Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i02.003
Year: 2016, Volume: 2, Issue: 2, Pages: 13-18
Original Article
Filiz Bayar1, R Erkal Ozkan1, Dilek Tas2
1Dr, Department of Infectious Diseases and Clinical Microbiology, Usak State Hospital, Usak, Turkey,
2Nurse, Department of Infectious Diseases and Clinical Microbiology, Infection Control Committee Infectious, Usak State Hospital, Usak, Turkey
Address for correspondence:
Filiz Bayar, Infectious Diseases and Clinical Microbiology, Usak State Hospital, Usak, Turkey. Phone: +905057123235. E-mail: drfiizsurucu(S)hotmail.com
Objectives and Aims: The sharp object injury and occupational exposures to blood and body fluids have kept to be a serious problem for the healthcare personnel (HCP), especially in the developing countries. The aim of this study was to evaluate the occupational exposures to blood and body fluids among HCP in Usak State Hospital and determine the measures for reduction of occupational exposures.
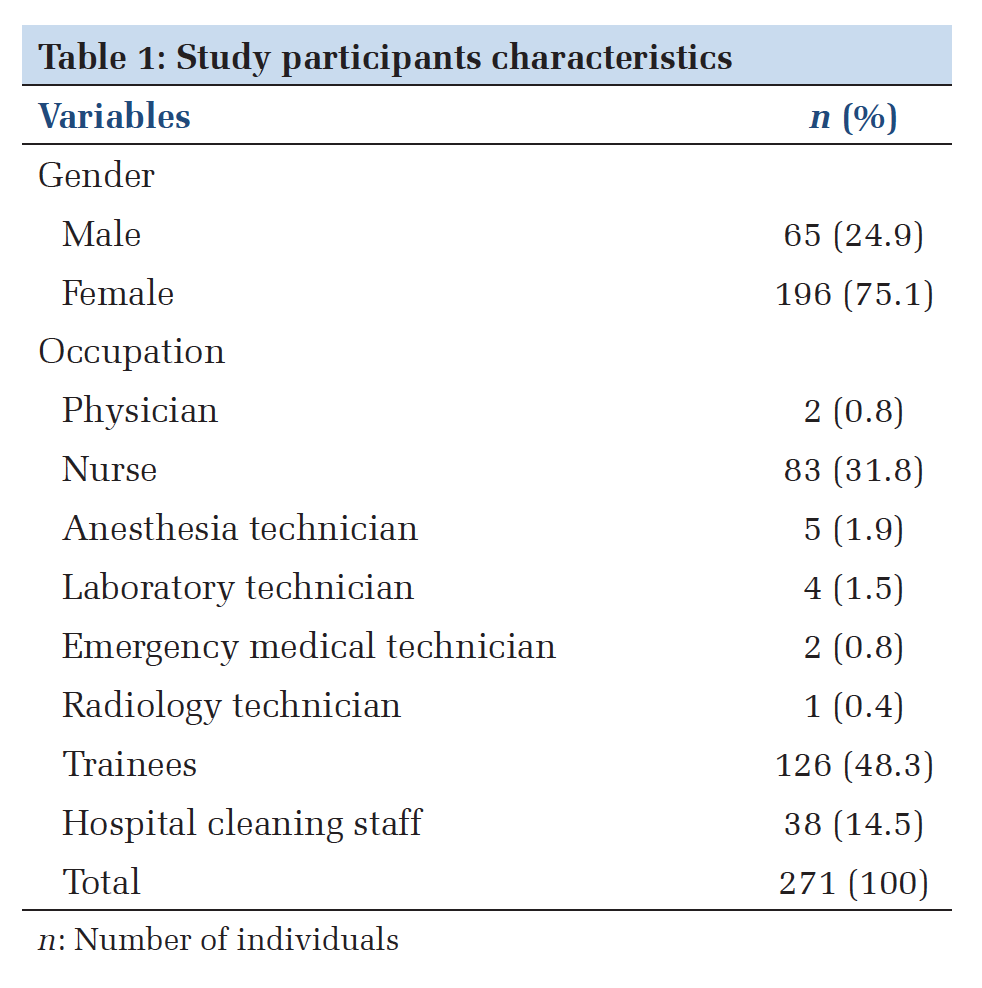
