Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.011
Year: 2021, Volume: 7, Issue: 3, Pages: 51-58
Original Article
Burcu Gultekin1 , Seckin Tuncer2 , Ilksen Burat3
1Faculty Department of Histology and Embryology, Necmettin Erbakan University Meram Medical, Konya, Turkey,
2Medical Faculty Department of Biophysics, Eskisehir Osmangazi University, Eskisehir, Turkey, 3The Scientific and Technological Research Council of Turkey, Space Technologies Research Institute (TUBITAK-UZAY), Ankara, Turkey
Address for correspondence:
Seckin Tuncer, Medical Faculty Department of Biophysics, Eskisehir Osmangazi University, Eskisehir, Turkey. E-mail: [email protected]
Background: Local and systemic effects of ischemia reperfusion are an important problem in vascular surgery. Acute ischemia-reperfusion injury in the lower extremity causes dysfunction of many organs. In this study, we investigated the protective effects of alpha lipoic acid (ALA) on renal damage caused by infra renal ischemia reperfusion in rats. Methods: Animal model used in this study mimics post-operative complications caused by many aortic surgeries. In IR group blood delivery is occluded from the infrarenal area of the abdominal aorta with vascular clamp, after 30 minutes the clamp was removed and blood delivery was allowed for 2 hours. In SHAM group, only clamp was not placed. In IR+ALA group, ALA was injected (100mg/kg, i.p) for 3 days before the operation, then on the operation day the same procedure with IR group was performed. Animals in ALA group were only received ALA. In addition to hematoxylin-eosin staining, mouse monoclonal Bcl-2 and Bax antibodies are used for immune evaluation of kidney tissue sections with streptavidin-biotin-peroxidase method. Results: Histopathological evaluation revealed that the renal tissues of the SHAM group had normal structure. In the IR group, tubular lumen dilation, vacuolization, degeneration, and mononuclear cell infiltration were higher than those of the SHAM group. However no differences were observed in ALA group, in IR+ALA group, tubular degeneration, decrease in mononuclear cell infiltration and expansion of Bowmann’s capsule cavity is determined. Bcl-2 expression found higher in renal tubules of SHAM and ALA groups than IR and IR+ALA groups. The Bax expression were found to be increased in SHAM and ALA as compared with IR and IR+ALA group. Findings revealed that ALA has significant protective effects on abdominal ischemia-reperfusion induced renal tissue damage.
Keywords: Ischemiareperfusion, alpha lipoic acid, kidney, rat, immunohistochemistry
Ischemia defined as lack of oxygen in tissues or organs as a result of insufficient perfusion of organ and tissue due to arterial or venous blood flow reduction and causes cell death as a result of discharge of cellular energy storage and accumulation of toxic metabolites. Ischemic tissue requires re-blood flow to clear toxic metabolites and cell regeneration. However, reperfusion of ischemic tissue paradoxically results in more severe damage than ischemia-induced damage.[1]
Several factors have been proposed for the pathophysiology of ischemia-reperfusion injury. Although their relationship to each other is mixed, they are series of cellular and humoral events. Especially; four factors, including free oxygen radicals, polymorphonuclear leukocytes (PMNL), complement system and endothelial cells, are among the causes of damage.[2]
One of the most important organ systems involved in the internal balance of the body is the urinary system. Regulation of the volume and content of the body fluids, blood pressure, pH and regulation of water and electrolyte balance, the product of metabolism in the cells and the removal of them from blood are among the functions of the urinary system.[3] Kidneys are the most affected organ from ischemiareperfusion. Despite recent advances in medicine, various studies have been carried out to clarify and treat acute renal failure, and still remain important.[4]
Local and systemic effects of ischemia reperfusion are an important problem in vascular surgery. Acute ischemia-reperfusion injury in the lower extremities occurs especially in aortic surgery for transient crossclamping of the abdominal aorta and for single or bilateral acute femoral artery obstruction. Ischemia reperfusion injury during abdominal aortic surgery has local and systemic effects. Local effects are seen in the distal vein and muscle tissue, while systemic effects are seen in almost all organs including the brain, heart, lung, and kidneys. During periods of ischemia reperfusion, disruption of microvascular function triggers both the directly affected organ and the systemic inflammatory response, resulting in impaired endothelium-dependent dilatation of arterioles in distant organs. This pathological process involves increased fluid filtration and leukocyte plugs in the capillary bed, plasma proteins in the post capillary venules, and leukocyte extravasation.
