Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.22.281
Year: 2024, Volume: 10, Issue: 1, Pages: 96-103
Original Article
Michael Promise Ogolodom1 , Anthony Chukwuka Ugwu2 , Christopher O Akosile3 , Hyacienth Uche Chiegwu2 , Awajimijan Nathaniel Mbaba4 , Joseph C Eze2 , Daniel C Ugwuanyi2 , Robert O Akhigbe5 , Oluwafemi Olumide Egbeyemi6
1Department of Radiography, Faculty of Basic Medical Sciences, Rivers State University, Port Harcourt, Nigeria,
2Department of Radiography and Radiological Sciences, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi Campus, Nigeria,
3Department of Medical Rehabilitation, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi Campus, Nigeria,
4Department of Radiology, Rivers State University Teaching Hospital Port Harcourt, Nigeria,
5Department of Radiography and Radiation Sciences, Lead City University, Ibadan, Nigeria,
6City Gate Health Diagnostic Services, Ogun State, Nigeria
Received Date:06 June 2022, Accepted Date:03 April 2024, Published Date:22 April 2024
Background: It is not known to what extent differences in radiological findings of individuals with spinal pathologies may be associated with their quality of life (QOL) and the degree of disabilities. Objective: This study aimed at determining if QoL and degree of disabilities differs in individuals with cervical and lumbar spine pathology with different magnetic resonance imaging (MRI) findings. Methods: This cross-sectional study of 185 purposively sampled patients was carried out at Radiological facilities in Rivers State, Nigeria. Magnetic resonance images were assessed for pathological findings, Nurick grade scales and Short Form Health survey (SF-36) QoL questionnaire were used to assess participant’s disability grade and QoL respectively. Results: Majority of the participants with cervical (n=49, 64%) and lumbar (n=86, 79.8%) spine pathologies were males. Degenerative spine pathology was the most common in both the cervical (75%) and lumbar (80.7%) spine regions. The patients with cervical (n=30, 39.5%) and lumbar (n=56, 50.5%) spine pathologies had Nurick grade I and Nurick grade II respectively. There were statistically significant differences in the physical functioning domain (k=12.27, p = 0.03) and role limitations due to emotional problem domain (k= 13.03, p = 0.02) among individuals with different Nurick grades. Conclusion: Males were commonly affected by the spinal pathologies. Degenerative spinal pathology was the most common in both the cervical and lumbar spine regions. The most prevalent degree of disabilities associated with cervical and/or lumbar spine pathologies was Nurick grade I and II respectively.
Keywords: Disabilities, Pathology, Quality of life
Imaging of the spine plays an ever increasingly essential role in the diagnosis and treatment of cervical and lumbar spine disorders. The diagnostic approach for the evaluation of spinal pathologies should take into account the clinical manifestations of the conditions and the associated quality of life of the individual 1, because according to recent evidence, treatment pattern, which depends on the diagnosis, is associated with improved function and quality of life 2.
Quality of life is rapidly becoming a standard for evaluating outcomes in clinical trials, cost effectiveness analysis and clinical practice 3, 4. Pathologies of the lumbar and cervical spine can affect the QoL of the sufferer. Previous studies reported that by 7th decade, prevalence of spinal pathologies would have reached 95% in many individuals, and this increased the dependence rate and also decrease the quality of life (QoL) in older population 5, 6. The quality of life (QoL) outcome assessments are based on a number of clinician-scored grading scales. The oldest of them is the Nurick scores, which consist of five explanations of the effects of the conditions and is scored from 0 to 5, representing the degree of incapacitation of the affected individual.
Nonetheless, it is not known to what extent differences in radiological findings of individuals with cervical and lumbar spine pathologies may be associated with their quality of life and degree of disabilities. Therefore, this study was aimed at determining if the degree of disabilities and QoL outcome of individuals with cervical and lumbar spine pathologies differs with magnetic resonance imaging (MRI) findings.