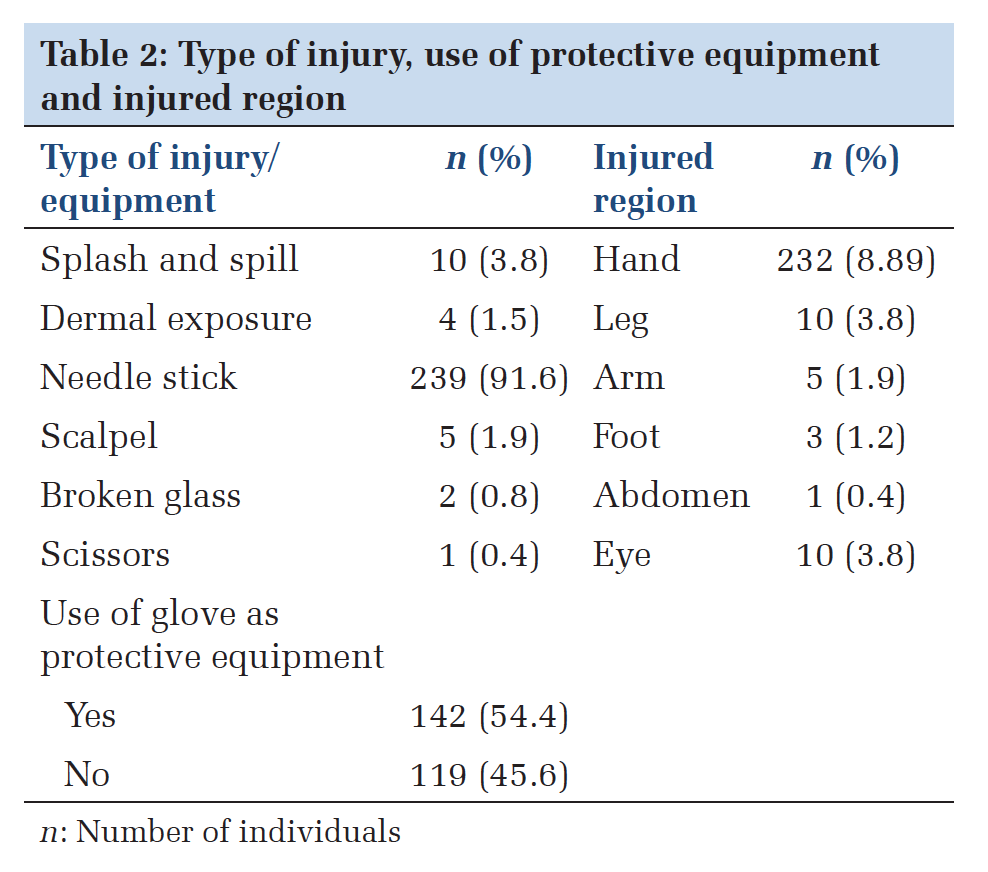
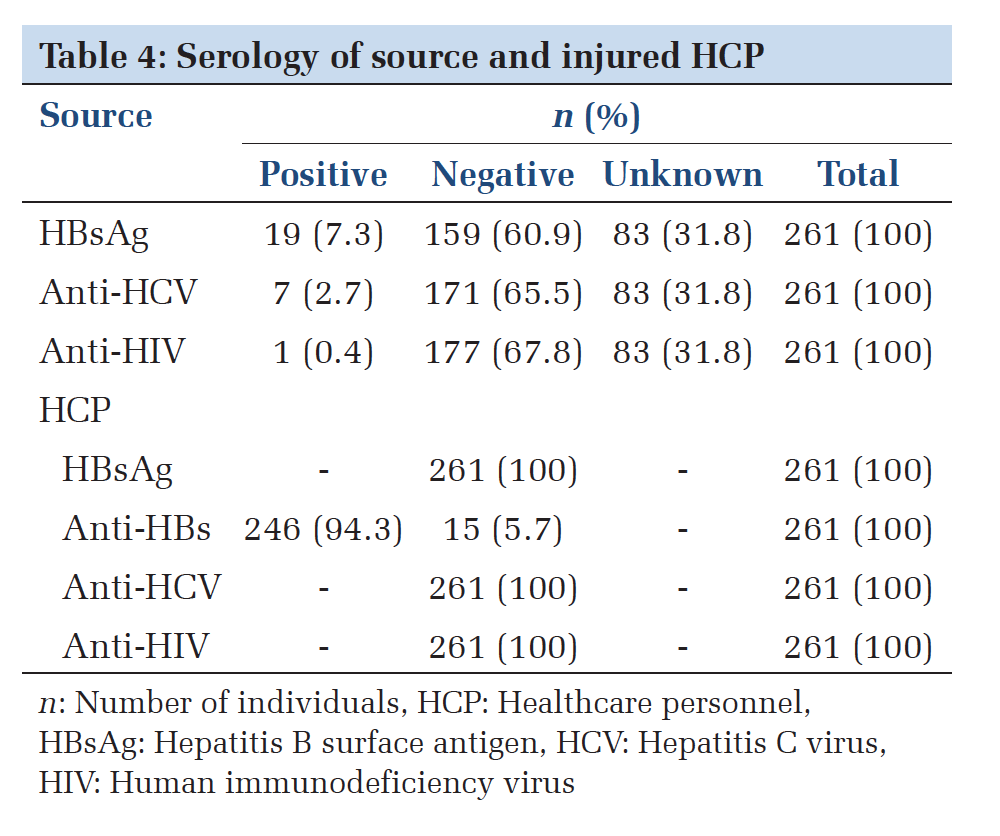
Materials and Methods: We evaluated 261 cases of occupational exposures to blood and body fluids among HCP during the period July 2011-October 2015 in Usak State Hospital by examining the records of Infection Control Committee (ICC). Results: Total 261 HCP applied to ICC for the occupational exposures to blood and body fluids, and 196 (75.1%) persons of them were women, while 65 (24.9%) persons of them were men. The trainees were the occupational group which was mostly exposed to blood and body fluids with 48.3% among occupational groups, while the most cases of occupational exposures to blood and body fluids were reported by internal medical units with 31.0%. Most of the injuries (94.6%) were percutaneous, and the needlestick injury was the type of incident most frequently reported by HCP (91.6%). Nearly half of the HCP (54.4%) exposed to blood and body fluids reported that they wore gloves during the injuries, and the sources were known in 68.2% of all cases. Hepatitis B (HB) surface antigen was found to be positive in 10.7% of these patients; hepatitis C virus (HCV) was found to be positive in 3.9% of the patients; and anti-human immunodeficiency virus (HIV) was found to be positive in 0.6% of the patients. On the other hand, anti-HBs was found to be positive in 94.3 of the HCP, but none of the anti-HCV and anti-HIV positiveness were found after the exposure. 15 (5.7%) HCP with negative anti-HBs were included in vaccine program, and antiretroviral prophylaxis was applied to one HCP, which contacted with a person having positive anti-HIV. No seroconversion was detected in the HCP after a 6 month-regular screenings.
Conclusions: Occupational exposures to blood and body fluids have still been a serious problem for HCP. All the HCP and trainees should be trained about the occupational exposure, protection, and post-exposure procedures regularly to decrease the frequency of occupational exposures to blood and body fluids.
