Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2022.v8i1.20
Year: -0001, Volume: 8, Issue: 1, Pages: 8-13
Original Article
Shulbha V Sejekan1 , Dayananda S Biligi2
1Associate professor, Department of Pathology, Bangalore Medical College & Research Institute, Bangalore, India,
2Professor & HOD, Department of Pathology, Bangalore Medical College & Research Institute, Bangalore, India
Address for correspondence: Shulbha V Sejekan, Associate professor, Department of Pathology, Bangalore Medical College & Research Institute, Bangalore, India.
E-mail: [email protected]
Background: Skin is a complex organ composed of epidermis, dermis and skin adnexa producing multitude of tumors. The skin adnexal neoplasms are classified into sub-groups, depending on their differentiation towards hair follicles, sebaceous, apocrine and eccrine glands. Clinically adnexal neoplasm presents as asymptomatic papules or nodules, having non-specific morphological appearance and therefore histopathology is the gold standard for their confirmatory diagnosis. The aim is to assess clinico-histopathological characteristic features of the skin lesions, subtype and to pick up certain subtle features that clinch the diagnosis towards their line of differentiation. Methods: The study has been conducted in the Department of Pathology, for a period of one year. The total numbers of cases with histopathological diagnosis of skin adnexal lesions are 105. Ethical clearance for the same has been obtained by the Head of Institution. Skin biopsy specimen are received and processed in the histokinette; paraffin embedded blocks made and stained with Hematoxylin & Eosin stain. Special stains when required have been used. Descriptive statistics have been used in analysis of the results. Result: The total number of cases with histopathological diagnosis of skin adnexal lesions is 105. Among them 99/105 cases (94.3%) are benign and malignant counterparts comprised of 6/105 cases (5.7%).Overall lesions with hair follicle differentiation comprised of 73.3% (77/105), followed by sebaceous differentiation of 15.3% (16/105) and eccrine differentiation of 11.4 % (12/105). Conclusion: This study emphasized that histopathological examination, plays an essential role in studying the skin adnexal tumors, owing to its indistinctive clinical presentation.
Keywords: Adnexal, Eccrine, Skin, Tumor, Sebaceous, Apocrine
Skin is a complex proficient organ composed of epidermis, dermis and skin adnexa that procreates a multitude of tumors.[1,2] The skin adnexal neoplasms are classified into sub-groups, depending on their differentiation towards hair follicles, sebaceous, apocrine and eccrine glands.[3] They arise from the multi- potent undifferentiated stem cells, which in due time differentiates into specific pathways. This doctrine explains the fact that adnexal neoplasm
can resemble their mature counterparts and different histopathological appearance in the same tumor would be precisely because of multiple differentiation pathways of stem cells.[4] This signifies that though most of the adnexal neoplasms are benign in nature, they are genetically predetermined which in course of time become pre-malignant and aggressive in nature.[5]
Clinically adnexal neoplasm presents as asymptomatic papules or nodules, having non-specific morphological appearance and therefore histopathology is the gold standard for their confirmatory diagnosis.[6] The added advantage of histopathological examination is that it will also yield the prevalence of pre malignancies, which would otherwise be missed in the routine clinical workup and even with usage of sophisticated technologies such as computerized tomography.
The aim of the present study is to assess the clinico-histopathological characteristic features of the skin lesions, subtype the lesions and to pick up certain subtle features that can clinch the diagnosis towards their line of differentiation. The unique feature of this study is that it is making a maiden attempt to re-categorize the skin adnexal neoplasm based on pattern analysis, which would aid in a better understanding of the general concepts in cutaneous pathology, helping the enthusiastic pathologists.
The study has been conducted in the Department of Pathology, for a period of one year. The total number of specimens including biopsies sent for the histopathological examinations are 4000, of which skin biopsies are 1100. The total number of cases with histopathological diagnosis of skin adnexal lesions are 105, has been included in the study. Ethical clearance for the same has been obtained by the Head of Institution [Reference numberBMCRI/PS/344/2015-16]. Clinical data of patients has been documented.
Skin biopsy specimen in properly labeled containers, fixed in 10% formalin solution have been received and processed. Gross examination in form of size of biopsy, type of biopsy (punch biopsy/excision biopsy) has been performed. External changes and cut surface changes such as areas of hemorrhage, necrosis, calcification and mucoid change have been documented. These biopsies have been processed in the histokinette; later paraffin embedded blocks have been made. The sections are stained with Hematoxylin & Eosin stain. Special stains when required have been used. Descriptive statistics have been used in analysis of the results.