This cross-sectional study of 185 purposively sampled patients with complaints of neck and back pains was carried out at Radiological facilities in Rivers State, Nigeria from February 2020 to November 2020. The inclusion criteria include patients with properly filled request forms and clinical indications. The patients were informed about the purpose of this study and their consent was duly sought and obtained. The nature of their participation was entirely voluntary. Ethical approval (UPTH/ADM/90/SII/VOL.XL/897) was obtained from the Human Research and Ethic committee of University of Port Harcourt Teaching Hospital, River State, Nigeria. Permission for this study was also obtained from the study centers. A total sample size of 185 patients included in this study was derived from the formula of unknown population given below
n = Zα2pq
d2
Where,
n = Expected sample size
Zα = significant level usually set at 95% confidence level, Zα is 1.96 (two sided).
p = proportion of the population with similar attributes under study = 50% (0.5).
d = Margin of error tolerated or absolute error = 7.2% (0.072)
q = 1-p = 1-0.5 = 0.5
n = (1.96)2 x 0.5 (1-0.5)/(0.072)2
n = 185
The purpose of the study was adequately explained to the participants and their consent was obtained. The voluntary nature of participation and their liberty to withdraw their informed consent were maintained. All retrieved data about the participants were treated with high level of confidentiality and used for the purpose of this study only. Only participants who were able to complete the quality of life questionnaires by themselves or with the help of others and had complete identification information were included in this study.
The spinal MRI investigations were performed using open type MRI machines (Brivo MR235, General Electric, and Siemens Magnetom C) with 0.35 Tesla using ( medium and large neck spine array volume coils) and (planar surface and multi-coil phased array) for cervical and lumbar spine respectively. The patients were examined lying supine with head and neck in a neutral position for cervical spine while the body in a neutral position for lumbar spine. The scanning parameters include: Fast spin-echo sequence was used to obtain T1 and T2 weighted images in axial and sagittal planes. Coronal images for T1W and T2W and Short Tau Inversion Recovery (STIR) sequences were also acquired for adequate assessment of the spine. The imaging parameters were: T1W sagittal image: TR/TE= 337-495/15-19, Field of view (FOV)= 240mm-260mm, slice thickness = 4-5mm, Flip angle = 900, matrix size = 206 x 256 and number of excitation (Nex)= 3-4, and T2W sagittal image: TR/TE = 3200-4700/110-125, FOV = 240-260mm, slice thickness = 4-5mm, Nex = 3-4 and Flip angle = 900. Axial image T2W: TR/TE= 2221-3400/120-125, FOV= 240 x 240mm, slice thickness =4-5mm, Nex= 3-4 and Flip angle = 900. The acquired images were interpreted by the researcher and two consultant radiologists with more than three years of experience in MRI spine reporting.
The patients were evaluated for degree of disabilities using the Nurick grading classifications:
0:Signs or symptoms of root involvement but without evidence of spinal cord disease.
1:Signs or symptoms of spinal cord disease but no difficulty in walking.
2:Slight difficulty in walking but does not prevent full-time employment.
3:Difficulty in walking which prevented full-time employment or ability to do all household work but which was not enough to require somebody's help to walk.
4:Able to walk only with someone else's help or with aid of a frame.
5:Chair bound or bedridden 7.
The assessment of the participant’s quality of life (QoL) was done using generic Short Form-36 (SF-36). The SF-36 is a comprehensive scale for the measurement of quality of life (non-health-related and health-related) through self-administered questionnaires and made up of 8 subscales consisting of Physical function (PF), Role function (RF), Bodily pain(BP), General health(GH), Vitality(VT), Social function (SF), Role emotion (RE) and Mental health (MH) 3, 8. Patients who indicated interest in participating in this study were ushered to a private seating area and were informed orally and in writing about the patterns of the study, and that their participation would involve filling out a questionnaire and providing answers to some questions. Each patient filled in the SF-36 questionnaire based on their quality of life as at the time of administering the questionnaire and interview. The Radiographers, Nurses and patient’s relatives who were involved in this study were adequately informed about the study and their consent and support were duly sought. Data such as gender, age group, spinal pathologies, degree of disabilities associated with spinal pathologies, and QoL outcome responses were collected using a data capture sheet and analyzed using descriptive statistics (mean standard deviation, tables, frequency, percentages and bar chart). Inferential statistics such as Kruskal-Wallis and Mann-Whitney U tests and data processing and analysis were done using Statistical Package for Social Sciences (SPSS) version 20(SPSS, Inc, Chicago, IL USA). A p-value <0.05 was considered statistically significant.
