological findings, there were cases such as schwannoma, pilomatricoma, and fibroadenoma of ectopic breast which are rare in the axillary region with few reported cases so far.
Cytological findings
Reactive lymphadenitis About 23 cases (30.6%) showed the presence of polymorphous population of lymphoid cells at various stages of maturation comprising of predominantly small lymphocytes with a variable number of centrocytes, centroblasts, immunoblastic cells, and also tingible body macrophages with occasional cases showing variable amounts of plasma cells. The smears were moderately to highly cellular. There was no evidence of granulomas or any atypical cells in these smears. 14 of these were clinically diagnosed as tubercular lymphadenitis, whereas the rest nine were clinically suspected to have metastases from breast carcinoma (Table 1).
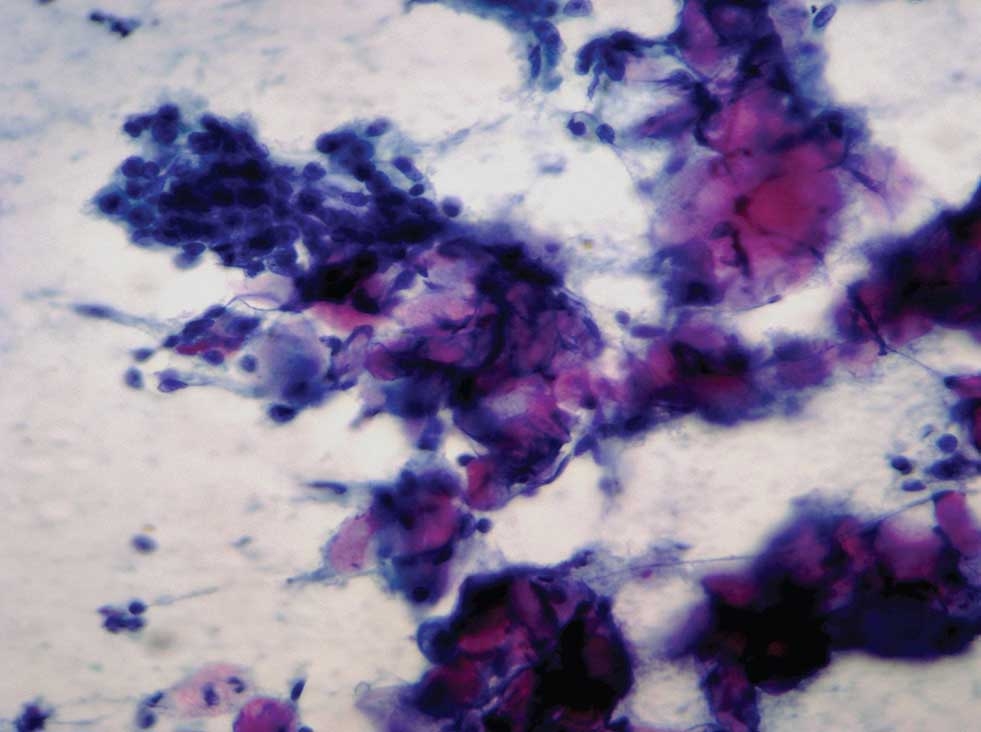
Metastatic infiltrating ductal carcinoma This was seen in nine cases (12%). The cytological features included clusters and sheets of malignant ductal epithelial cells. Individual cells were pleomorphic with high N:C ratio, moderate cytoplasm, round to oval nuclei with irregular margins and coarse clumped chromatin. Background showed hemorrhage and necrosis (Figure 2).
Acute suppurative lymphadenopathy Plenty of neutrophils along with macrophages (both intact and degenerated) were seen against necrotic background in five cases (6.6%). Occasional tingible body macrophages were also seen along with degenerated lymphoid cells (Figure 3).
Tubercular lymphadenitis Out of the 23cases clinically suspected as tubercular lymphadenitis only four cases (5.3%) showed the consistent findings. The smears showed abundant caseous necrosis along with polymorphous population of lymphoid cells. Occasional multinucleated giant cells of Langhan’s type were also seen. ZN stain revealed the presence of acid-fast bacilli (AFB) in both the cases (Figure 4).