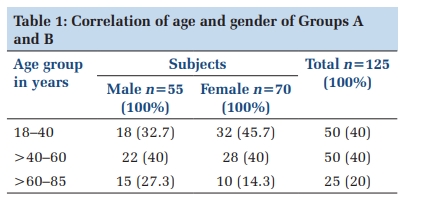
The total number of cases with histopathological diagnosis of skin adnexal lesions is 105. The male to female ratio is 1.2:1. The age group ranged from 02 years to 75 years, with a mean age of occurrence of 38.5 years. The most commonly involved site is head & neck region (95%), followed by hand (03%) and abdomen (02%). Among them 99/105 cases (94.3%) are benign and malignant counterparts comprised of 6/105 cases (5.7%). Overall lesions with hair follicle differentiation comprised of 73.3% (77/105), followed by sebaceous differentiation of 15.3% (16/105) and eccrine differentiation of 11.4 %( 12/105).
Adnexal lesions with hair follicle differentiation: In our study, lesions with hair follicle differentiation are the commonest (73.3%). Among these, commonest are pilomatricoma in 25/77 cases (32.4%), followed by trichilemmal cysts in 23/77 cases (29.8%), pilar sheath acanthoma with keratoacanthoma in 19/77 cases (24.6%), proliferating trichilemmal tumor in 4/77 cases (5.2%), trichoepithelioma in 3/77 cases (3.9%), trichofolliculloma in 02/77 cases (2.6%) and trichoblastoma in 01/77 cases (1.5%). The mean age of occurrence is 40 years, commonly involving head & neck region, followed by abdomen.
Adnexal lesions with sebaceous differentiation: Sebaceous differentiation is noted in 16/105 cases (15.3%). Commonest is sebaceous hyperplasia in 11/16 cases (68.6%) followed by malignant counterpart of sebaceous carcinoma in 05/16 cases (31.4%). Mean age of presentation is 49 years, predominantly occurring in head & neck region. Adnexal lesions with eccrine differentiation: Tumors with eccrine differentiation is seen in 12/105 cases (11.4%). Benign lesions are commonest which included 11/12 cases (91.6%), followed by a single case of poro carcinoma (8.4%). Among the benign tumors, eccrine poroma is commonest, seen in 05/12 cases (41.6%), followed by eccrine spiradenoma in 03/12 cases (25%), chondroid syringoma in 02/12 cases (16.6%) and a single case of eccrine cylindroma (8.4%). Mean age of presentation is 54.2 years, commonly occurring in head & neck region, followed by hand.
Skin adnexal tumors are amalgamating group of primary skin tumors. Their prevalence among the tumors in the human body is variable. Our study, showed histopathological prevalence of adnexal tumors over a period of one year, studied among the 4000 pathology records as 2.6% (105 cases). The study conducted by K Kamyab Hesari et al,[7] reported a prevalence rate of 3.3%, in a period of 04 years. However, other studies have reported a lower prevalence. In a study conducted by Kaur K et al,[8] their prevalence rates were 0.3%, while a study conducted in Nigeria,[9] showed 0.9% prevalence rate. Many reasons can be cited for a higher prevalence rate in our setup. The most important is that ours being a combination of an academic, tertiary care and a referral center, it may be possible that patients have been referred here and the increased rate of excision biopsies performed with availability of better treatment modalities would have aided in an overall upsurge in the diagnosis of skin adnexal lesions.