These effects occur with increased oxygen radical production in all stages of microcirculation.[5] Repair and regeneration processes occur with cellular apoptosis, autophagy and necrosis, and the fate of an organ depends on if there is cell death or regeneration. Because of the reason that energy and protein synthesis is required for the realization of apoptosis, it occurs most after reperfusion.[6]
In our study, Bcl-2 and Bax protein staining were performed to determine the antiapoptotic factor in renal glomeruli and tubule cells. Bcl-2 oncoprotein inhibits apoptosis of endothelial cells and inhibits apoptosis, which ensures cell viability without causing cell proliferation.[7,8] Despite the fact that Bax protein has a high degree of structural similarity with Bcl-2, it shows proapoptotic activity.[9] Bax overexpression results in homodimerization and forms the heterodimer with Bcl-2 protein to inactivate it. This induces apoptosis as Bcl-2 function is inhibited[8,9]
Alpha Lipoic Acid (ALA), also known as thioctic acid, is a potent antioxidant that was discovered in the late 1980s.[10]
It was defined as vitamin in the first defined period. It is found in plant foods such as spinach, broccoli, tomatoes and animal foods such as liver, kidney and heart.[11] Nowadays, clinical use is becoming more widespread and it is subject to many scientific researches.
ALA comprises two oxidized or reduced sulfide molecules. This difference allows ALA to serve as the cofactor of many important enzymes. ALA can affect both oil and water-soluble oxygen radicals.
Both the oxidized and the reduced form of ALA show antioxidant activity. ALA administration has been shown to be useful in some of the oxidative stress associated models such as diabetes, ischemiareperfusion injury, cataract formation, HIV activation, and nerve degeneration and also radiation damage.[12–14]
With this study we aimed to investigate the possible protective effects of a strong antioxidant ALA on infra renal ischemia-reperfusion induced damage on kidneys.
Adult (2.5-3 months) male Spraque Dawley rats weighing 200-250 g were used in experiments. Animals were housed as 5 per cage at ambient temperature and humidity on 12/12h light/dark cycle. Food and water were given ad libitum to rats.
Animals were randomly divided to four groups. The first of these groups, called SHAM group, is the group in which the abdominal ischemia-reperfusion model is not applied. The second group; The IR group is the group in which the abdominal ischemia-reperfusion model is applied. The third group is the group called ALA group which is received daily injection of alpha lipoic acid (100 mg / kg, i.p.) for 3 days. The fourth group, IR+ALA group is the group in which alpha lipoic acid is injected daily (100 mg / kg, i.p.) starting from 3 days prior to the operation, followed by the same operation as the IR group.
Abdominal Ischemia-Reperfusion Injury Model In order to make abdominal ischemia-reperfusion injury model, rats were anaesthetized with intraperitoneal injection of ketamine (8 mg per 100 g of animal) and xylazine (1 mg per 100 g of animal) combination. During the experiments body temperature was maintained at 37oC using a heating pad (MAY RTC9404-A Animal Rectal Temperature Controller, Commat Ltd., Turkey) with a feedback of rectal probe. Abdominal region was prepared for surgery and a ~3 cm median incision was made. The infra renal region of the abdominal aorta was visualized with the help of a retractor. The peritoneal membrane was opened in order to reach the aorta, connective tissue was cleared and a vascular clip was inserted to completely block the blood flow. (Figure 1). In order to prevent loss of water from the peritoneum, the incision site was covered and waited for 30 minutes.
After the waiting period for ischemia, the clip was removed and abdominal blood flow was provided. The incision was sutured with 4-0 silk suture and the experimental animal was returned to normal living conditions for 2 hours. Following this reperfusion period, the experimental animal was anesthetized again by intra peritoneal injection of 8mg/100g of ketamine and 1mg/100g of xylazine and dissection was performed for the diaphragm isolation.
The experimental group in which this procedure was applied was named IR group. Same procedures were applied to SHAM group, except for the occlusion of abdominal aorta. Histological Techniques On the day after the last injection, the animals were sacrificed and their tissues were collected. For histological examinations, each kidney tissue taken in sufficient size was kept in a 10% buffered formaldehyde solution for 24-48 hours. After the fixation, 5 micrometer thick sections were taken from the tissue samples embedded in paraffin using a microtome. The sections were stained using Hematoxylin-Eosin staining method and examined by microscope.