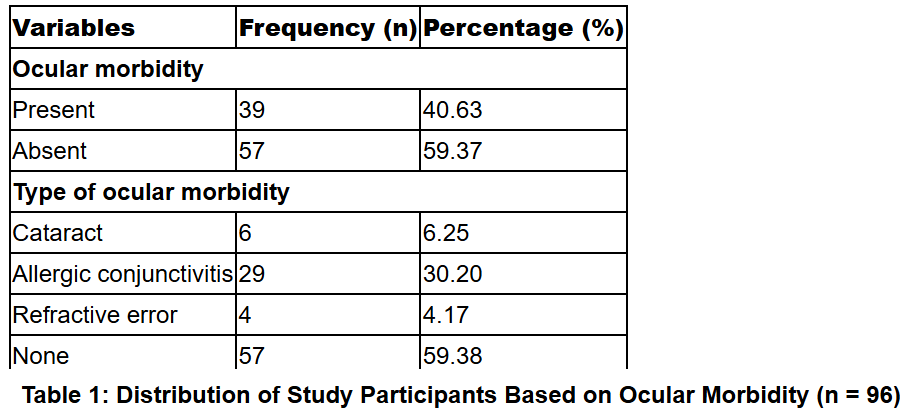
Out of 185 participants in this study, the greater number 58.9% (n= 109) had lumbar spine pathologies while those with cervical spine pathologies accounted for 40.1% (n=76). Most of the participants with cervical 64% (n= 49) and lumbar 79.8% (n= 86) spine pathologies were males. The majority of the participants were within the age range of 20-39 years 41 %(n=31) and 40-49 years 48.6% (n=53) for cervical and lumbar spine pathologies respectively (Table 1).
From Figure 1, most of the participants had degenerative spinal abnormalities, which were 75% (n=57) and 80.7% (n= 88) for cervical and lumbar spine regions respectively.
The results of the degree of disabilities associated with spinal pathologies in Figure 2, Figure 3 respectively, revealed that Nurick grade I 39.5% (n=30) was the most common among the participants with cervical spine pathologies while Nurick grade II 50.5% (n=56) was the most common score among individuals with lumbar spine pathologies. The lowest scores were Nurick grade IV 10.6% (n=5) and Nurick grade 0 1.8% (n=2) in individuals with cervical and lumbar spine pathologies respectively (Figure 2, Figure 3).
The QoL scores of the participants with different age groups were evaluated and the results revealed that in the physical functioning domain, age group < 20years and ≥ 60 years had the highest (155.50) and lowest (117.63) mean rank scores respectively. In the physical component summary, < 20 years and ≥ 60 years had the highest (169.67) and lowest (115.72) mean rank scores respectively, while in the mental component summary, ≥ 60 years and < 20 years had the highest (130.40) and lowest (111.94) mean rank scores. There was no significant difference in the QoL domains, components and total QoL in participants with different age group (p > 0.05) (Table 2).
The results of Kruskal-Wall’s test mean rank values for some of the QoL domains in the participants with different Nurick grade scales and their level of statistical significance were; PF (0=121.74, I=141.66, II=113.15, III=109.57, IV=92.28, V= 123.40, k=12.27 and p=0.03), VT(0=128.52, I=117.02, II=112.75, III= 128.77, IV=148.92, V= 146.70, k = 5.67 and p= 0.034) and SF(0=118.09, I= 122.24, II= 121.93, III=130.03, IV = 94.81, V= 151.60, k= 4.30 and p=0.51). There were statistically significant differences in the physical functioning domain (k=12.27, p = 0.03), total quality of life (k= 11.63, p = 0.04) and role limitations due to emotional problem domain (k= 13.03, p = 0.02) among participants with different Nurick grade scales. Participants with Nurick grade scales of 0(132.65) and IV (71.61) had significantly highest and lowest mean rank scores in the physical component summary with significant differences (k= 12.75, p= 0.03) [Table 3].