Our study showed higher occurrence of skin adnexal tumors in male as compared to females. Ankit S et al,[10] in his study showed male to female ratio as 1.07:01. Similar male predominance was noted in study by Yaqoob N et al.[11] The mean age of occurrence in our study is 38.5 years. K Kamyab Hesari et al,[7] also showed similar findings, with mean age of occurrence of 34.5 years. However, we went ahead and calculated mean age of occurrence in skin adnexal tumors with different lines of differentiation which varied accordingly. The mean age affecting tumors with hair follicle differentiation is 40 years, 49 years in tumors with sebaceous differentiation and 54 years in eccrine differentiated tumors. The commonest site of involvement is head & neck region in our study. Consistent results were found in study conducted by Ankit S et al[10] and K Kamyab Hesari et al.[7] The pilosebaceous and eccrine glands are magnanimously distributed over the head & neck region, providing a hebetic soil for evolution of maximum skin adnexal lesions.[7]
In our study, the incidence of benign lesions (94.3%) is more compared to malignant counterpart (5.7%). It was tandem with other studies conducted by Vani et al,[12] Shukla P et al,[5] Samaila et al,[9] and Vaibhavi Bani et al.[1] These tumors basically originate from undifferentiated pluripotent stem cells, determining its preponderance to behave in a benign fashion. These tumors are influenced by genetics, local vascularity, and microenvironment of epidermis & dermis in its malignant transformation.[3,13] It should
be kept in mind that, benign tumors should be completely excised with larger excisional margins as recurrence and malignancy tends to occur if incompletely excised.[11] Malignant counterparts are rare, but locally aggressive, so they are more prone for lymphatic and hematogenous metastasis carrying poor prognosis. The benign nature of the lesion is ascertained by the fact that they clinically present as asymptomatic papules & nodules, have a long history & duration of symptoms. Patients often seek medical attention, only when they are cosmetically dis-figuring.[14,15]
Our study showed that pilar tumors are the commonest followed by sebaceous gland tumors and sweat gland tumors. Review literature and studies,[12,16,17] shows that tumors with pilar differentiation were usually not as common to sweat gland and sebaceous gland differentiated tumors. However, Yaqoob N et al,[11] in his study showed 41.6% with combined pilosebaceous differentiation. In our study, lesions with hair follicle differentiation comprised of 73.3% of the total burden. Among them, pilomatricoma is the commonest. They are microscopically characterized by tumor islands with two types of cells, basophilic cells with elongated nuclei and cells with eosinophilic cytoplasm (shadow cells) and central region of ghost cells (Figure 1 a, b). Areas of calcification and foreign body giant cell reaction can also be seen.[3,17]
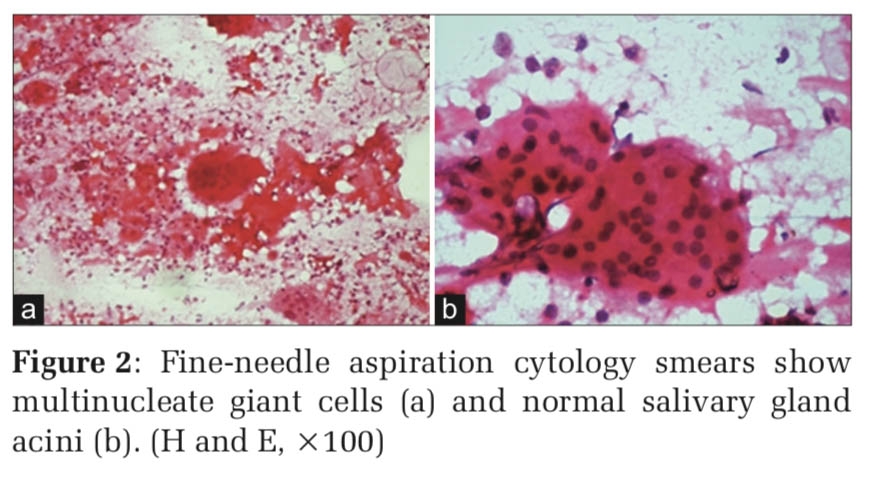
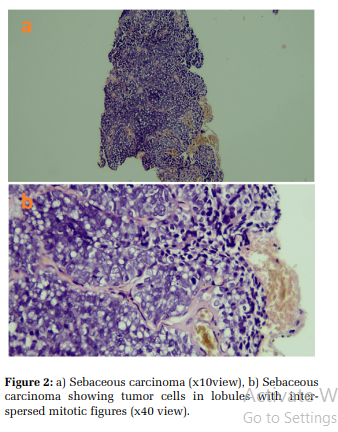
In our study, lesions with sebaceous differentiation are the second commonest, comprising of 15.3% of the total skin adnexal lesions. Majority of them are benign in nature comprising of 68.6%. They were predominantly sebaceous hyperplasia (68.6%), followed by a malignant counterpart of sebaceous carcinoma (31.4%). A study conducted by Saha A et al,[15] also showed sebaceous hyperplasia as the commonest. Sebaceous hyperplasia microscopically appears as large number of mature sebaceous lobules with an overlying normal looking epidermis. Its malignant counterpart is sebaceous carcinoma. Sebaceous carcinomas have been seen to occur in old age and around eye & lid margin in our study. Microscopically they show irregular lobules and sheets of cells with sebaceous differentiation (Figure 2 a, b). Marked nuclear atypia and abnormal mitotic figures are also seen in the tumor proper.