Granulomatous lymphadenitis Three cases (4%) were diagnosed cytologically as granulomatous lymphadenitis. The smears showed the presence of well-formed epithelioid granulomas against background showing polymorphous population of lymphoid cells at various stages of maturation (Figure 5). There was no evidence of necrosis or atypical cells in the smears. ZN stain done on the smears did not reveal any acid-fast bacteria. FNAC material subjected to culture also did not yield any results.
Lipoma About 16 cases, out of the total 75 cases (21.3%), were cytologically diagnosed as lipoma. The smears showed sheets and clusters of benign mature adipocytes along with fibrous stromal fragments.
Ectopic breast This comprised 5% (4/75) of all cases. The smears showed presence of benign ductal epithelial cells arranged in monolayered sheets of variable shapes and sizes along with overriding myoepithelial cells (Figure 6).
Fibroadenoma of ectopic breast This was seen in three cases (4%) all of which were clinically suspected as lymphadenopathy. The smears showed bimodal cell population comprising of benign ductal epithelial cells and myoepithelial cells. The ductal epithelial cells were arranged in monolayered sheets and staghorn pattern against background showing numerous bare bipolar nuclei and stromal fragments (Figure 7).
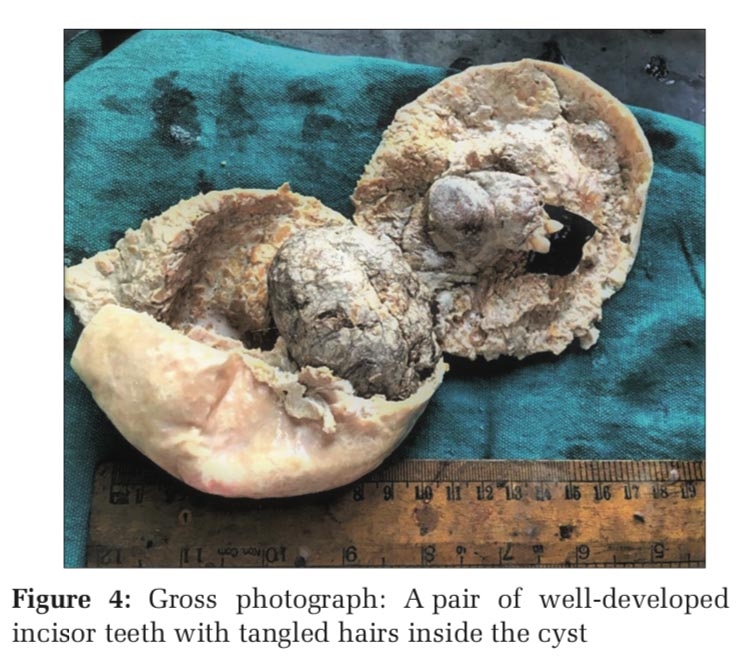
Epidermal cyst Three cases (4%) showed the presence of plenty of anucleate squames against a clean background (Figure 8).
Schwannoma This comprised 2.6% (2/75) of all cases. The smears showed cohesive clusters of spindle cells against a fibrillar intercellular stromal background. Individual cells were spindle with moderate cytoplasm, elongated slender nuclei, and bland chromatin. At places nuclear palisading was also seen (Figure 9).
Pilomatricoma One case (1.3%) showed the presence of clusters of basaloid cells along with sheets of degenerate, anucleate, and keratinized squamous cells (ghostcells). Acytological diagnosis of pilomatricoma was given (Figure 10).
Metastatic squamous cell carcinoma One case (1.3%) had a previous history of squamous cell carcinoma of the right forearm and had presented with swelling in the right axilla 6 months after treatment of the forearm lesion. The case was clinically suspected as reactive lymphadenopathy. The cytology smears showed presence of malignant squamous cells arranged in clusters, sheets and singles against background showing keratinous debris. Individual cells were pleomorphic with high N:C ratio with moderate cytoplasm and round to oval hyperchromatic nuclei with irregular margins and prominent nucleoli (Figure 11).
