Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 2, Pages: 162-165
Case Series
Sumanta Laha1 , Amaresh Roy2 , Sushama Saren2 , Tarak Nath Ghosh3
1Associate Professor, Department of Pediatric Medicine, Burdwan Medical College and Hospital, Burdwan, West Bengal, India,
2 Junior Resident, Department of Pediatric Medicine, Burdwan Medical College and Hospital, Burdwan, West Bengal, India,
3Professor, Department of Pediatric Medicine, Burdwan Medical College and Hospital, Burdwan, West Bengal, India
Address for correspondence: Sumanta Laha, Associate Professor, Department of Pediatric Medicine, Burdwan Medical College and Hospital, Burdwan, West Bengal, India.
E-mail: [email protected]
Received Date:08 August 2021, Accepted Date:30 May 2022, Published Date:03 September 2022
Post COVID-19 MIS-C cases are on the rise recently and various cardiac abnormalities are reported among them in different literature. Here we have presented six cases of MIS-C with significant echocardiographic abnormality. They have a varied presentation like acute encephalitis, acute renal failure, incomplete Kawasaki, shock or acute gastroenteritis along with fever. Our cases have raised inflammatory markers like ESR, CRP, IL-6 with increased D-dimer, CPK-MB and positive COVID serology. Except case5, none has any cardiovascular presentation but every case has some important echocardiographic finding. Mild pericardial effusion was present in two cases, gross LV systolic dysfunction with LVEF 40-45% in one case, significant coronary artery dilatation in three cases and valvular abnormality like MR or TR in three cases. So it is extremely important to evaluate every case of MIS-C with proper echocardiography even if they had no cardiac manifestation at presentation to prevent complication afterwards.
Keywords: COVID -19, MIS-C, Echocardiography
Though COVID -19 seems to be relatively benign in nature in pediatric population initially, but there is a recent rise of post COVID complication (2-6 weeks after SARS-CoV-2 infection) known as Multisystem Inflammatory Syndrome in Children (MIS-C) causing concerns. 1 There may be silent cardiac damage in a case of MIS-C without any overt cardiovascular manifestation. Here we describe a series of six MIS-C cases with varied presentation, but all with serious cardiac involvement.
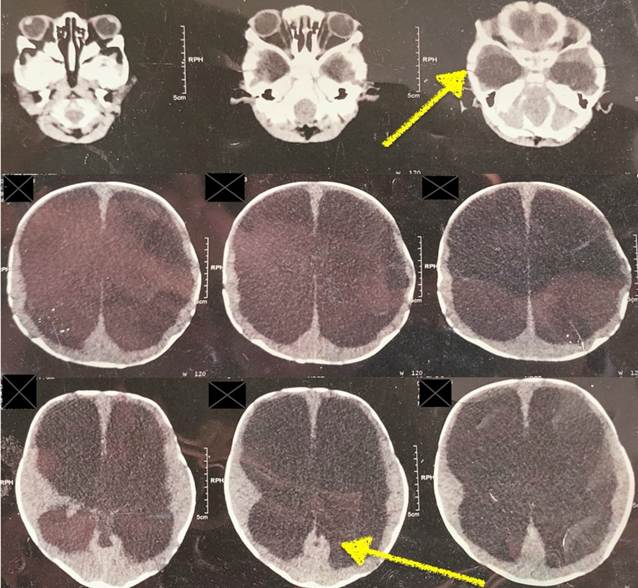
In the following three tables we have documented the age, sex, varied clinical presentations, important laboratory parameters and notable echocardiographic findings of our six MIS-C cases. We found most cases above nine years of age with male predominance and all admitted with more than three days fever. Gastrointestinal symptoms like diarrhea, vomiting or abdominal pain is the commonest presentation. Kawasaki like features like maculopapular rash, non-purulant conjunctivitis and pedal edema either singly or in combination is the next common presentation. One case presented with features of AES, like vomiting, convulsion and disorientation. Another child came with acute renal failure with oliguria for last 48 hrs along with hypotension and shock. Among other cardiovascular manifestations some unexplained tachycardia and faint systolic heart murmur were present in two cases. Leucocytosis with neutrophilia and lymphopenia (neutrophil, lymphocyte ratio>3:1) and elevated inflammatory markers like ESR, CRP, IL-6 are present in most cases.