KEY WORDS:Occupational exposures, safeguard measures, healthcare personnel.
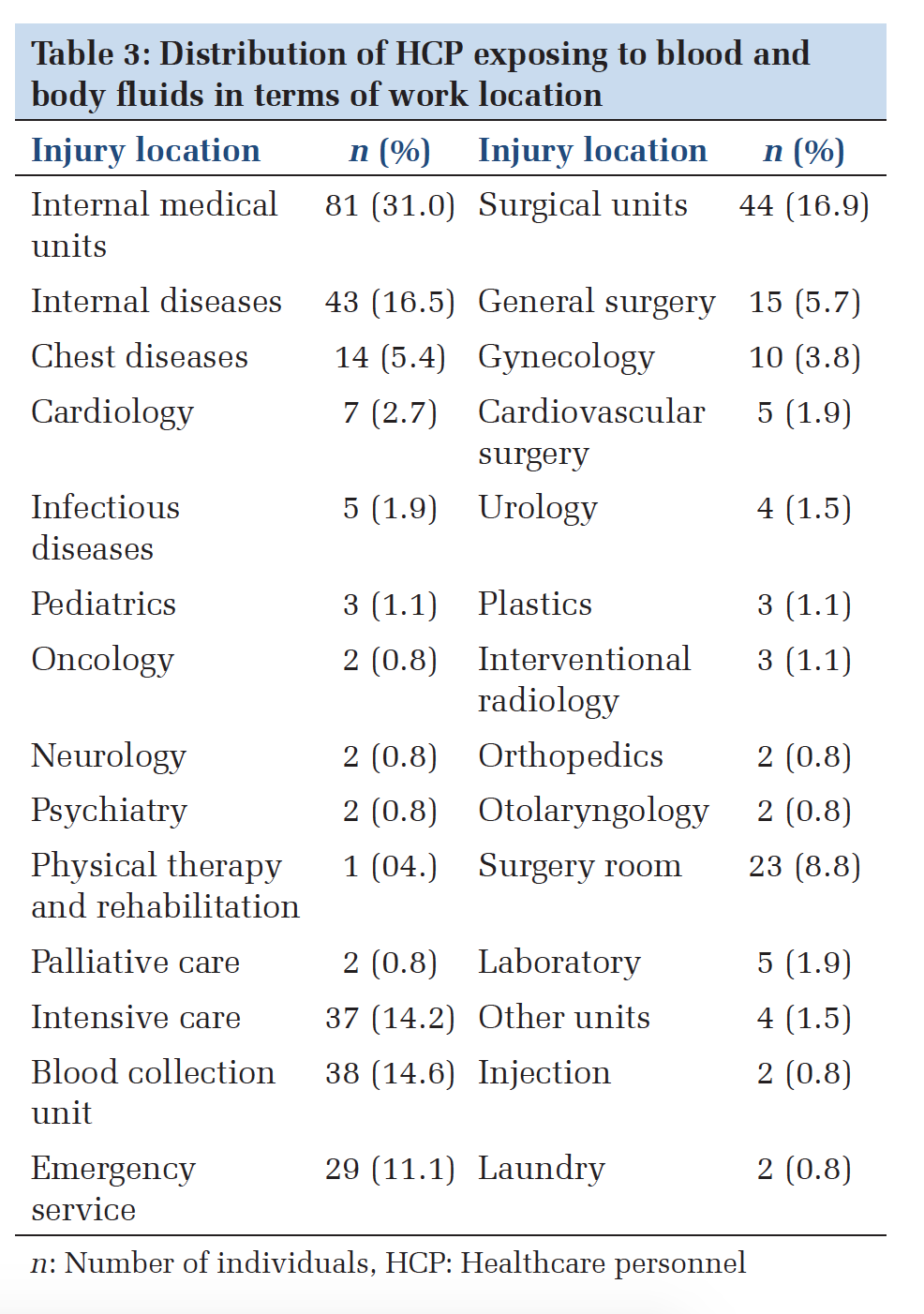
IntroductionThe exposure to the blood-borne pathogens poses a serious risk for the healthcare personnel (HCP). These pathogens are generally transmitted to the HCP by percutaneous or mucosal contact with the blood and body fluids of the infected patients. The transmission of the pathogens may happen by the injuries with a needle and other sharp objects, direct inoculation of the viruses through bruise skin, stretch marks, and lesions or splash to the mucosal areas such as eye, nose, and mouth.[1,2] At least 20 pathogens transmitted by sharp object injuries (SOIs) have been reported, and the crucial ones from these pathogens carrying transmission risk are hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV).[2] The World Health Organization projected that 3 million persons out of 35 million persons were exposed to blood-borne pathogens through the injuries in every year in the world. About 66000 HBV, 16000 HCV, and 200-5000 HIV infections are expected to emerge among HCP in every year as a result of these injuries.[3] The HIV contamination risk after needlestick contaminated by blood infected with HIV and mucosa exposure is, respectively, 0.3% and 0.09%. HBV infection risk after only one parenteral exposure to the patient with positive hepatitis B surface antigen (HbsAg) is 6% if Hepatitis B e-antigen (HBeAg) is negative and may reach 40% if HBeAg is positive. HCV seroconversion incidence after injury from a positive HCV source is on average 1.8% (0-7%).[4] The evaluation and treatment of this kind of incidents cause financial burden and workforce loss. This kind of exposure also affects the life quality of the HCP and leads anxiety for their family and colleagues.[5,6] Furthermore, occupational hazard affects not only HCP but also the quality medical service.[7] The aim of this study is to analyze the SOIs and the occupational exposures to blood and body fluids among HCP of Usak State Hospital during the period July 2011-October 2015 and determine the measures for reduction of occupational exposures. Materials and MethodsIn this study, we examined the SOIs and mucosal exposures of infected blood and body fluids among the HCP during the period July 2011-October 2015 in Usak State Hospital. Total 261 HCP applied to the ICC for this kind of injury, and no HCPs had experienced repeated occupational exposures. The Usak State Hospital has inpatient bed availability for 800 persons and has 1140 HCP except administrative personnel, 274 hospital cleaning staff, and 845 trainees as of December 2015. We examined the forms retrospectively filled by the HCP, which applied to the ICC after the injury or occupational exposures to blood and body fluids. These forms include demographic information, occupational group, working unit of HCP, type of equipment causing the injury, time of injury, use of protective equipment during occupational exposure, serology of HCP and patient and follow-up information. First, we tested the normality by Kolmogorov–Smirnov and Shapiro–Wilk tests and found that they did not exhibit a normal distribution. Therefore, we used Kruskal–Wallis test, which is a non-parametric method, for the evaluation of group differences. We used Pearson Chi-square test because our data is categorical. We choose 99% as confidence interval in the study and benefited from SPSS 20.0 software package for the statistical analysis. ResultsTotal 261 HCP applied to the ICC for the SOIs and occupational exposures to blood and body fluids. 