Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i02.009
Year: 2020, Volume: 6, Issue: 2, Pages: 46-49
Original Article
D Abhijith1, M D Nandini1, B G Vittal2
1Tutor, Department of Biochemistry, Hassan Institute of Medical Sciences, Hassan, Karnataka, India, 2Professor and Head, Department of Biochemistry, Hassan Institute of Medical Sciences, Hassan, Karnataka, India
Address for correspondence:
Dr. B.G. Vittal, Department of Biochemistry, Hassan Institute of Medical Sciences, Hassan, Karnataka, India.
Phone: +91-8904595910. E-mail: [email protected]
Objective: The objective of the study was to assess the usefulness of ethylenediaminetetraacetic acid (EDTA) plasma as an alternative to serum for glucose, renal function test, and liver function test.
Need for the Study:The use of plasma as compared to serum decreases the turnaround time, coagulation- induced interferences, gives high sample volume for analysis, and is economical.
Methodology An observational cross-sectional study was done on blood samples of 51 patients. A 4 ml of blood was drawn from each patient by standard venipuncture technique. A 2 ml was collected in a plain red top Vacutainer and 2 ml in an EDTA Vacutainer. Red top tubes, after 20 min of clotting, were centrifuged for 5 min at 5000 rpm to separate serum. EDTA tubes were centrifuged immediately at 5000 rpm to separate plasma. Serum and plasma were analyzed with ERBA-EM-360 autoanalyzer for glucose, urea, creatinine, total bilirubin, direct bilirubin, total protein, albumin, aspartate transaminase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP). Results obtained were analyzed using paired “t-test.”
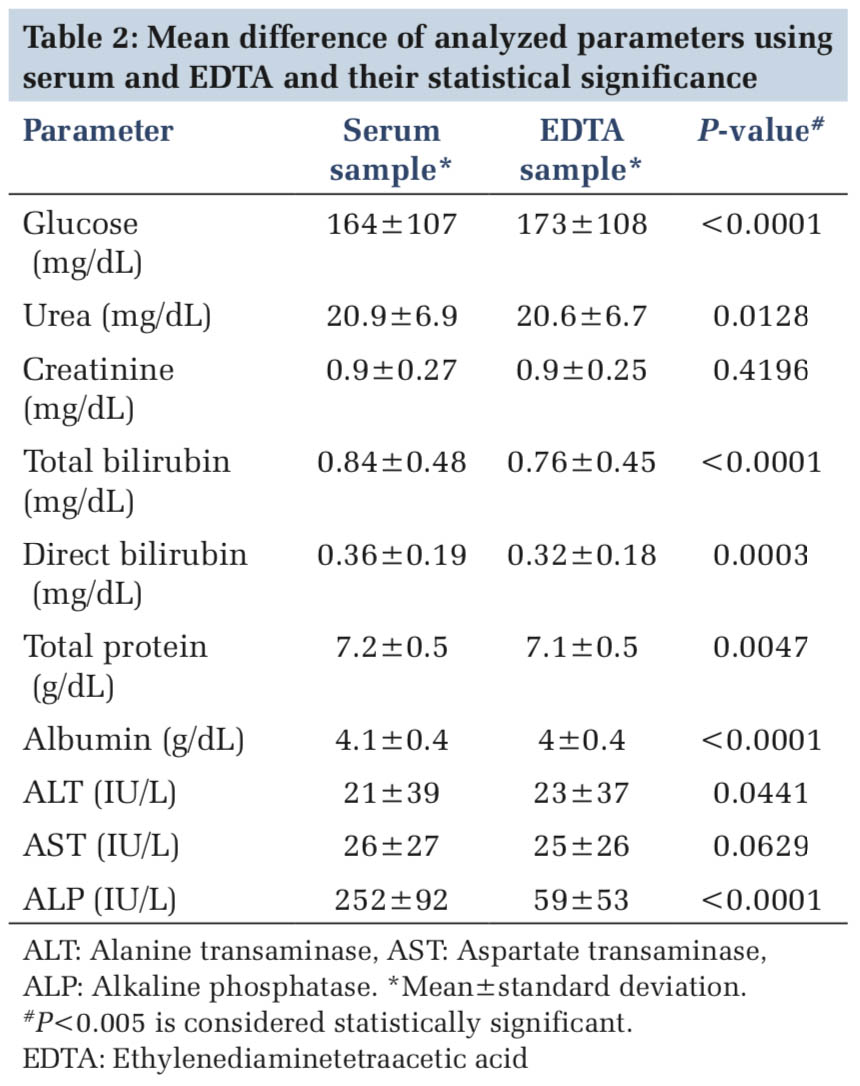
Results: Values of glucose, urea, total bilirubin, direct bilirubin, total protein, albumin, and ALP in serum and plasma samples showed statistically significant difference with P < 0.05. Plasma glucose was more as compared to serum glucose. Creatinine, AST, and ALT values in serum and plasma samples showed statistically no significant difference with P > 0.05.