The differences in the QoL of the participants with different durations of pathology was evaluated and the results, showed that in the physical functioning domain, those with < 6 months and 1-2years durations had the highest (123.67) and lowest (107.94) mean rank scores respectively. There was no significant difference in the QoL of the participants with different durations of pathology in the physical functioning domain (k= 1.18 and p = 0.76). Participants with 6 months to 1 year and 2-3years durations of pathology had the highest (130.02) and lowest (88.96) mean rank scores respectively in the physical component summary, and there was no statistically significant difference in the QoL of the participants with different durations of pathology in the physical summary component (k= 7.81 and p = 0.06). Generally, there was no statistically significant difference in any of the QoL domains, components and total QoL among the participants with different duration of pathologies (p > 0.05)(Table 4).
|
Demographic variables |
Regions of the spinal |
Total |
|
|
Cervical n (%) |
Lumber n (%) |
|
|
|
Gender |
|
|
|
|
Male |
49 (64%) |
86 (79.8) |
135 (73.5%) |
|
Female |
27 (36%) |
22 (20.2) |
50 (26.5%) |
|
Total |
76 (100%) |
109 (100) |
185(100%) |
|
Age group |
|
|
|
|
< 20 |
12 (16%) |
610(9.2) |
22(25.2%) |
|
20 – 39 |
31(41%) |
27(24.8) |
58(65.8%) |
|
40 – 59 |
18(21%) |
53 (48.6) |
71(70.6%) |
|
60 years and above |
15(19%) |
18(17.4) |
33(36.4%) |
|
Total |
76(100%) |
109(100%) |
185(100) |



|
Quality of life scores |
Class |
Mean Rank |
K |
P |
|
Physical functioning Domain |
<20 years |
155.50 |
2.58 |
0.46 |
|
20-39 years |
123.45 |
|
|
|
|
40-59 years |
118.38 |
|
|
|
|
≥60 years |
117.63 |
|
|
|
|
Role limitation due to Physical health |
<20 years |
125.83 |
2.41 |
0.49 |
|
20-39 years |
128.45 |
|
|
|
|
40-59 years |
114.39 |
|
|
|
|
≥60 years |
125.56 |
|
|
|
|
Mental health |
<20 years |
109.50 |
1.94 |
0.59 |
|
20-39 years |
120.10 |
|
|
|
|
40-59 years |
119.45 |
|
|
|
|
≥60 years |
134.97 |
|
|
|
|
Vitality |
<20 years |
139.83 |
2.60 |
0.46 |
|
20-39 years |
126.99 |
|
|
|
|
40-59 years |
114.13 |
|
|
|
|
≥60 years |
126.51 |
|
|
|
|
Role limitation due to Emotional Problem |
<20 years |
114.22 |
2.42 |
0.49 |
|
20-39 years |
126.99 |
|
|
|
|
40-59 years |
115.09 |
|
|
|
|
≥60 years |
133.87 |
|
|
|
|
Social functioning |
<20 years |
117.50 |
0.85 |
0.84 |
|
20-39 years |
126.60 |
|
|
|
|
40-59 years |
117.69 |
|
|
|
|
≥60 years |
121.79 |
|
|
|
|
Pain |
<20 years |
170.44 |
6.44 |
0.09 |
|
20-39 years |
120.86 |
|
|
|
|
40-59 years |
122.51 |
|
|
|
|
≥60 years |
106.90 |
|
|
|
|
General health |
<20 years |
139.00 |
1.67 |
0.64 |
|
20-39 years |
114.79 |
|
|
|
|
40-59 years |
124.68 |
|
|
|
|
≥60 years |
123.84 |
|
|
|
|
Physical component Summary score |
<20 years |
169.67 |
4.77 |
0.19 |
|
20-39 years |
122.93 |
|
|
|
|
40-59 years |
118.23 |
|
|
|
|
≥60 years |
115.72 |
|
|
|
|
Mental component Summary score |
<20 years |
111.94 |
3.49 |
0.32 |
|
20-39 years |
129.60 |
|
|
|
|
40-59 years |
113.13 |
|
|
|
|
≥60 years |
130.40 |
|
|
|
|
Total quality of life |
<20 years |
156.56 |
5.29 |
0.15 |
|
|
20-39 years |
127.24 |
|
|
|
|
40-59 years |
111.91 |
|
|
|
|
≥60 years |
128.66 |
|
|
Most of the participants with either cervical or lumbar spine pathologies in this study were males. This finding is in harmony with the findings of the studies conducted by Dallbayrak et al 9; Harkema et al 10; Laxton and Perrin 11, Maaji et al 12; Motter et al 13; Mustapha et al 5, Olarinye-Akorede et al 6; RoseBist et al 14, Ogolodom et al 15, which also reported more males than their female counterparts. The male preponderance identified in this study could be ascribed to the fact that males constituted the greater proportion of the workforce in most societies and are mostly exposed to strenuous jobs, which predisposes them to spinal pathologies 15. Contrary to our finding, Babinska et al 16, Miyagishima et al 17, Nikjooy et al 18 and Shalaby et al 19, reported high female preponderance. The differences identified in the finding of this study and that of the previous researchers, could be attributed to the different sample sizes studied, the nature and purposes of the various studies.