196 (75.1%) of the 261 HCP were women, and 65 (24.9%) of them were men. The trainees including students from a medical career college and high school of nursing were the occupational group which was mostly exposed to blood and body fluids with 48.3% among occupational groups; then, nurses applied to the ICC for this kind of injury with 31.8%. On the other hand, hospital cleaning staff, allied health personnel including anesthesia technician, laboratory technician, emergency medical technician, radiology technician, and physicians were relatively less exposed to the sharp object injuries and occupational exposures to blood and body fluids and the share of these occupational groups as a percentage of 261 applications, respectively, were 14.5%, 4.6%, and 0.8% (Table 1). 94.7% of all the reported injuries were percutaneous. The tools causing percutaneous injuries were needlestick with 91.6%, scalpel with 1.9%, broken glass with 0.8%, and scissors with 0.4%. The contaminated body parts and their ration as a percent of 261 cases, respectively, were hand with 88.9%, leg with 3.8%, eye with 3.8%, arm with 1.9%, foot with 1.2%, and abdomen with 0.4%. We found that all the injured HCP wore work uniforms such as apron and forma as protective equipment but only 54.4% of the injured HCP pulled on gloves (Table 2). We also analyzed the relationship among the use of glove as protective equipment, gender, time of injury, type of occupation, and working service and found that women were more effective in the use of gloves as protective equipment relative to the men (P = 0.000). On the other hand, protective equipment were found to be used more within working hours relative to off-hours (P = 0.026). Laboratory technicians, emergency medical technicians, and anesthesia technicians were the occupational groups which used the protective equipment mostly among the HCP, while physicians, nurses, and trainees were the occupational groups which used the protective equipment least (P = 0.017). Finally, we found that protective equipment were used mostly in surgery rooms and services of oncology and gynecology, while protective equipment were used least in the services of orthopedics, neurology, and otorhinolaryngology (P = 0.000). The internal medical units were in the lead with 31.0% among the clinics which reported the cases of SOIs, and occupational exposures to blood and body fluids were followed by surgical units with 16.9%, blood collection unit with 14.6%, and intensive care units with 14.2% (Table 3). The source was known in 68.2% of all the cases. HBsAg was found to be positive in 10.7%; anti- HCV was found to be positive in 3.9%, and anti- HIV was found to be positive in 0.6% of these patients. On the other hand, anti-HBs was positive in 94.3% of the injured HCP, but no positiveness of anti-HCV and anti-HIV were seen (Table 4). All the personnel contacted with the source having positive HbsAg were immune to HBV. 15 (5.7%) HCP with negative anti-HBS were subjected to the vaccine program. On the other hand, antiretroviral (tenofovir+emtrisitabin) prophylaxis was applied to one HCP contacted with a source having positive anti-HIV during a 4-week period. Furthermore, 7 HCP having contact with positive anti-HCV source were taken under review, and no positiveness of HBsAg, anti-HCV, and anti-HIV were detected in any HCP after 6 months follow-up. DiscussionThe mucosal contact with blood and body fluids and SOIs pose an important source of risk for HCP. 2.5% of HIV cases and 40% of hepatitis B and C cases among HCP in the world emerge due to occupational exposures.