Metastatic poorly differentiated malignancy This was seen is a single case (1.3%) where a 50-year- old female presented with disseminated malignancy and multiple lymphadenopathies. FNAC from axillary swelling was done. The smears showed disseminated population of poorly differentiated malignant cells. Individual cells were highly pleomorphic with high N:C ratio, moderate to abundant cytoplasm, round to oval nuclei with irregular margins and coarse clumped chromatin with occasional nucleoli. Few cells showed cytoplasmic vacoulations (Figure 12).
As histopathological confirmation of these lesions were not done hence false positives, and true negatives could not be calculated. Cytopathological diagnoses were compared with the clinical diagnoses. As 33 cytological diagnoses were concordant with the clinical diagnosis, these were true positives. Hence, the diagnostic accuracy of this test was 44% and sensitivity was 44%. The sensitivity and diagnostic accuracy for detection of carcinoma was 66.66%. The concordance rate of this study was 44%, and discordance rate was 56%. The low sensitivity was due to the discordance between the clinical and cytological correlation.













The axilla is a pyramid-shaped area which is spaced between the chest wall and the upper part of the arm.
It comprises a truncated apex, a concave base and four walls (anterior, posterior, medial and lateral). The various contents of axilla consist of the axillary artery with its branches, the axillary vein with its tributaries, brachial plexus cords with their branches, axillary lymph nodes with their connections, axillary fat and occasionally axillary tail of breast. The lymph nodes are 20-30 in number. These are the anterior, posterior, lateral, central, and the apical groups. The anteriorgroupreceiveslymphfromthemajorpart of the breast, whereas the posterior group receives lymph from the axillary tail of the breast. The apical group receives lymph from the upper part of the breast. Hence, any disorder involving these structures can lead to a mass in the axillary domain.[8]
The axillary lesions frequently encountered are usually lymphadenopathies. Apart from the lymph nodes, the other mesenchymal tissues present in the axillary region can also give rise to various lesions. These lesions may include accessory ectopic breast tissue and related lesions, lipomas, hemangiomas, hamartomas, fat necrosis, epidermal cysts, and also rare lesions like schwannomas, malignant fibrous histiocytomas. Various ectopic breast tissues related lesions in the axillary region may include fibroadenomas and primary carcinoma of ectopic breast tissue. Furthermore, certain surgery related masses such as seromas, old hematomas, and lymphangiectasia may frequently occur. Rarely in this context, suture granulomas and pseudoaneurysms may occur.[1]
In the various prior studies done on axillary lesions, cytology, imaging techniques, and sometimes histopathology were undertaken for diagnosis.[1,4-7,9,10] Studies by Dey et al. and Das et al. did a cytological and clinical correlation, though both the studies dealt with just axillary accessory breast tissue.[6,7]
In this study, reactive lymphadenitis was the most common cytological diagnosis followed by lipoma and metastatic lymphadenopathy. There were two cases of schwannoma which is rarely seen in the axillary region. There was one case of pilomatrixoma which too is rare in this region.
Four cytomorphological patterns of lymphadenopathy were seen in this study, viz. Reactive pattern, granulomatous, tubercular, and acute suppurative.
The diagnostic criteria for reactive lymphadenopathy consist of a high cell density along with clear polymorphic patterns of cells without malignant features and considerable amount of tingible body macrophages.[11] However, the yield in case of a reactive lymphadenopathy may vary according to the degree of stimulation, number and size of germinal centers and also the fact that various zones of a lymph node may result in different types of yields. Germinal center material usually consists of poorly defined tissue fragments of poorly cohesive cells comprising of centroblasts, centrocytes, tangible body macrophages, and a number of lymphocytes adhering to syncytial cytoplasm of dendritic reticulum cells. Smear derived from the interfollicular tissue mainly shows lymphocytes with small and variable amounts of scattered immunoblasts, non-specific histiocytes, plasma cells, and endothelial cells.[12] The 23 cases diagnosed cytologically as reactive lymphadenopathy in the present study showed similar findings.