The age group commonly affected with spinal pathologies was evaluated and the results revealed that majority of the individuals with cervical spine pathologies were mostly found within the age group of 20-39 years while those with lumbar spine pathologies were more in the age group of 40-59 years. This finding is in agreement with the findings of the studies conducted by Ogolodom et al 15. Our findings could be ascribed to the fact that people in these age range are the most active parts of every society and are usually involved in vigorous jobs and social activities that often dispose them to spinal pathologies.
Most of the participants with cervical spine pathologies had Nurick grade I, which implies that they had signs or symptoms of spinal cord disease but no difficulty in walking. Among those with cervical spine pathologies, the least had Nurick grade IV, in which they were able to walk with the aid of someone or frame. This finding is in consonance with the finding of the study carried out by Ogolodom et al 15, but not in agreement with the findings of the studies conducted by Olarinye-Akorede et al 6 and RoseBist et al 14. Nurick grades III and IV scores were reported in the study conducted by Olarinye-Akorede 6. In RoseBist et al 14 study, which was carried out to determine the clinical and radiological correlation of cervical spondylosis, reported Nurick grade II [43%) to be highest followed by Nurick grade I (35%), and the least was Nurick grade III (15%). The differences in our findings could be attributed to the different sample sizes employed in the various studies as well as the nature of the various studies. The majority of the patients in our study with lumbar spine pathologies had Nurick grade II, which means that they had slight difficulty in walking but they were not prevented from full employment. This result is in keeping with the findings of a research work conducted by Ogolodom et al 15, which also reported Nurick II to be more common among individuals with cervical spine pathologies.
The QoL scores of the participants with different age group was evaluated and the results, revealed that there was no significance difference in the QoL domains, components and total QoL in participants with different age group, meaning that all the different age groups have similar quality of life scores across the various domains, components scores and in their total quality of life outcomes. Nevertheless, those within the age group < 20 years had the highest role limitations due to physical functioning while those within the age group ≥ 60 years had the least role limitations due to physical functioning. This could be attributed to the fact that people within the age bracket of ≥ 60 years are usually highly experienced and can also adapt easily to health challenges when compared to the younger ones.
The results of the QoL scores in the participants with different degrees of disability revealed that, there were statistical significances in the role limitations due to physical functioning, emotional problem, as well as in the total quality of life among participants with different degree of disabilities. This implies that participants role limitations due to physical function, emotional problems and their overall QoL scores, were not same across the different Nurick grade scales. In physical functioning domain, those with Nurick grade I (participants with signs or symptoms of spinal cord disease without difficulty in walking) class were highly limited in their physical functioning when compared to those with Nurick grade IV class. The loss of somatic and autonomic control, which is associated with spinal cord disease, results in a reduction of physical activity and blunted cardiovascular response to exercise 20. The consequences of this reduction in physical activity are significant physical deconditioning, altered body composition, and development of detrimental metabolic profiles leading to poorer health outcomes in this population 20. According to Ditor and Hicks21, physical activity programs and information about how activity can promote health are two of the services most desired but least available to people with spinal cord disease.
The differences in the QoL of the participants with different durations of pathology was evaluated and the results showed there was no statistically significance difference in any of the QoL domains, components and total QoL among the participants with different duration of pathologies. This implies that the quality-of-life scores across the different domains, components and the overall QoL are same among individual with different duration of pathology. However, in the physical functioning domain, those that had < 6 months duration of pathology had the highest role limitations due to physical functioning. This could be attributed to the fact that these categories of persons were still yet to be adapted with the pathological conditions.
This study demonstrated that males are commonly affected with either cervical or lumbar spine pathologies. Functional grading of patients with either cervical or lumbar spine pathologies revealed that most patients with cervical spine pathologies have Nurick grade I while Nurick grade II pathologies are more prevalent among patients with lumbar spine pathologies. QoL outcome is independent of age group and duration of the different pathologies. Role limitations due to physical functioning, emotional problem, as well as total quality of life differ and depend on the different Nurick grade scales.
None declared among the authors
Nil
Subscribe now for latest articles and news.