|
|
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
Case 6 |
|
Age ( in year) |
10 |
11 |
2 |
6 |
11 |
11 |
|
Sex |
Male |
Male |
Male |
Male |
Female |
Male |
|
Fever > 3 days |
4 days |
5 days |
6 days |
4 days |
7 days |
10 days |
|
Maculop-apular Rash |
- |
+ |
+ |
- |
- |
- |
|
Conjunc-tival congestion |
+ |
+ |
- |
- |
- |
- |
|
Diarrhrea/ |
+ |
+ |
- |
+ |
- |
+ |
|
Abdomin-al pain |
+ |
+ |
- |
- |
+ |
+ |
|
Hypotensi-on, Shock |
- |
- |
- |
- |
+ |
- |
|
Kawasaki like presenta-tion |
- |
+ |
- |
- |
- |
- |
|
Acute encephal-opathy (AES) |
- |
- |
- |
+ |
- |
- |
|
Acute renal failure (ARF) |
- |
- |
- |
- |
+ |
- |
|
|
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
Case 6 |
|
WBC count(4.5-11x109/L) |
16 |
16.5 |
8.2 |
16.2 |
22.8 |
9.2 |
|
Neutrophil(%) |
78 |
88 |
67 |
85 |
78 |
65 |
|
Lymphocyte(%) |
20 |
11 |
28 |
10 |
20 |
25 |
|
Platelet(150-400x109/L) |
138 |
156 |
560 |
236 |
287 |
222 |
|
C-reactive protein(<10mg/L) |
84 |
85.5 |
3.5 |
69 |
56 |
66 |
|
ESR(<10mm/hour) |
55 |
65 |
52 |
60 |
38 |
22 |
|
D-dimer (<0.5mg/L FEU) |
1.22 |
8.27 |
0.92 |
4.95 |
4.32 |
1.62 |
|
Interleukin 6(<7 pg/ml) |
853 |
>5500 |
>5500 |
910 |
2365 |
>5500 |
|
CK-MB(5-25 IU/L) |
38 |
28 |
27 |
27 |
81 |
51 |
|
Serum Creatinine (0.5-1mg/dl) |
0.7 |
0.9 |
0.5 |
0.7 |
3.7 |
0.8 |
|
SARS –CoV -2 RTPCR |
- ve |
- ve |
- ve |
- ve |
- ve |
- ve |
|
SARS –CoV-2 IgG antibody |
+ ve |
+ ve |
+ ve |
+ ve |
+ ve |
+ ve |
|
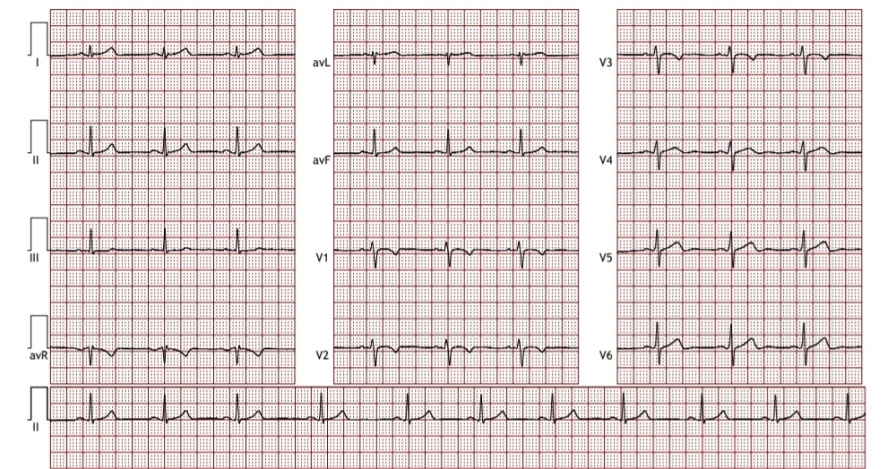
Echocardiographic findings |
|||
|
|
Coronary artery Dimension |
Pericardial effusion |
Other cardiac dysfunction |
|
Case 1 |
Distal LMCA dilated (4.7mm) (z score 4.54). RCA at origin 3.2mm (z score 2.25) |
Absent |
Normal with LVEF 79% |
|
Case 2 |
Normal |
Minimal pericardial effusion |
Global hypokinesia of LV, LVEF 40-45%, mild MR, mild PHTN with TR |
|
Case 3 |
Proximal LAD ectatic (3mm) |
Absent |
Normal with LVEF 65%, (Z score 3.23) |
|
Case 4 |
Normal |
Absent |
Grade 2 MR, mild TR. LVEF 75% |
|
Case 5 |
Normal |
Thin layer of pericardial effusion |
Dyskinetic septal movement, with LV systolic dysfunction, mild TR , LVEF 53% |
|
Case 6 |
Ectatic segment in mid LAD (3.7mm) (z score 3.15) |
Absent |
Normal with LVEF 66% |