[8] We conduct medical inspections of HBsAg, anti-HBS, anti-HCV, and anti-HIV for the new hired HCPs, and the non-immunited HCPs are included hepatitis B vaccination. Furthermore, training about blood and body fluid-borne infections and safeguard measures is given to the new hired HCPs during orientation training, and this training is done again a year. In this study, 261 HCP applied to the ICC owing to SOIs and occupational exposures to blood and body fluids. 79% of all the HCP in Turkey experiences an SOI, at least, one time during their working life.[9] Furthermore, the nurses have been found to be the occupational group which is most exposed to injuries by extensive studies in the literature.[5,6,10-12] However, some studies also have found that hospital cleaning staff is the occupational group which is the most frequently exposed to the SOIs and occupational exposures to blood and body fluids.[13,14] We found that trainees were mostly exposed to the SOIs and occupational exposures to blood and body fluids as distinct from the literature. 845 students undergo training in the Usak State Hospital as of December 2015, although their number varies depending on the school periods. The high injury ratio among the trainees may be arisen from a higher number of trainees relative to the other occupational groups, being inexperienced and educational problems. Furthermore, we think that the trainees implement invasive procedures such as blood collection, establishing vascular access, injection, and measurement of blood sugar in the services more. Finally, the occupational group with lowest injury ratio was physicians with 0.8%. Following the protective measures and statements of these kinds of cases still have stayed at insufficient levels, although there have been extensive written procedures and handbooks about the SOIs and occupational exposures to blood and body fluids. One study in the literature suggests that only 14% of occupational exposures apply for prophylaxis and follow-up visits.[15] We think that HCP, especially the physicians, do not report the occupational exposures which they evaluate riskless. In another study, the physicians did not regard the relevant training among the occupational groups, and 20% of the physicians did not participate to the training.[16] Therefore, we think that the low ratio of occupational exposures among the physicians may be arisen from their not giving statement about the exposures considering the relevant findings in the literature. On the other hand, all physicians who reported the occupational exposures were from surgical units and our this result is consistent with the results of the other studies in the literature.[11,15,17] The most cases of SOIs and occupational exposures were seen in the internal medical units, and also, there have been some studies which reached the same result in the literature.[11,18] However, many studies found that there have been relatively more SOIs and occupational exposures in the surgical services,[9,10,19-21] and this result was explained by more uses of sharp objects and more direct contacts with the patients in the surgical services. Use of disposable medical supplies and blood collection by vacuum tubes and throw of sharp objects into the solid boxes contribute to the significant decreases in the SOIs. However, cases of SOIs have been experienced frequently despite to these countermeasures and needlestick has still the most common tool causing the injuries. We found that the most of the injuries in our study were caused by needlestick similarly with the results in the literature.