Conclusion:EDTA plasma can be used as an alternative to serum for creatinine, AST, and ALT but its use for urea, total bilirubin, direct bilirubin, total protein, albumin, and for ALP may not be appropriate.
KEY WORDS:Biochemical assay, ethylenediaminetetraacetic acid, liver function tests, plasma, renal function
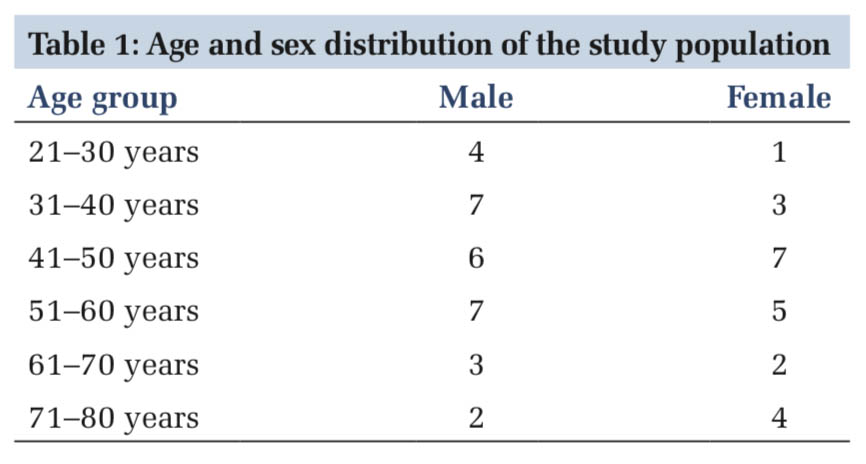
IntroductionSerum is the specimen preferred for estimating the biochemical parameters by most of the laboratories. Serum is the liquid portion of the blood obtained after the blood has clotted completely. The Association of Physicians of India and American Diabetes Association (ADA) guidelines use plasma glucose for diagnosis of diabetes mellitus. Plasma is the cell-free supernatant layer obtained after centrifugation of the anticoagulated blood. Anticoagulants are the substances/compounds MethodologyAn observational cross-sectional study was done on blood samples of 51 patients attending central laboratory of HIMS Teaching Hospital, Hassan. Patient selection was based on sampling of convenience, so patients were chosen irrespective of their clinical condition. Institutional Ethics Committee approval was obtained and consent of participants was obtained. A 4 ml of blood was drawn from each patient by standard venipuncture technique out of which 2 ml was collected in a plain red top Vacutainer and the other 2 ml in an EDTA purple top Vacutainer. Blood in red top tubes, after 20 min of clotting, were centrifuged for 5 min at 5000 rpm to separate serum. Blood in the EDTA tubes were centrifuged immediately at 5000 rpm to separate the plasma. Serum and plasma after separation were analyzed with ERBA EM 360 autoanalyzer using ERBA reagents for glucose (glucose oxidase- peroxidase method), urea (urease UV kinetic glutamate dehydrogenase method), creatinine (modified Jaffe’s endpoint method), total bilirubin (Evelyn-Malloy’s modified diazo method), direct bilirubin, total protein (biuret method), albumin (bromocresol green method), AST (IFCC-Kinetic method), ALT (IFCC-Kinetic method), and ALP (p-Nitrophenyl phosphate AMP kinetic method). Routine quality control procedures were in place during the study. Results obtained were analyzed using paired “t-test” with SPSS statistical software. Paired “t-test” was used, as plasma is a substance obtained after adding an anticoagulant to serum. Results before and after addition of anticoagulant are compared using paired “t-test.” ResultsThe study group comprised 51 patients of whom 22 were male and 29 were female of age groups, as shown in Table 1. DiscussionThis study showed statistically significant difference in values between serum and EDTA plasma for urea, total bilirubin, direct bilirubin, total protein, albumin ALT, and ALP, thereby confronting the postulated hypothesis of use of EDTA plasma as a replacement for serum with respect to the above parameters.
|
ConclusionEDTA plasma can be used as an alternative to serum for creatinine, AST, and ALT but its use for urea, total bilirubin, direct bilirubin, total protein, albumin, and for ALP may not be appropriate as per our study. Estimation of glucose in plasma will ensure that diabetes mellitus is not underdiagnosed, as plasma glucose levels are higher than serum glucose. |
Subscribe now for latest articles and news.