[18] Eccrine tumors comprised of 11.4% in our study. The benign tumors are the commonest with percentage of 95.5% and 8.5% are malignant. Benign lesions encountered in our study are eccrine poroma, eccrine spiradenoma, chondroid syringoma and cylindroma. A single case of porocarcinoma has been documented in our study. The convoluted nature of the sweat gland may be culpable for the development of this wide multitude of tumors. [9] Eccrine poroma histologically showed a lobulated tumor growing downwards into dermis as broad band of epithelial cells. The tumor masses showed two types of cells. One type showed round cells with basophilic cytoplasm, the other cell type showed round cells with dark nuclei and clear cytoplasm. Periodic acid Schiff stain showed the clear cytoplasm was due to presence of glycogen.[3] Eccrine spiradenoma (Figure 3 a, b), microscopically showed a highly cellular tumor with sharply demarcated lobules containing intertwining cords of epithelial cells, separated by a fibrous stroma.[3] Chondroid syringoma showed a biphasic tumor with epithelial component comprising of tubular lumina lined by bilayered epithelial cells in a chondroid matrix. We encountered a single case of cylindroma, histologically showing basaloid cells nests arranged in jigsaw puzzle with dense basement membrane material at its periphery.[3,17] A single case of porocarcinoma is seen in elderly male, over the neck region in our study. The eccrine porocarcinoma showed the morphology of the benign counterpart with superimposed features of a neoplastic process, in form of infiltrating growth pattern, desmoplastic stromal reaction, high degree of cytological atypia and hyperchromasia.[18]
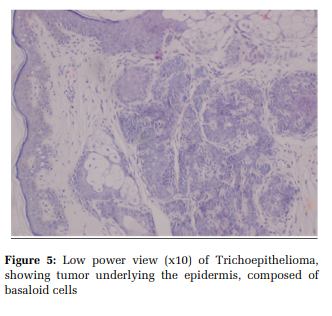
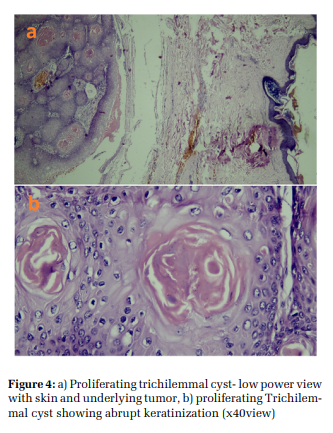
Morphologically, our study pondered a step ahead, and we made a sincere attempt to re-categorize the skin adnexal tumors, depending on their predominant pattern under the microscope. They were divided into cystic lesions, basaloid tumors, squamoid tumors and glandular tumors. The cystic lesions comprised of predominantly cysts with squamous keratinization. We included proliferating trichilemmal cyst (Figure 4 a, b) and pilomatricoma with cystic change in this category. Basaloid tumors showed presence of small, round basaloid cells. We included trichoblastoma, trichoepithelioma (Figure 5), cylindromas and eccrine spiradenoma in this category. In tumors with predominantly squamoid differentiation, we sub typed as solid lobules with eosinophilic cells like pilar sheath acanthoma and lobules with clear cell change as in hidreadnoma. In glandular tumors, we included chondroid syringoma. This classification was done to stress upon the importance of pattern recognition in dermatopathology. The pathological outcome for this morphological classification emphasized on a better understanding of the morphology of skin adnexal tumors under the microscope.This study therefore signified that histopathological examination, thus forms a sole and an essential tool in studying the skin adnexal tumors, owing to its indistinctive clinical presentation.[7] Most of the skin adnexal tumors are benign in nature, hence wide excision performed by clinicians is therapeutic in nature. The clinical outcome for most of the skin adnexal tumors are favorable, since excision biopsy in curative. However, the early recognition of these skin adnexal tumors are also important, because of the fact, that sometimes they provide signs of certain syndromes associated with internal malignancies.[6,11]
Skin adnexal tumors constitute small proportion of dermatological disorders and the burden of tumors of rest of the body. As they present as asymptomatic papules and nodules, clinical diagnosis may be difficult at times, thus empowering the histopathological examination as a gold standard in the diagnostic modality. This can thus increase the rate of diagnosis and aid in a better therapeutic intervention. Thus, we can gain the acquaintance of these groups of tumors, which has been so elaborately classified but over sightedness in clinical practice, owing to its asymptomatic nature and longer duration of the symptoms.


Subscribe now for latest articles and news.