For immune examination of kidney tissue sections, Murine monoclonal Bcl-2 (1:100 dilution) (C-2, Santa Cruz: 7382) antibody and Bax (1:100 dilution) (B-9, Santa Cruz: 7480) with murine monoclonal antibody to streptavidin-biotin-peroxidase method was used.
The evaluation of Bcl-2 and Bax immunostaining was performed in each renal tissue section by evaluating the immunostaining at 10 randomly selected areas in X40 amplification in light microscopy. (0; no staining, 1; weak, 2; moderate, 3; severe staining)
Ethical Issues All experimental protocols and steps of the tests were conducted in compliance with the regulations of the Research Ethics Committee of Necmettin Erbakan University Ethical Guidelines for the use of animals in research. Additionally, all animal experiments were in accordance with protocols approved by the United States National Institutes of Health (NIH, 1978). This study was also approved and supported by Ethics Committee of Necmettin Erbakan University Experimental Medicine Research and Application Center (Ref #118).
Statistical analysis Statistical comparisons between the groups were performed using the One-Way ANOVA and the Tukey’s post-hoc test after the data were checked for normal distribution with the Kolmogorov-Smirnov (K-S) test. The comparisons for the distributions that did not pass the normality test were done by KruskalWallis One-Way ANOVA and Duncan’s post-hoc test. Comparisons and tests were performed using the GraphPad Prism 5.0 Demo software. Data were given as mean ± standard error and p <0.05 was chosen for statistical significance.
Histopathological Evaluation