[5,9,10,16,18,19,21] Use of gloves by the HCP, which has been exposed to blood and body fluids changes between 52% and 75.7% according to the studies in the literature.[11-13,17-19,22] We found that the ratio of glove usage by the injured HCP was 54.4%. This finding shows that the HCP should be more sensitive about obeying the standard measures. Taking the protective measures will decrease the risk of bloodborne infection by preventing the contact with blood and body. The standard measures were suggested by Centers for Disease Control and Prevention in 1982, and a new guidebook about occupational exposures was issued in the coming years. In this regard, obeying the standard measures should be required by considering all the patients and blood samples being infected.[23] The patient on which was used the material causing the injury was unknown in the 29-46.7% of the percutaneous injuries.[10-12,17,20] In our study, the ratio of injury by the material with the unknown source was about same with results of the relevant studies in the literature. The ratio of HBV carriers in Turkey is between 2% and 10% and is located among intermediate endemicity regions. This ratio is 1.5-2 times more among the HCP.[24] In this case, vaccination of the HCP, a risky group in terms of occupational exposure, exhibits importance. 5.7% of the injured HCP was found to be negative, and no positiveness of HbsAg was detected in this study. No prophylaxis against HBV was required, or no HCP was required to be treated after contact with HBV carrier source. Transmission rates of HIV and HCV are low, and the injured HCP should be monitored. Taking and the following standard is important because it is not possible to protect against the prevention of transmission by the vaccine. It is projected that 0.5% of the HCP meets with HIV as a result of occupational exposure and 1000 new HIV infections emerge in every year in the world.[25] The seroprevalence of HCV is about 0.5-2% in the world, while the seroprevalence of HCV is about 1.6% in HCP and 0.3-0.5% in blood donors.[26] In this study, 7 HCP which contacted with positive anti-HCV source were monitored during 6 months. Furthermore, antiretroviral prophylaxis was applied to one HCP having contact with positive anti-HIV source during the 4-week period, and no positiveness of HbsAg, anti-HCV, and anti-HIV were detected during the follow-ups.
|
ConclusionWe examined 261 cases of occupational exposures to blood and body fluids among HCP during the period July 2011-October 2015 in the Usak State Hospital. The results indicated that the occupational exposures to blood and body fluids have still been a serious problem for the HCP. However, it is seen that there have been the existence of unvaccinated HCP, insufficient usage level of protective equipment, and low statement level by the physicians with SOIs or exposed to blood and body fluids. All the HCP and trainees should be trained regularly about nosocomial infections, standard procedures, blood-borne infections, statement of the injury, and prophylaxis post injury to reduce the level of occupational exposure. |
Subscribe now for latest articles and news.