Granulomata are recognized cytologically by observing cohesive clusters of histiocytes of epithelioid type with or without associated multinucleated giant cells. Adirty necrotic background if present would suggest caseation and possibly tuberculosis.[12] Apart from tuberculosis, granulomatous inflammation in lymph nodes may be encountered in various non-neoplastic as well as neoplastic conditions. Non-neoplastic causes may include toxoplasmosis, atypical mycobacterial infection, sarcoidosis, leprosy and cat scratch disease. Neoplastic causes can be Hodgkin disease, non-Hodgkin lymphoma, and metastatic carcinomas.[12,13]
However, in some cases, the exact etiology of granulomatous reaction may remain occult as was seen in three cases in this study.
Granulomata with caseous necrosis are the hallmark of tuberculous lymphadenitis. The absence of necrosis does not rule out tuberculosis, and ZN staining for AFB is imperative in all cases of granulomatous lymphadenitis. In immunocompromised patients, FNAC from tuberculous lymph nodes may show only necrotic debris without histiocytes, as was seen in four cases in our study. In such cases demonstration of AFB both in direct smears and culture from aspirate is necessary.[12]
Sen et al. in their study have given the spectrum of cytomorphological pattern that can be seen in tubercular lymphadenitis. They further stressed that unless AFB is demonstrated, diagnosis of tuberculosis is difficult in cases when smears are richly cellular with an occasional cluster of epitheliod cell and absence of necrosis. In such cases, other granulomatous conditions need to be taken into consideration.[14] Further, Das et al. also suggested the importance of AFB demonstration in smears where only necrotic material was seen in FNAC smears, as was seen in our study.[15]
The smears of acute suppurative lymphadenitis are usually highly cellular and dominated by polymorphonuclear cells in large numbers. Polymorphs in the smears may be both intact and degenerated. Lymphoid cells may show degenerative changes.[11] Similar findings were seen in five cases in this study. Lupus lymphadenopathy can also result in a suppurative aspirate.[11] When only necrotic material and few leucocytes are seen, the possibility of sterile pus (antibioma) or tumor necrosis needs to be ruled out.[15]
The overall survival and management of a patient with breast cancer depend greatly on the detection of metastases in axillary lymph nodes. Hence, it poses as a very important prognostic factor and also helps the surgeon to select the type of axillary lymph node dissection to be performed. Pre-operative detection of axillary lymph node metastasis can be done using various techniques.[16] FNAC is a well-established diagnostic method with rapid access for the evaluation of suspected cases with metastatic disease in follow-up of breast carcinoma. As compared to clinical examination or sonological analysis alone, FNAC has proved to be more valuable in the evaluation of suspicious lymph nodes. Evaluation of lymph node status of newly diagnosed cases of breast cancer by clinical examination only can be difficult at times, as large reactive nodes may be mistaken for metastatic nodes and very small nodes may be missed out on palpation.[17] This also could be a cause of discrepancy in the clinical and cytological diagnosis as seen in the present study. Out of the 18 cases suspected to have metastasis from breast carcinoma in this study, only nine showed positive findings. The other nine cases showed features of reactive lymphadenitis.
These false negative cases (9/18) could have been avoided if sonographical modality was also explored in diagnosis. The most common cause of false negative result is the failure for accurate localization of the lesion, which can be overcome with the aid of imaging techniques.
The sensitivity of FNAC to detect metastases of carcinoma breast in axillary lymph nodes was 66%. This was more as compared with the study by Alkuwari et al.[18] (sensitivity was 60%) and less as compared to the study by Hammom et al.[10] (sensitivity was 100%).