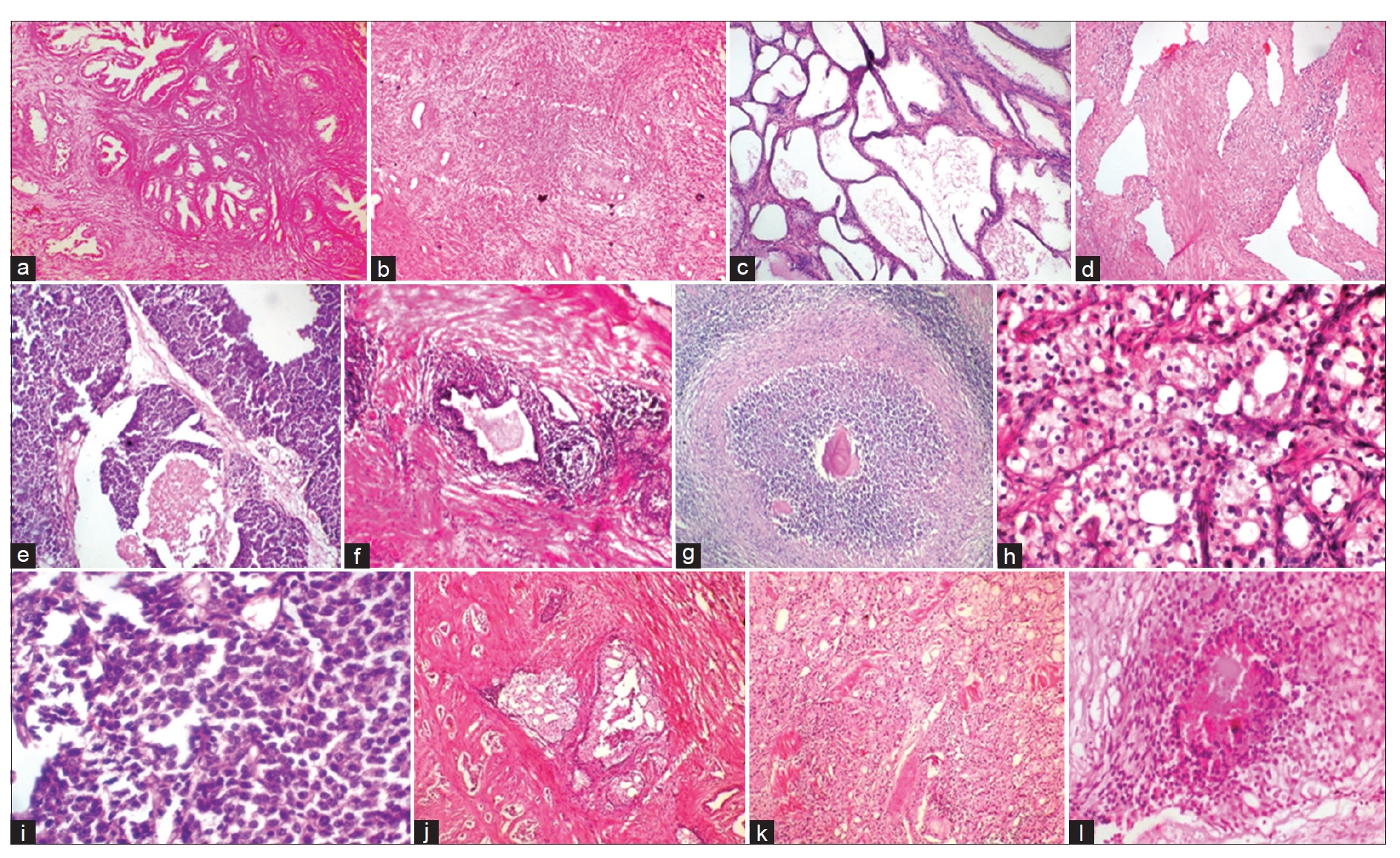
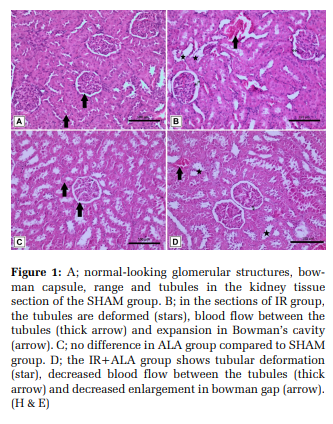
In the SHAM group, it was observed that the appearance of tubule cells in the renal cortexmedulla passage was normal, necrotic cells were not found in the renal tubules, there was no blood supply between the tubule cells and therefore there were no pathological finding (Figure 1 1A). In IR group, there was swelling of the tubule cells due to IR damage and consequently the accumulation of fluid in the tubules and tubular deformation due to the cells formed by cell debris. However, there was intense blood supply between the tubules. In addition to tubular damage, in a part of the renal bodies, enlargements were detected in the Bowman’s cavity due to glomerular atrophy (Figure 1).
There was no difference in ALA group compared to SHAM group, whereas in IR+ALA group, the tubular deformation continued but the blood supply between the tubules and expansion in Bowman’s cavity was decreased (Figure 1 1C and 1D).
Evaluation of Immunostaining
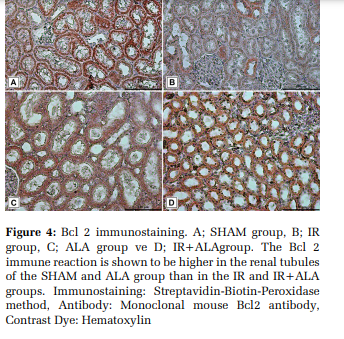
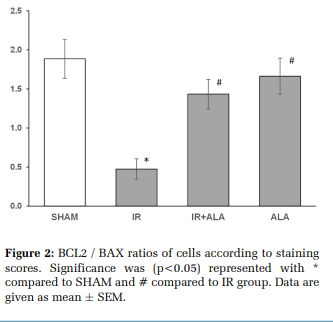
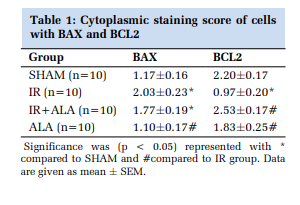
The Bcl2 immune reaction was found to be higher in the renal tubules of the SHAM and ALA group compared to the IR and IR+ALA groups (Figure 2 and Figure 4). Bax immune reaction was increased in IR and IR+ALA group compared to SHAM and ALA group (Figure 2 and Figure 3). Statistically, there was a significant difference between the IR and IR+ALA groups in terms of Bcl2 immune reaction, but there was no difference between the Bax immune reaction of the same groups (Figure 2 and Table 1).