A case of MIS-C is defined by the following six criteria(WHO definition) 2; 1. Age 0 to 19 years, 2. Fever for ≥ 3 days, 3. Clinical signs of multisystem involvement (at least two of the following five): i) Rash or bilateral non purulent conjunctivitis or muco-cutaneous inflammation signs (oral, hands, or feet), ii) Hypertension or shock, iii) Features of myocardial dysfunction, pericarditis, valvulitis or coronary abnormalities (including echocardiographic findings or elevated troponin/NT-BNP), iv) Evidence of coagulopathy (prolonged PT, PTT, elevated d-Dimer), v) Acute gastrointestinal symptoms (diarrhea, vomiting or abdominal pain), 4. Elevated markers of inflammation (ESR, CRP or procalcitonin), 5. No other obvious microbial cause of inflammation, including bacterial sepsis and staphylococcal/streptococcal toxic shock syndromes, 6. Evidence of SARS-CoV-2 infection( RT–PCR, antigen test or serology positive)or contact with a case of COVID-19 present.
In our case series all the cases has meet the criteria of MIS-C, but their presentation is varied as reported in different literature. 3, 4 Some presented with AES like feature, some with ARF, hypotension and shock, some with kawasaki like presentation and some simply with rash or GI symptoms. Except one case with hypotension and shock, most of the other cases did not have any significant cardiovascular manifestation, but still every case showed some form of echocardiographic abnormality including significant coronary artery dilatation. Study by Matsubara D et al showed that myocardial injury is common in MIS-C, but coronary arteries may be spared in early MIS-C. 5 But various other studies described coronary artery dilatation or aneurysms in around 6-24% patients (mostly mild dilatation with score 2 to <2.5) 6, 7. In small aneurysm Z score is 2.5 to <5, medium aneurysm 5 to <10 and giant aneurysm 10 or more. In our study mostly we got small aneurysm in the coronary artery. Though rare but reports of large coronary artery aneurysms are there and even some of them developing after discharge. 8, 9, 10 This case series shows that coronary artery aneurysm similar to Kawasaki disease or other cardiac abnormality may be there in a case of COVID-19 MIS-C without any overt cardiovascular manifestation and presenting with different symptomology. Although further studies with more number of cases is needed to reach to the conclusion that significant number of MIS-C cases may have cardiac involvement with echocardiographic abnormality.
Proper echocardiographic evaluation is extremely important in every child with MIS-C irrespective of their clinical presentation both at admission and at follow up, as otherwise asymptomatic coronary artery dilatation may go unnoticed to cause complication afterwards.
Subscribe now for latest articles and news.