The presence of accessory breast tissue is rare with a prevalence of 0.6-6%.[19] Failure of involution of the mammary ridge can give rise to ectopic breast tissue. The mammary milk lines, which extend from the groin to axilla, develop along the sides oftheembryoduringthe6thweekofembryonic life.[20] An accessory breast can occur anywhere along the milkline but is most frequently found in the axillary region and is usually subjected to changes similar to the eutopic breast. Sometimes, it becomes difficult to tell whether it is an accessory breast or an extension of normal breast parenchyma toward the axilla, although the superficial location of the accessory breast and the characteristic mammographic features are helpful.[20] At times the palpable accessory breast in the axilla may have monthly premenstrual changes such as tenderness and swelling.
Fibroadenomas, though relatively frequent and the most common benign neoplasm of the breast, are rarely found in the axillary ectopic breast tissue with few reported cases so far.[21,22] Smears from non-neoplastic breast and fibroadenoma show a bimodal cell population, with smears of fibroadenoma being more cellular. The triad of cellular smears with bimodal cell population, many bare bipolar nuclei lying singly and fibromyxoid stromal fragments in the background points towards a diagnosis of fibroadenoma. In case, the fibromyxoid fragments are not seen then the presence of many single bare bipolar nuclei suggests a diagnosis of fibroadenoma.[23] The three cases of fibroadenoma in our study did not show any fibromyxoid stromal fragments.
Epidermal inclusion cysts, also known as sebaceous cysts, are one of the most commonly encountered lesions. We have reported three such cases in our study. Various complications may arise in cases of epidermal cysts like rupture and development of squamous cell carcinoma. Rupture of epidermal cysts may result in foreign body giant cell reaction, granulomatous reaction or formation of abscesses.[1]
Lipomas are benign fatty tumors and may occur in any location. These were the second most common cytological diagnosis in our study.
Pilomatrixoma, also known as calcifying epithelioma of Malherbe, is a tumor of skin appendage, which originates from the hair matrix. It usually occurs on the face or upper extremities. It rarely occurs in the axilla.[24] Only one case was found in this study. Smears from pilomatrixoma show sheets of anucleate and keratinized squamous cells along with clusters of basaloid cells. Background may show calcific debris along with inflammatory infiltrates and also giant cells of foreign body type. Cytological diagnosis of pilomatricoma may be difficult at times due to the predominance of one component over the other. A predominance of basaloid cells may lead to a misdiagnosis of malignancy, while the presence of only keratinous debris or ghost cells along with foreign body type giant cells may arise suspicion of epidermal cyst.[25] Our case showed the presence of all the elements of pilomatrixoma thus helping in the diagnosis.
Schwannomas are benign neoplasms that originate from Schwann cells and are most frequently seen in the extremities, trunk, and head, with very rare cases presenting in the axillary region.[1,26] We found two cases of schwannoma in our study.
Metastatic squamous cell carcinoma in axilla is rare and carries a poor prognosis.[27] We found a single case of metastatic axillary squamous cell carcinoma. The patient gave a history of squamous cell carcinoma of the forearm and had presented with an axillary swelling 6 months after the treatment of the forearm lesion.
Metastasis of poorly differentiated malignancy to axillary lymph node is another rare condition with unfavorable outcome. In a study conducted by Pentheroudakis et al., the mean age of the patients presenting with axillary metastasis of poorly differentiated carcinoma of unknown origin was found to be 52 years which correlated with the single case in our study which presented with similar findings.[28]
Sensitivity and diagnostic accuracy depend on the number of false negatives. Hence, complete and accurate physical examination of the axillary masses aided by guidance methods can definitely improve the clinical diagnosis and hence the concordance rate and the sensitivity.
FNAC is a safe, easy and a cheap diagnostic tool to decipher the benign or the malignant nature of the swelling. It is a rapid, outpatient based, accurate procedure and helps in diagnosis of benign as well as malignant lesions in experienced hands with less chances of false negative results. This study also stresses the importance of accurate physical examination of swellings and takes the aid of imaging wherever needed. This study highlights the gamut of lesions the axilla can harbor which are accessible for timely diagnosis by the invaluable procedure of FNAC.
Subscribe now for latest articles and news.