In this study, we can say that abdominal ischemiareperfusion causes significant damage to kidney tissues in rats and these damages are significantly suppressed by treatment with ALA. Lipoic acid has been suggested to be a potential therapeutic agent in the treatment or prevention of different pathologies including diabetes, polyneuropathy, cataract and neurodegeneration.[14]
The main reason for the effectiveness of ALA on ischemia-reperfusion is the ability to remove multiple oxygen radicals, exhibit metal chelating activity and participate in the regeneration of ascorbate and vitamin E. Thus, the beneficial effects of a high LA dose on renal dysfunction and tissue injury in ischemic acute renal failure may be related to the suppression of increased renal ET-1 production induced by ischemia-reperfusion. This indicates that oxidant stress induces ET-1 production at any stage of gene expression. Therefore, ALA is thought to reduce over-production of renal endothelin (ET-1) due to oxidative stress during reperfusion.[15]
Aortic clamping during abdominal aortic surgery reveals an IR injury affecting the distal organs, including the kidney.[16] Restoring oxygen supply to the ischemic kidney results in ROS production.[17]
Excessive ROS formation causes lipid peroxidation in cell membranes and oxidative damage in DNA and proteins. These negativities increase in hyperoxia conditions and can lead to cell death.[16] Cell membranes containing polyunsaturated fatty acid residues of phospholipids are highly sensitive to oxidation. Therefore, lipid peroxidation of cell membranes is one of the important mechanisms of IR injury.[18]
Sehirli et al.[19] showed that, ALA could reduce tissue damage in the renal IR as in other organs. This effect was achieved by reducing the neutrophil infiltration, balancing the oxidant-antioxidant status and regulating the formation of inflammatory mediators. Bae et al.[20] showed that treatment with ALA increased creatinine clearance compared to untreated rats. ALA treatment also reduced the degree of polyuria that normalized sodium excretion.
The same authors reported that ALA treatment reduced the reduction of aquatic (AQPs) and sodium carriers in response to IR. All of the ischemiareperfusion models support the idea that ROS may be an appropriate target to reduce tissue damage from ischemia. However, it is likely that ALA activity and mechanisms of action may vary depending on each tissue and organ from which ROS is produced.[21]
In addition, ALA reversed the levels of all damage parameters and inflammatory mediators while preserving the kidney tissue against oxidative damage caused by reperfusion. Treatment with ALA significantly inhibits the development of acute renal failure (ARF) and results in normal renal function and normal kidney morphology.[15] These protective effects of lipoic acid in reperfusion-induced injuries, at least in part, inhibit neutrophil infiltration, may be based on oxidant-antioxidant status balancing and suggest that it may play a role in the treatment of IRinduced organ failure.[19] The administration of ALA to the animals exposed to ischemia-reperfusion injury, reduced the effects of reperfusion by decreasing the ROS level in brain cells compared to the control group, decreasing the dimensions of damage and prolonging the survival time of the animals. However, the efficacy of dihydrolipoic acid (DHLA) has also been shown to prevent reperfusion injury.[14,22]
In another study in which ALA activity against renal dysfunction due to ischemia-reperfusion was investigated, ALA given before and immediately after ischemia was observed to protect the kidney from ischemia-reperfusion induced damage such as impaired renal hemodynamics, urinary concentration and normalization of sodium excretion.[20] In a study by Şehirli et al.[19] , they used ALA (100 mg / kg, i.p.) to prevent renal ischemia reperfusion injury. They showed that tubular damage in kidneys caused by ischemia-reperfusion ameliorated significantly after ALA treatment.
In our study; while there was no difference between the SHAM and ALA groups, the IR+ALA group had tubular deformation, but the blood supply between the tubules and the expansion in the Bowman’s cavity was found to be reduced.
The kidneys are the target organ, especially in distant organ damage caused by lower extremity ischemia reperfusion caused by cross-clamping aorta from the infrarenal region. This is clinically important. The pathophysiology of renal damage after ischemia reperfusion is quite complex and a large number of mediators are involved. During the ischemia reperfusion, excessive amounts of free oxygen radicals are formed, causing oxidative stress. This may be due to changes in mitochondrial oxidative phosphorylation, decreased ATP, increased intracellular calcium, and activation of proteases and phosphotases leading to disruption of the cell skeleton and membrane phospholipids.[23] A certain ischemia time is required for the effects of experimental ischemia reperfusion injury in the kidneys. Paller et al. (1984) showed that reperfusion injury occurred in the rat kidney after 60 minutes of ischemia. In the same study, it was found that tissue damage occurred in 4 hours and reached its peak in 24 hours.[24] In our study, the 30-minute ischemia period was followed by a 120-minute reperfusion period. As a result of histopathological evaluation; n the SHAM group, it was observed that the appearance of the tubule cells in the renal cortex-medulla passage was normal, necrotic cells were not present in the renal tubules, there was no blood supply between the tubule cells and there was no pathological evaluation. In IR group, there was swelling of the tubule cells due to IR damage and consequently fluid accumulation in the tubules and tubular deformation due to cells formed by cell rashes. However, there was intense blood supply between the tubules. In addition to the tubular injury, a portion of the kidneys were observed in the Bowman’s cavity due to glomerular atrophy.
In their study, Özer et al.[25] Evaluated the renal damage after myocardial ischemia reperfusion with light microscope. In this evaluation, the kidney tissues of the control group showed normal histological features but they observed severe renal damage in the myocardial ischemia reperfusion group. Tubular dilatation and atrophy of these injuries were also noted as extensions in the Bowman’s cavity due to glomerular atrophy in some of the kidneys.
In a study performed by Ahmadiasl et al.[26] they applied a 45 min microvascular clamp to the left renal artery and vein and reperfused for 1 hour following ischemia. In the kidney tissues of the ischemia reperfusion group, dilatation, degeneration, dissection and mononuclear cells were observed to penetrate more than the SHAM group in the tubular lumen.
It consists of more than 26 different types of cells, such as multiple types of renal tubular epithelial cells, glomerular cells and interstitial cells. Renal cell types, which are the most affected by ischemia reperfusion, are endothelial cells and tubular epithelial cells. However, it was demonstrated that an extended ischemia followed by reperfusion would lead to loss of apoptosis or necrosis in all renal cell types.[27] In our study, Bcl-2 protein staining was used to determine the antiapoptotic factor in kidney glomeruli and tubule cells, and Bax protein staining was performed to determine the proapoptotic factor. It is known that Bcl-2 oncoprotein inhibits apoptosis of endothelial cells and inhibits apoptosis, which results in cell viability without causing cell proliferation. Bcl-2 also significantly reduces cell death induced by different stimuli.[8] Bcl-2 has been reported to prevent apoptosis by inhibiting caspases by direct and indirect mechanisms.[28]
Ito et al.[29] reported that Bcl-2 reduced cell death by free radicals. Fennell et al.[30] found that Bcl-2 formed this protective effect from the mitochondria by inhibiting the release of cytochrome-c and apoptosis-inducing factor (AIF) into the cytoplasm. Another mechanism of the antiapoptotic effect of Bcl-2 is the inhibition of Bax (bcl-2-associated x protein).[31] Bax is one of the members of the Bcl-2 family showing pro-apoptotic activity.[9] Yildar et al.[32] also showed that the severity of apoptosis increased in the kidney tissue where oxidative stress occurred after IR.
In our study, the Bcl2 immune reaction was found to be higher in the renal tubules of the SHAM and ALA group compared to the IR and IR+ALA groups. Bax immune reaction was increased in IR and IR+ALA group compared to SHAM and ALA group. Statistically, there was a significant difference between the IR and IR+ALA groups in terms of Bcl2 immune reaction, but there was no difference between the Bax immune reaction of the same groups.
However there are some limitations of our study about dose and time of injection of ALA. An exposure time and dose-response study can be performed by evaluating biochemical markers of oxidative stress in order to make better adjustments in dose and time.

Alpha lipoic acid in our study has been shown to prevent renal injury in the abdominal ischemiareperfusion model of rats. This result may give us new hope in preventing renal ischemia-reperfusion injury during aortic surgery.
Authors would like to thank to Prof. Dr. Nizamettin Dalkilic and Prof. Dr. Aydan Canbilen for their scientific comments and support.
Authors’ contribution
Burcu Gultekin and Seckin Tuncer designed the research. Ilksen Burat conducted experimental part of animal study. Burcu Gultekin made histological praperations and evaluation. Seckin Tuncer analyzed data and prepared the final draft of the article. All authors read and signed the final paper.
Subscribe now for latest articles and news.